
Research Article | DOI: https://doi.org/10.31579/2642-9756/108
1 MD, University of Health Sciences, Kanuni Sultan Suleyman Training & Research Hospital, Perinatology Clinic
2 MD, University of Health Sciences, Department of Microbiology, Istanbul Kanuni Sultan Suleyman Training and Research Hospital, Head of Blood Center , Istanbul , Turkey.
*Corresponding Author: Alev Atis Aydin, Obstetrician & Gynecologist University of Health Sciences, Istanbul Sarıyer Hamidiye Etfal Training & Research Hospital, Sarıyer, Istanbul/TURKEY.
Citation: Alev A. Aydin., Kamuran Sanli, Zuhat Acar, Sema S. Caypınar., Deniz Acar, et all (2022). Amniopatch Treatment in Spontaneous Previable Preterm Rupture of Membranes with Neonatal Outcomes. J. Women Health Care and Issues. 5(2); DOI:10.31579/2642-9756/108
Copyright: © 2022 Alev Atis Aydin, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 February 2022 | Accepted: 14 February 2022 | Published: 18 February 2022
Keywords: previable; premature rupture of membranes; amniopatch; neonatal
Objective: To evaluate the efficiency of amniopatch application in previable preterm rupture of membranes (pPPROM) between 17-23 gestational weeks of pregnancy.
Methods: 30 pregnants with previable preterm rupture of membranes were given amniopatch as therapy option instead of termination.After one week of antibiotics and bed rest the volunteers were applied amniopatch under sonographic guidance by infusion of 100 mL of 0.9% Isotonic solution alternate infusions of platelets, normal saline and FFP with a total of 100cc of each maximally were given into amniotic cavity. During infusion, in the event of bradycardia, the infusion was stopped.
Results: 38 amniopatches were applied to 30 pPPROM patients. 7 aborted, 17 gave an immature birth and 6 gave preterm birth None reached to term. Alive birth rate was %23, All of them were born prematurely with changing durations in Neonatal Intensive Care Unite (NICU). In the 7 alive newborns duration of NICU differed (10 days-91 days) with a mean of 44,5 days. Deepest vertical pocket normalized in only 4 of the 30 patients (13,3%) after one week. There were 2 ablatio plasenta cases, none born alive. Cesarean section rate was 6/30 (%20). Maternal complications were endometritis (5/30, 16%), chorioamnionitis 4/30 (13%) all cured with antbiotic regimens in one week, none had sepsis.
Conclusion: Results of amniopatch treatment in pPPROM are not convincing, although you restore the amnion a little bit, the etiopathogenesis and underlying factors still exist and cause premature birth, resulting in neonatal complications.
Premature (prelabor) rupture of membranes (PROM) is a rupture of the membranes before labor begins. If PROM occurs before 37 weeks of pregnancy, it is called preterm premature rupture of membranes (PPROM). PROM occurs in about 8 to 10 percent of all pregnancies. PPROM (before 37 weeks) accounts for one fourth to one third of all preterm births and is one of the major causes of preterm births [1] . However, the prognosis of PPROM before 24 weeks of gestation, is not favorable and is called previable PPROM (pPPROM) complicates about 1-4 /1000 pregnancies [2,3]. Neonatal outcomes and prognosis are not promising due to pulmonary hypoplasia, extremity defects like Potter syndrome and various complications [1,4]. Currently, there is no consensus regarding the optimal management for pPPROM. At this early gestational age they may be counseled about the potential risks and benefits of expectant management or the termination, with antibiotic therapy, steroid administration and/or tocolytic therapy [2,6]. Previable PPROM at this early stage of pregnancy occurs either iatrogenically (iPPROM) or spontaneously (sPPROM) [3,5]. Previable iPPROM may occur after chorionic villus sampling, amniocentesis or therapeutic procedures like shunt therapies [4,6]. Regardless of the type or etiology, the prognosis of pPPROM is not good.
The etiology of previable sPPROM is not identified but intrauterine infection is known to be the most common identifiable cause [5-8]. Even with the recent advances in obstetric and neonatal care, the survival rate of neonates born at less than 22–24 weeks of gestation ranges between 40–60% at best. Transabdominal amnioinfusion may be beneficial for preventing pulmonary hypoplasia and prolonging the latency period [9]. However, this treatment can not possibly seal the defect completely. Many experimental and clinical studies have been conducted in order to seal the defected membranes, including isotonic solutions, maternal blood, fibrinogen extract and evaluation of the amniopatch technique [9-12]. The amniopatch technique was first introduced by Quintero et al. [10] in 1996. It consisted of infusing a platelet concentrate and cryoprecipitate into the amniotic cavity which may form a blood plug and seal the defected site, as a result of platelet activation and fibrin formation [10,11]. The success rate of the amniopatch treatment varies from 10 to 60
This is a cohort study of women diagnosed with prevable sPPROM at 16–24 weeks of gestation between September 2017 and January 2019 at our Training & Research Hospital’s Perinatology Clinic, a tertiary-care referral hospital in Istanbul. This study was approved by the Institutional Review Board by the number of 2017-06-31.
The diagnosis of ruptured membranes was made by the presence of gross leakage and pooling of amniotic fluid in the vagina with positive nitrazine test or placental α microglobulin-1 test (amniosure). Gestational age was calculated based on CRL measurement made during the first trimester. Patients were placed for at least 2 -5 days of bed rest, in trial with expectation of spontaneous sealing of the membranes. During this waiting period, prophylactic antibiotic treatment, with iv cefazolin (1 g every 6 h) and oral azitromisin (500 mg 1x2) administration, and the daily amniotic fluid volume and fetal heart beat control was performed. If the amniotic fluid leakage persisted and the amniotic fluid volume continuously decreased, we counseled the patient about the potential benefits and risks and offered the following options: 1) active treatment with an effort to seal the ruptured membranes using the amniopatch technique; 2) expectant management with prophylactic antibiotics, antenatal corticosteroids and/or tocolytics; or 3) termination of pregnancy (TOP).
The amniopatch procedure was not offered as a treatment option to patients with regular uterine contractions or vaginal bleeding, cervical insufficiency, major fetal congenital anomalies, or signs or symptoms of clinical chorioamnionitis.
Clinical characteristics of patients before performing an amniopatch included age, parity, gestational age at PPROM. Factors associated with the procedures included gestational age at amniopatch, PPROM-to-delivery interval, maximal vertical pocket (MVP) before and after the procedure. MVP was used because the 4 quadrant assessment was not feasible in severe oligohydramnios.
Pregnancy outcomes included termination of pregnancy (TOP), fetal death, stillbirth, live birth, gestational age at delivery, delivery beyond 34 weeks of gestation, delivery beyond 37 weeks of gestation, PPROM-to-delivery interval, amniopatch-to-delivery interval, and clinical chorioamnionitis. TOP was done when pregnant woman refused to maintain the pregnancy. Fetal death was defined as no fetal heart beat while fetus is in the uterus.
Whereas stillbirth included all death of fetus including, death occurring with or immediately after birth. Clinical chorioamnionitis was defined as maternal fever of 37.8 °C or more plus one or more of the following signs: uterine tenderness, malodorous vaginal discharge, maternal serum WBC count of more than 15,000 cells/mm3 maternal tachycardia (>100 beats/min) and fetal tachycardia (>160 beats/min).
Neonatal outcomes of live-born neonates were birth weight, need of admission to the neonatal intensive care unit (NICU), and neonatal mortality.
We obtained written informed consent from each patient who chose the amniopatch treatment. Briefly, blood products were prepared using the transfusion protocol, and an ultrasound-guided amnioinfusion of the platelet concentrate followed by cryoprecipitate was performed Blood bank prepared the products of one unit of cross matched fresh frozen plasma (FFP) and one unit of platelets concentrate. After they came to room temperature, first amnioinfusion was performed using a 20- 22 gauge spinal needle after sterilization of the abdomen with povidone iodine. Prior to the procedure we excluded a subclinical infection by measurement of the C-reactive protein, procalcitonin and a white blood cell count. We usually gave a local anaesthetic and used a 22 G needle to access a safe location, devoid of umbilical cord. An infusion of 100 mL of 0.9% Isotonic solution was given to create a safe and clear pocket, which also permited better visualisation of the further procedure. Then alternate infusions of 20 mL of platelets, normal saline (which does not contain Calcium, needed for the clotting process), and 20 mL of FFP were given in order to avoide contact between the blood products and clotting in the lines. During infusion, the fetal heart rate as well as the accumulation of amniotic fluid were monitored by ultrasound. In the event of bradycardia, the platelet infusion was stopped and additional saline was used to dilute the active substances. Usually a total of around 100 mL of platelets, 100 mL of FFP and 150 mL of amnioinfusion fluid was used, because of slow infusion, the procedure could easily take up to 20 min. We usually offered one, maximally two attempts, if the initial ones did not cure amniotic fluid leakage. 8 patients had twice amnioinfusion, the others were applied only once.
On the following days, bed rest, prophylactic antibiotic therapy, and daily ultrasound monitoring for amniotic fluid volume were continued. Tocolytics and antenatal corticosteroid were administered when indicated. Primary outcome was no further additional amniotic fluid leakage and maintenance/increase of amniotic fluid volume after the treatment. Failure of amniopatch treatment was defined as continuous amniotic fluid leakage after the procedure and/or persistent oligohydramnios.
The proportions were compared using the x2 test or Fisher’s exact test as appropriate. The results were considered statistically significant when p values were <0>
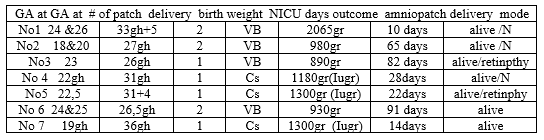
38 amniopatches were applied to 30 previable PPROM patients. 7 aborted, 17 gave an immature birth and 6 gave preterm birth (Figure 1). Demographic variables are shown in Table 1.
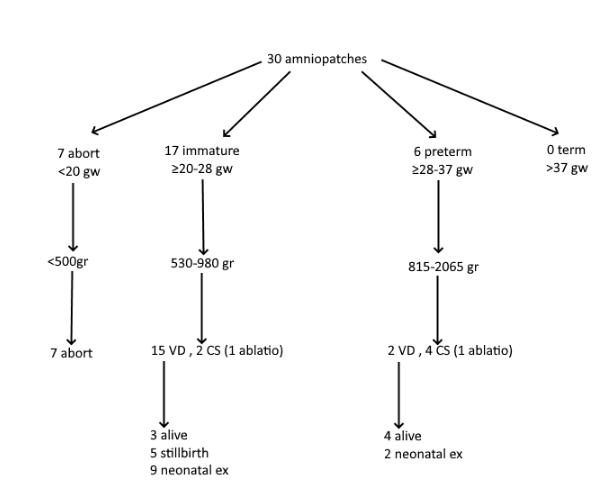

Alive birthrate was #, 2 patients out of 30 had ablatio plasenta (6,6%), 4 had chorioamnionitis cured totally with two antibiotics regimen, 5 had postpartum endometritis none were severe and were cured & discharged after 7 days of antibiotic therapy. Deepest vertical pocket was normalized (> 2,5 cm) in only 4 of the 30 patients (13,3%) after one week ( table 2).
In the 7 alive newborns, duration of NICU differed (10 days-91 days) with a mean of 44,5 days. All had normal neurodevelopment at 2 years of age.
Neonatal survival rate was #, none reached to term, all of them were born prematurely with changing durations in NICU (Table 2). Except 2 nonsevere retinopathies, none of them had bad outcome or complications but longer duration in NICU was hesitating both for parents and doctors in charge . Nearly all the vaginal deliveries were sudden and unexpected, except in induction of stillbirths .Amniopatch success were higher in group done after 20weeks compared with before. There were 2 ablatio plasenta cases, unfortunately none born live (one was at 25weeks 890 gr, the other 1390gr at 30 weeks. Cesarean section (cs) rate was 6/30 ( ) not high for these risky patients, .IUGR rate was high 3/7 (42.8%). Babies having retinopathy were cured with operation
PPROM is defined as a rupture of the fetal membranes prior to 37 weeks of completed gestation. This significant obstetric problem is directly related to 40 -50 % of all preterm births [2,8]. Specifically, spontaneous pPPROM is a disease of the fetal membranes in which inflammation-oxidative stress axis produces pathways that can lead to membrane weakening through a variety of processes. While there are several therapeutic options to reverse the rupture, it is highly difficult to reverse these processes. Therefore many of these aforementioned options (bedrest, antibiotics, amnioinfusion or amniopatch, endoscopic repair of rupture site etc.) are relatively unsuccessful [5-10].
Amniopatch for the treatment of sPPROM is less efficacious than the iPPROM ruptures. The reason for this is unclear but contributing factors may include the various underlying etiologies, the higher risk for infection and antenatal bleeding. In the amniopatch procedure, platelets are infused into the amniotic cavity together with the necessary clotting factors. Quintero reported a success rate of amniopatch used for iPPROM ranging from 65-80 % in two successive studies [10,11]. In a much lower finding, Richter et al. reported an amniopatch success rate of 58 %, and an overall live birth rate of 68% [18].Further evidence of the wide variation in success rate, Deprest reported that the procedure was successful in approximately 66 % of the iatrogenic ruptures included in the study. In 2017, Chmait et al evaluated the success rate of amniopatch in women with iPPROM, finding that PPROM occurred in 19 out of 1124 women who underwent laser surgery for TTTS. They reported a success rate of amniopatch in 63.2% of the women [17].
The membrane defects in iPPROM are usually well demarcated and relatively small, and the needles used are usually inserted high in the uterine cavity under sterile conditions.
In contrast, membrane defects in sPPROM are mostly large, poorly delineated, over or near the internal cervical os, and commonly associated with intra-amniotic infections [12]. Concomitant intra-amniotic infections may also cause an amniopatch procedure to fail, as bacterial fibrinolytic enzymes will cause rapid clot degradation, coexisting leukocytes may be activated and inflammatory reactions can then occur [18] . For these reasons, previous studies have found that the amniopatch procedure in sPPROM is far less effective . We reviewed the available literature to find cases of sPPROM treated with amniopatch but the treatment was only successful in a few cases [11, 15, 19]. Kwak et al. reported in his study that amniopatch treatment in spontaneous ruptures was successful in 1 out of 7 cases (14.3%). All except one were born prematurely and one had a mild disability. Other studies reported lower rates of complet healing of membranes with spontaneous rupture (11-14.3 %) [19-21].
Contino et al. and Ferianec both reported two successful cases delivered at 27 weeks [12] and 33 weeks of gestation [15], respectively. The periods of prolongation of the pregnancies were 4 weeks and 12 weeks, respectively.
Finally, Young reported successful treatment in none of the sPPROM cases but successful treatment in 3 out of 4 iPPROM cases [13].
In 2017, Sung et al performed a cohort study in to assess the risk factors of amniopatch in 28 women with iatrogenic or spontaneous PPROM between 15- 23 weeks of gestation. They reported successful procedures in 6 out of 28 women (21.4%) with iPPROM and only 2 out of 17 (11.8%) in women with sPPROM [20].
Maged et al. reported achieving complete sealing of membranes via amniopatch in 6 out of 50 (12%) women with sPPROM and restoration of the amion fluid index to the normal range in 22 out of 50 (44%) women. However the neonatal outcomes did not differ between the two groups [14,15].
Maged et al. also reported that their neonatal outcomes between the amniopatch group and expectant management group did not differ. There were no significant differences between the gestational ages at delivery, Apgar score at 1 and 5 minutes, NICU admission and duration of stay, perinatal mortality and neonatal complications in the two study groups. Futher, there was no statistical difference between women who underwent amniopatch and the control group regarding the mode of delivery, length of hospital stay or development of maternal complications. Our study confirmed that the neonatal outcomes of amniopatch are not favorable. This begs the question if the neonatal outcomes do not differ why perform amniopatch ?
We attempted to seal the ruptured membranes with an amniopatch technique in sPPROM patients, which was the largest study on amniopatch up till to now. We hypothesized that the degree of defects would be variable among previable sPPROM patients, and that few patients that would benefit from the amniopatch procedure. In this study, we reviewed 38 amniopatch procedures performed on 30 women with previable sPPROM at 17–23 weeks’ of gestation and compared the pregnancy outcomes of these cases with the controls who continued their pregnancies with conservative management. We found a neonatal survival rate of 23.3 % (7 out of 30 women) but 2 patients were at 24-25 weeks when their patches were applied. Thus our actual neonatal survival rate was lower at 16.6%. Among the survivors NICU admission rate was high,with a duration stay ranging (from 10-91days) (mean: 44,5 days) . None of the patients reached full term, with gestational weeks ranging from 26-36 (mean: 30,2 weeks) at birth. Two amniopatches were applied at 24 weeks, this may have affected their survival chance due to earlier pulmoner maturation. Mean fetal weights at birth was 1235gr (890-2065gr); 3 out of 7 were IUGR babies (42.8%). The deepest vertical pocket (> 2,5 cm) was normalized in 4 of 30 patients (13.3%). Further seven infants were born alive, which is consistent with the above studies. This means that although we restored the amniotic fluid in some cases, we could not build the same environment,- the same vascular network - in utero. The rate of NICU stay was high. In the 7 alive newborns duration of NICU differed (10 days-91 days) with a mean of 44,5 days. All had normal neurodevelopment at 2 years of age. But follow up of these newborns were challenging if they will be spastic or disabled because of prematurity. Two out of 7 had premature retinopathy fully recovered after operation fortunately. Although informed consent was taken for the possible complications & outcomes, families have hesitating moods when a complication occured as most premature babies had intracranial bleeding more or less due to prematurity but parents met these with a great grief .Thanks god they were all cured without a sequela. If they had sequela we would face with malpractis charges even though the parents had given informed consent previously. This is the largest study including 38 amniopatches on 30 patients, I could say instead of letting the fetuses to natural selection after PPROM, with amnipatch ,we drag them into prematurity complications or into a life with disabilities. Amniopatch just restores amnion may be temporarily but not the whole pathopysiology. According to above studies, although amniopatch helped in some cases, the fact is not normalisation of amnion quantitively actually. At the end most delivered preterm and were subjected to neonatal complications. Fortunately maternal complications were not severe, 4 chorioamnionitis cases responded to antibiotics .We also had not sepsis or life threatening complications just as the studies reported no increased risk for maternal complications,
Because of all these factors, amniopatch should not be recommended in spontaneous previable preterm premature rupture of membranes but should be reserved for iatrogenic cases.
Limitations of this study is that we could compare amniopatch group with expectant group in previable PPROM cases, but it is obvious that the results are not promising in both groups in observational studies.Further studies would approve our results.
Amniopatch treatment in pPPROM may help in minority of cases but it never heals the underlying factors that cause preterm birth.
We thank to perinatology staff including fellows, nurses, personels, blood bank staff, assistants and all residents on shifts.
None
None
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
