
Review Article | DOI: https://doi.org/10.31579/IJBR-2021/058
Professor and clerkship director of Emergency Medicine, California Northstate University, Elk Grove, California, USA.
*Corresponding Author: Professor and clerkship director of Emergency Medicine, California Northstate University, Elk Grove, California, USA.
Citation: Ma, V.X.T, Sauer, A.J., and Ranasinghe, L. (2022) Amiodarone versus Lidocaine Therapy in the Adult Cardiac Arrest Algorithm for VF/pVT/PEA/Asystole. International J. of Biomed Research. 2(3): DOI: 10.31579/IJBR-2021/058
Copyright: © 2022, Leonard Ranasinghe, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 January 2022 | Accepted: 13 January 2022 | Published: 22 January 2022
Keywords: cardiac; algorithm; amiodarone; lidocaine
Out-of-hospital cardiac arrests claim more than 300,000 lives each year in North America. The time of arrest plays a crucial role in the success of resuscitative efforts, as survival rates with favorable neurologic outcomes rapidly declines after about 16 minutes of cardiopulmonary resuscitation (CPR) [1].
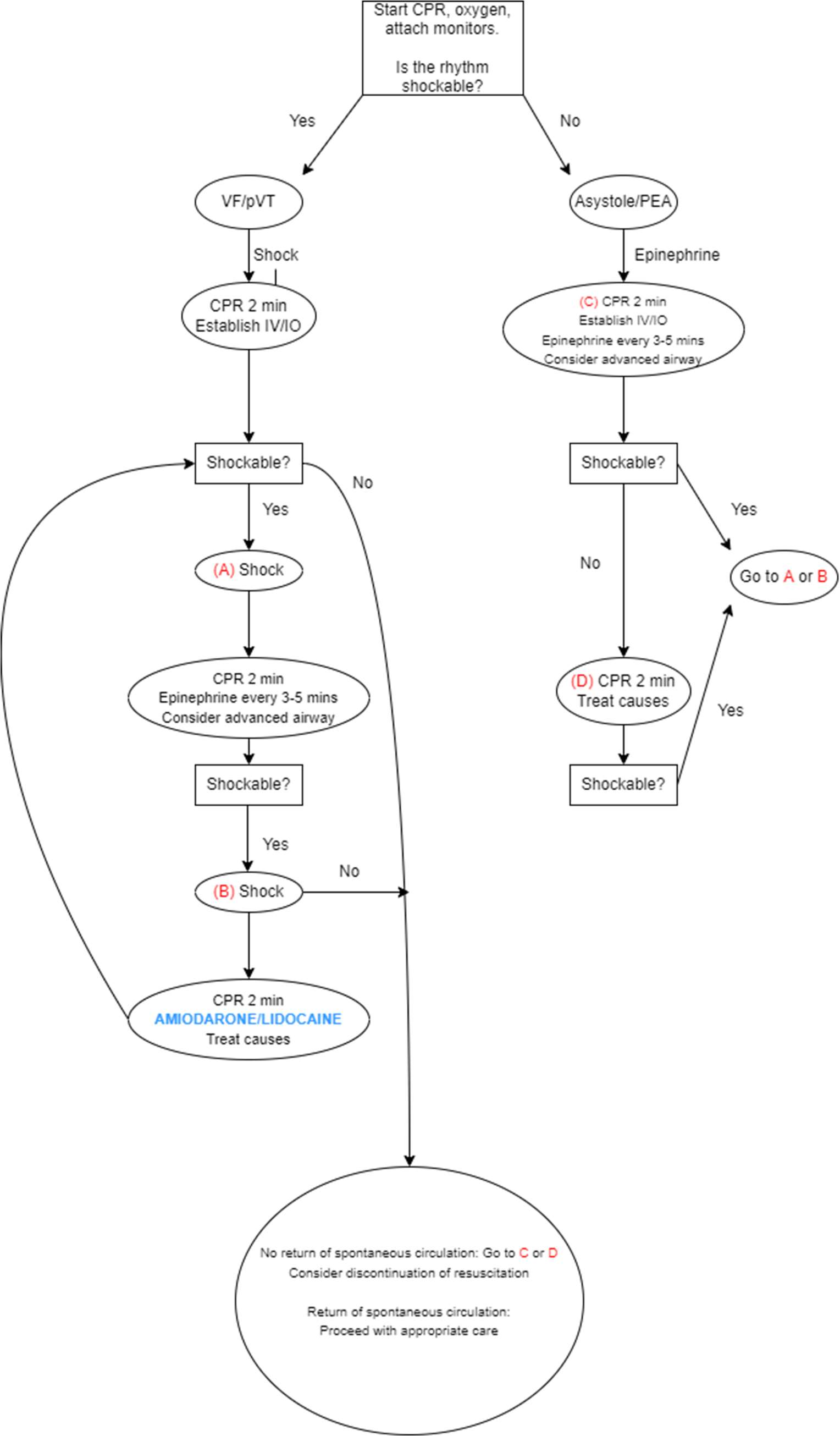
Antiarrhythmic agents are widely used in out-of-hospital cardiac arrests for shock-refractory pulseless electrical activity or ventricular fibrillation, but current data fails to show any proven benefits to survival in these patient groups. In 2015, the American Heart Association updated the Advanced Cardiac Life Support (ACLS) algorithm to include class III antiarrhythmic IV amiodarone 300 mg bolus first dose with subsequent 150 mg doses or the alternative class IB antiarrhythmic IV lidocaine 1.0 to 1.5 mg/kg first dose with subsequent 0.50 to 0.75 mg/kg doses for sustained ventricular fibrillation (VF) or ventricular tachycardia (VT) fractious to CPR, vasopressors, and defibrillation in the out-of-hospital setting. In the absence of contraindications and other factors in a patient’s history (allergies, adverse reactions, etc.), it may be difficult for a healthcare provider to decide which treatment may be more beneficial for any given patient during an emergent situation, whether in-hospital or out-of-hospital. Given that increasing number of shocks is associated with a decreased likelihood of survival [2], it stands to reason that it is paramount for a provider to promptly administer the most effective treatment in these critical moments. Many studies have been published since then comparing the two treatments, with several in 2016 raising the question of whether or not these treatments are even effective to begin with. This article will serve as a mini review of current literature comparing the efficacy of amiodarone and lidocaine as used in the ACLS algorithm since the 2015 update.
The most oft-cited study when it comes to this conundrum is the Amiodarone, Lidocaine, or Placebo (ALPS) study of 3,026 patients, published by the Resuscitation Outcomes Consortium in 2016, which assessed the efficacy of amiodarone (974), lidocaine (993), or saline placebo (1059) administration by paramedics in non-traumatic out-of-hospital cardiac arrests with focus on proportion of those who survive to hospital discharge. In short, neither amiodarone nor lidocaine resulted in statistically significant improvements in hospital to discharge survival compared to placebo, citing 24.4% versus 23.7% versus 21.0% respectively [3]. Amiodarone recipients more frequently required temporary cardiac pacing compared to lidocaine or placebo. Neurologic outcomes post-discharge were similar amongst all 3 groups. Although these treatments yielded significantly higher survival rates before hospital admission in bystander-witnessed arrest, there was no clear benefit in unwitnessed arrests, reinforcing the urgency for prompt antiarrhythmic therapy. In emergency professional-witnessed cardiac arrest, survival rates to discharge with amiodarone more than doubled compared to placebo. For amiodarone, the difference in survival rate vs placebo was 3.2% (P=0.08), while for lidocaine, the difference was 2.6% (P=0.16). For amiodarone versus lidocaine, an even smaller difference was noted, sitting at 0.7% (P=0.70).
These findings were touched upon in Sugiyama’s subsequent discussion on the necessity of amiodarone/lidocaine in August of 2016 [4], raising the question of whether these medications are truly effective. The study also found the rate of return of spontaneous circulation (ROSC) to be significantly higher with lidocaine than placebo, 39.9% versus 34.6%, with amiodarone showing less efficacy than lidocaine at 35.9%.
Several additional small studies have since been published, which may shed further light on the topic. In the United States, IV amiodarone is available in 2 approved formulations; one containing the vasoactive solvent polysorbate that has potential to cause hypotension, and the other including non-vasoactive captisol. In 2 distinct out-of-hospital, randomized controlled studies exploring adults with shock-refractory VF/pVT who received at least 3 shocks and epinephrine, amiodarone championed both lidocaine and the placebo [5]. The first study compared 246 patients who received amiodarone to a 258 patient placebo group and revealed the 300 mg bolus of polysorbate amalgam improved survival to hospital admission compared to placebo, with an odds ratio (OR) of 1.6 and 44% survival versus 34% respectively (P=0.03) [6]. The other study analyzed 347 patients treated by paramedics within 25 + 8 minutes since cardiac arrest and found amiodarone yielded 22.8% of 180 patients surviving to hospital admission versus 12.0% of 167 patients given lidocaine (P=0.009; OR 2.17, 95% CI 1.21 to 3.83). If these patients were treated equal to or less than the 24 minute median medical intervention time, amiodarone still showed consistently higher survival rates at 27.7% versus lidocaine at 15.3% (P=0.05) [7]. While these studies both show promising efficacy for amiodarone, they were both conducted nearly 2 decades ago and may be unreliable given the rather long EMS response time, sparking necessity for a more current and expansive study to elucidate the preference for this drug over lidocaine.
In 2020, a retrospective study on 130 patients compared the efficacy of an amiodarone-first strategy vs lidocaine-first strategy, ultimately noting that the amiodarone-first group had a higher likelihood of terminating the aberrant rhythm within 3 shocks [8]. There were no differences, however, between the two treatments in 24h survival, ROSC, or favorable neurological outcomes. Additionally, this study was fairly limited in its statistical power given the small sample size, as well as the fact that 113 patients were used for the amiodarone-first strategy compared to 17 for lidocaine.
Though additional information is available, the consensus on this topic has changed minimally. The studies cited can also be interpreted in a variety of ways, in both the acute and post-discharge setting. Procedure bias may exist in the large-scale 2016 analysis of 3,026 patients, as this study did not standardize hospital care, suggesting possible treatment imbalances between therapy groups, however the trial was blinded, randomized, and the frequencies of coronary catheterization, therapeutic hypothermia, and discontinuation of life-sustaining regimens did not substantially differ between these groups. Because amiodarone and lidocaine are both noted to improve survival rate to the hospital, the updated ACLS protocols certifies readily improved survival rates by allowing emergency medical personnel administration of amiodarone or lidocaine in witnessed cardiac arrests [3]. However, there still appears to be no significant impact on overall outcome to hospital discharge and beyond, as supported by a 2017 meta-analysis of 8 RCTs involving 4,464 patients [10] as well as 2018 systematic review 14 RCTs and 17 observational studies [9], warranting further larger-scale studies on the topic.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
