
Case Report | DOI: https://doi.org/10.31579/2641-0419/366
1Internal Medicine department Corwell Health East Dearborn.
2Cardiology Department Corwell Health East Dearborn.
3Internal Medicine Department Mclaren Flint Hospital.
*Author Note: Mohammad Ali Mozaffari and Khurram Arshad are equal contributors and share the co-first authorship.
*Corresponding Author: : Khurram Arshad, Internal Medicine Department Corwell Health East Dearborn
Citation: Mohammad A. Mozaffari, Khurram Arshad, Rabia Latif, Farman Ali, Yazan Alamro, et.al (2024), All in One: Anomalous Coronary Arteries Arising from the Right Cusp, J Clinical Cardiology and Cardiovascular Interventions, 7(4); DOI: 10.31579/2641-0419/366
Copyright: © 2024, Khurram Arshad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 April 2024 | Accepted: 26 April 2024 | Published: 02 May 2024
Keywords: anatomy; cardiology; chest pain; and coronary vessels
Background: Coronary artery anomaly (CAA) refers to structural abnormalities affecting the coronary arteries and, in most cases, are rare congenital defects affecting almost 1% of the general population. These malformations can vary in presentation, ranging from benign variations to potentially life-threatening anomalies. Anomalous coronary arteries arising exclusively from the right coronary cusp (RCC) represent a rare occurrence with an estimated incidence of approximately 0.03-0.2% in the general population.
Case Report: We are presenting a case of a 73-year-old male with a past medical history of coronary artery disease with prior coronary artery bypass surgery who came to the emergency department with chest pain. Given his ongoing symptoms, he was taken urgently to the Cardiac Cath Lab. He was found to have anomalous coronary arteries, all arising from the right coronary cusp. He has a chronic total occlusion of the right coronary artery (RCA) at the proximal segment with the faint right to right collaterals coming from the RV branch, 100% circumflex occlusion, with the left anterior descending artery (LAD) coming off from the proximal RCA that was diffusely diseased but patent, he had an antegrade filling and competitive flow from the left internal mammary artery (LIMA).
Conclusion: Understanding this anomaly's anatomical variations and potential hemodynamic consequences is crucial for accurate diagnosis, appropriate management, and optimizing patient outcomes. Management strategies for coronary artery malformation depend on the specific anatomical and functional characteristics and the presence or absence of symptoms. Treatment options may include medical management, lifestyle modifications, interventional procedures, or surgical intervention.
Coronary artery anomaly (CAA) refers to structural abnormalities affecting the coronary arteries and, in most cases, are rare congenital defects affecting almost 1% of the general population. [1-6] These malformations can vary in their presentation, ranging from benign variations to potentially life-threatening anomalies [7]. Anomalous coronary arteries arising exclusively from the right coronary cusp (RCC) represent a rare occurrence with an estimated incidence of approximately 0.03-0.2% in the general population [8]. In this intriguing anomaly, all coronary arteries, including the left main coronary artery (LMCA), left anterior descending artery (LAD), and circumflex artery (CX), originate from the RCC, deviating from the usual anatomical distribution [9]. Understanding this condition's unique anatomical variations and potential hemodynamic consequences is essential for accurate diagnosis, appropriate management, and optimizing patient outcomes.
A 73-year-old male with a past medical history of coronary artery disease with prior coronary artery bypass surgery came to the emergency department with chest pain. He had ongoing symptoms for approximately 4 to 5 days before the presentation. Initial troponin was 2.43, and EKG showed diffuse ST segment depression. Given his ongoing symptoms, he was taken urgently to the Cardiac Cath Lab. He was found to have anomalous coronary arteries, all arising from the right coronary cusp. He has a chronic total occlusion of the right coronary artery (RCA) at the proximal segment with the faint right to right collaterals coming from the RV branch, 100% circumflex occlusion, with the left anterior descending artery (LAD) coming off from the proximal RCA that was diffusely diseased but patent, he had an antegrade filling and competitive flow from the left internal mammary artery (LIMA). All 3 vein grafts were occluded. The vein graft to the RCA was occluded at the ostium, which was likely the culprit for the non-ST-elevation myocardial infarction. The intervention was attempted on the vein graft to the RCA, with attempted thrombectomy and balloon angioplasty, but failed to restore flow through the graft. The patient was admitted to the surgical ICU with an intra-aortic balloon pump in place. Given that he would need CTO intervention to the native right coronary artery, he was transferred to a higher level of care for intervention.

Figure 1: LAO 22O CRA 1.30 view showing total of the native RCA (thin arrow) LAD arising from proximal RCA (think arrow)
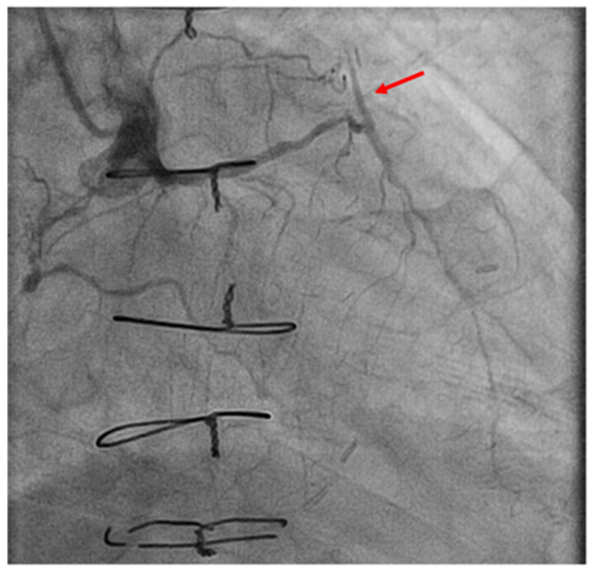
Figure 2: RAO 27.20 CRA 3.00 view showing antegrade filling of the LIMA graft
Coronary artery malformation encompasses structural abnormalities affecting the coronary arteries, essential for supplying oxygenated blood to the heart muscle [6]. These malformations
exhibit a broad spectrum of presentations, ranging from benign variations to potentially life-threatening anomalies [10]. A comprehensive understanding of coronary artery malformation is paramount in facilitating accurate diagnosis, implementing appropriate management strategies, and ultimately improving patient outcomes.
The aetiology and pathogenesis of coronary artery malformation are multifactorial and complex. While some cases may be congenital, others may develop due to acquired conditions or genetic predisposition. These anomalies can involve various aspects of coronary artery anatomy, including anomalies in origin, course, branching patterns, and luminal narrowing or dilation [9].
The clinical manifestations of coronary artery malformation can vary widely, ranging from asymptomatic individuals to those experiencing symptoms such as chest pain, shortness of breath, or even life-threatening cardiac events. Timely diagnosis through various imaging modalities, including coronary angiography, computed tomography angiography (CTA), or magnetic resonance imaging (MRI), is crucial for accurate characterization and appropriate management [10].
Management strategies for coronary artery malformation depend on the specific anatomical and functional characteristics and the presence or absence of symptoms. Treatment options may include medical management, lifestyle modifications, interventional procedures, or, in severe cases, surgical intervention [11].
Understanding this anomaly's anatomical variations and potential hemodynamic consequences is crucial for accurate diagnosis, appropriate management, and optimizing patient outcomes. Management strategies for coronary artery malformation depend on the specific anatomical and functional characteristics and the presence or absence of symptoms. Treatment options may include medical management, lifestyle modifications, interventional procedures, or surgical intervention.
Self Funded
It is not applicable as the patient's name or any identification is not mentioned in our case
None Declared
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
