
Case Report | DOI: https://doi.org/10.31579/2690-4861/350
1 Clinical Hospital Centre Sestre Milosrdnice, Clinic for Surgery, Zagreb, Croatia.
2 Private Orthopaedic Surgery Clinic Marinko Erceg Pty. Ltd., Split, Croatia.
3 General Hospital Šibenik, Šibenik, Croatia.
4 Clinical Hospital Center Split, Surgery Clinics, School of Medicine, University of Split, Croatia.
*Corresponding Author: Marinko Erceg, Private Orthopaedic Surgery Clinic, Marinko Erceg Pty. Ltd., Split, Croatia.
Citation: Erceg D., Erceg M., Bečić K., Bekavac J., (2023), Aloarthroplasty of the Hip After Pathological Fracture of the Right Femoral Neck and Right Femoral Dyaphysis and Osteosynthesis after Fracture of the Left Femoral Dyaphysis in 41-Year-Old Female Patient with Polyostotic Fibrous Dysplasia? Case Report, International Journal of Clinical Case Reports and Reviews, 15(2); DOI:10.31579/2690-4861/350
Copyright: © 2023, Marinko Erceg. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 10 November 2023 | Accepted: 30 November 2023 | Published: 11 December 2023
Keywords: fibrous dysplasia; pathological femoral fracture; hip aloarthroplasty
A 41-year- old female patient with pathological basicervical right femoral neck fracture and fractures of both femoral bones 15-20 cm distally from the small trochanter is presented. Skeletal scintigraphy was performed and multiple pathological accumulations of radioactive substances were found in almost the entire locomotor system. First, we implanted a partial biarticular hip prosthesis with long stem in right femur, and one year later osteosynthesis of the left femoral diaphysis was done. Pathohistological examination did not find tumor cells and polyostotic fibrous dysplasia also was not clear. Our patient had not problems with bones earlier and she was never treated for this disease, except surgery of femoral fractures. Today, 11 years later the patient is in good general state, she has no pain in her legs and fractures of femur bones healed completely. We did not find a case in literature that a two fractures of proximal right femur bone (femoral neck and proximal diaphysis) and fracture of the left femoral diaphysis were solved with long stem prosthesis, and osteosynthesis of another femoral bone in patient who, we believe, has fibrous dysplasia and was never treated for this disease.
Bone fractures without significant trauma can imply pathological fractures, especially when they occur on multiple locations. In adults we primarily consider tumor metastases, multiple myeloma and polyostotic fibrous dysplasia, although this disease is often detected in younger age. It is a developmental bone formation disorder during skeletal growth in which the marrow is replaced by fibrous tissue [1]. Clinical signs can occur at any age, usually around 30 years of age [2]. It is a benign formation and about 5-7% of all cases of benign tumors are fibrous dysplasia. Disease is more commonly reported in its monocystic form, in adolescents and young adults, and less often occurs as a polycystic form, usually in children below 10 years of age [3]. This disorder may also be associated with hormonal disorders (Albright syndrome), [1,4]. Most commonly affected are femur (thighbone), tibia (shinbone), humerus, and skull, ribs and pelvis. In adulthood, in some patients, the first clinical manifestation is pain or pathological fractures, with the patient reporting never having any problems before, or knowledge of fibrotic dysplasia. This was the case here. The scintigraphy of the locomotor system and the biopsy should also be performed. In the polyostotic form with fibrous dysplasia, we should also consider the multiple myeloma / plasmocytoma, as well as multiple bone metastases. Orthopedic-surgical treatment of long-bone fractures of patients with fibrous dysplasia consists of curettage, bone transplants, osteosynthesis of fragments, and in adults with proximal femur fractures hip prostheses are implanted [5,6].
A 41-year- old female patient A. N. with pathological basicervical right femoral neck fracture and infraction of both femur bones 15-20 cm distally from the small trochanter came to our Department in April 2007., (figure 1). She was limping on her right leg and had pain almost one year in her right hip and thigh, but also in left thight, although smaller. She could not remember any trauma in last year or earlier, as she did not know for any problems with her bones. The pain had not started suddenly, but slowly. Skeletal scintigraphy showed pathological collections on mentioned fractured locations on both femurs, as well on the spine, both shoulders, cranium, neck and both feet (figure 2).

Figure 1: X ray of the pelvis and proximal femur bones with pathologic fractures of the right femoral neck and infraction of both femoral diaphysis. Figure 2: Scintigraphy of the bones shows multiple places of radioactive activities.
We considered multiple myeloma (plasmocytoma) but this suspicion was not confirmed by hematologist. Surgical treatment was undertaken and patient had partial biarticular cementless prosthesis with long stem implanted, that served as intramedullar nail for the imobilisation of the femoral diaphysis fracture (figure 3).
Biopsy from the fracture location was taken for patohistology from the femoral neck. PHD didn't confirm plasmocytoma and neither did the control haematological analysis, including the cytology of the bone marrow. No other metastatic tumor cells were found. The result was described as „fibrous altered bone marrow“. After the rehabilitation the operated leg functioned normally. During the next year the patient started limping on her left leg. Beginning of 2009. osteosynthesis of the left femur was performed (figure 4,5). The biopsy result was also negative on tumor cells, and fibrous dysplasia wasn't confirmed with certainty. Regular check-ups showed normal bone healing on both femoral bones as well as normal function and the patient was feeling well.

Figure 3: X ray of the pelvis and proximal femurs after implantation of cementless partial biarticular hip prosthesis with long stem. Infraction of the left femur is well seen. Figure 4: X ray shows pathologic fracture of the left femoral diaphysis and bone angulation. Figure 5: X ray after osteosynthesis of the left femur bone.
Scintigraphy of the bone in late 2015. showed pathological collections only on the knees, 10th and 11th rib on the back and left hip. Fracture locations were clean and the collections on the cranium, spine and feet have completely diasppeared (figure 6).
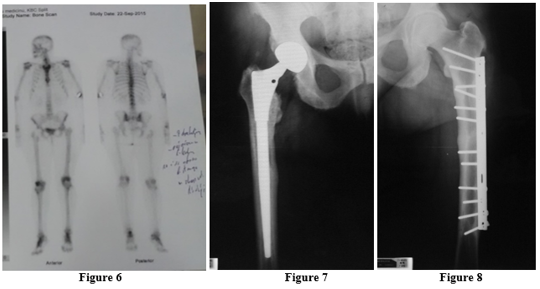
Figure 6: Scintigraphy of the bones 7 years after surgery. Figure 7: X ray of the right hip and femur, present time. Figure 8: X ray of the left femur, present time.
X-ray images from late 2017. showed completely healed fractures of both femurs with normal bone structure as well as the position of the right hip prosthesis (figure 7,8).
Authors considered this case interesting as it was peculiar that the first problems that patient reported were at the age of 40. Apart from the surgical treatment she never took any medication (bisphosphonates or similar) but the number of pathological collection sites was significantly reduced. Operated femurs are completely healed and the prosthesis works perfectly. The patient’s condition is well and does her check-ups every few years. Even it wasn’t confirmed by PHD we believe that this was the case of polyostotic fibrous dysplasia.
The author declares no competing interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
