
Case Report | DOI: https://doi.org/10.31579/2641-0419/134
1Department of interventional cardiology, Ziekenhuis Oost-Limburg, Genk, Belgium
2Department of interventional cardiology, Belfast City Hospital, Belfast, United Kingdom
*Corresponding Author: Jo Dens, MD, PhD Department of interventional cardiology Ziekenhuis Oost-Limburg Schiepse bos 6, 3600 Genk, Belgium
Citation: Ief Hendrickx, Bert Ferdinande, Colm Hanratty, Jo Dens, (2021) Algorithm for Recanalization of Chronic Totally Occluded (CTO) Native Coronary Arteries Through a Diseased or Occluded Saphenous Vein Graft in Post Bypass Patients.. J. Clinical Cardiology and Cardiovascular Interventions, 4(2); Doi:10.31579/2641-0419/134
Copyright: © 2021 Jo Dens, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 27 January 2021 | Accepted: 02 February 2021 | Published: 09 February 2021
Keywords: percutaneous coronary intervention; recanalization; chronic total occlusion; saphenous vein graft; coronary artery bypass graft
Chronic total occlusion (CTO) desobstruction of a native coronary artery in a post coronary artery bypass graft (CABG) patient can be a challenging procedure. In principle, the 3 basic approaches of recanalization of occluded native coronary arteries can be used: antegrade wire escalation (AWE), antegrade dissection re-entry (ADR) and a retrograde technique. On the other hand, a previous implanted saphenous vein graft (SVG) – even when occluded – can be used as a conduit for retrograde access. Moreover, access through a graft might be less complex compared to the use of septal or epicardial collaterals. If the graft is still open or has a tapered stump, this should be considered as a suitable conduit. Literature on recanalization of occluded native coronary arteries trough a diseased or occluded SVG is limited. A flowchart with an algorithm in post CABG patients is proposed and illustrated by 3 clinical cases.
Indexing words: angiography; coronary interventions; calcified stenosis.
Running title: Recanalization of chronic totally occluded native coronary arteries
About 30 years ago, Kahn and Hartzler performed the first percutaneous coronary intervention (PCI) through a saphenous vein graft (SVG) on a native coronary artery [1]. Although these landmark procedures were done a long time ago and many has changed regarding techniques and available materials, chronic total occlusion (CTO) desobstruction of a native coronary artery in a post coronary artery bypass graft (CABG) patient remains a challenging procedure [2,3].
Recanalization of an occluded coronary artery, by using a retrograde approach has significantly improved procedural success rates [4,5]. The most common retrograde conduits are septal collaterals followed by epicardial collaterals. Diseased or occluded SVGs are also suitable for retrograde access in CABG patients, but literature on these procedures is limited.
CTO desobstruction of a native coronary artery which is bypassed by a diseased or occluded SVG can be performed by the three conventional techniques: antegrade wire escalation (AWE), antegrade dissection re-entry (ADR) and by a retrograde technique (Figure 1).
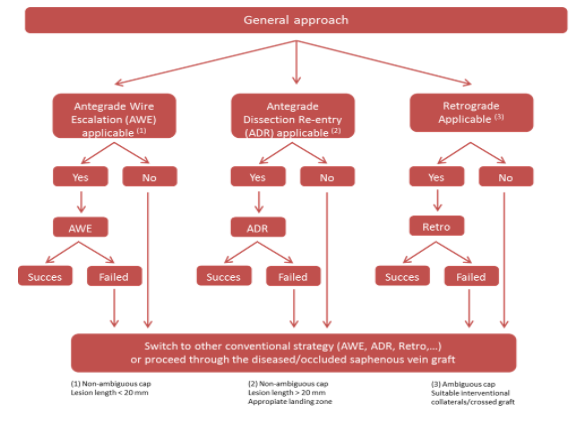
In function of the lesion characteristics (ambiguous or non-ambiguous cap, occlusion length and quality of the landing zone) different techniques are applied. AWE is mainly used in short lesions (< 20 mm length) with a non-ambiguous cap. ADR is mainly used in longer lesions ( > 20 mm length) with a non-ambiguous cap and an appropriate landing zone, whereas a retrograde technique is preferred for lesions with an ambiguous cap in the presence of suitable interventional collaterals (septal or epicardial) or graft (both arterial and venous). If present, SVG gain preference above septal and epicardial collaterals because of easier crossability, less tortuosity, larger caliber and less risk of perforation [6].
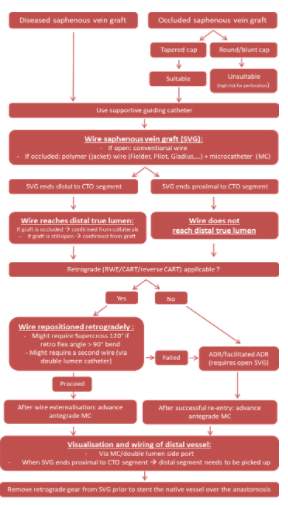
In case the SVG is occluded, usually the distal segment is visualized by collaterals. In case a retrograde approach is needed, access through the diseased or even occluded SVG is an additional option (Figure 2), especially when the collaterals are poorly developed or non-suitable for crossing with a wire or a microcatheter. If the graft is still open or diseased (with tapered stump), this graft should be considered as a suitable conduit and therefore can be used as for facilitated ADR.
Case series
The first case is a 73-year old male who presented with peri-operative ischemia during transurethral resection of the prostate (TURP). The electrocardiogram (ECG) showed diffuse ST-depression in all leads and ST-elevation in aVR with mildly elevated high-sensitive troponine T (19 ng/L, cut-off < 14). Transthoracic echocardiography (TTE) showed preserved left ventricle function (visual estimation about 60%) with no regional contractility abnormalities.
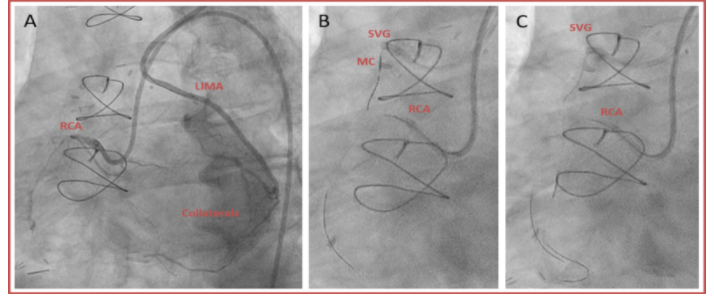
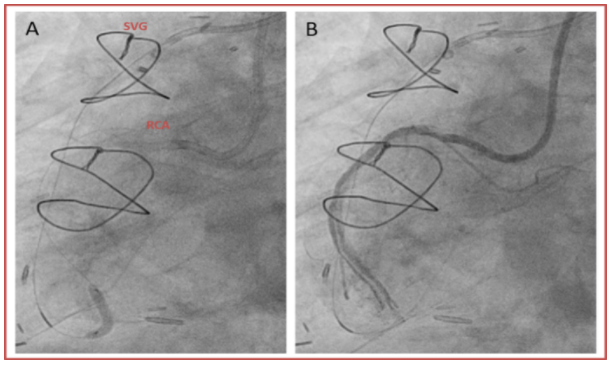
The patient was known with diabetes mellitus, peripheral arterial disease and coronary artery bypass graft (CABG in 2002) with left internal mammary artery (LIMA) on the 2nd lateral branch of the circumflex (L2Cx), right internal mammary artery (RIMA) on the left anterior descending artery (LAD) and saphenous venous graft (SVG) originating from the aorta to the right coronary artery (RCA). Coronary angiography showed patency of the LIMA-L2Cx and RIMA-LAD. There was a CTO of the RCA and also a CTO of the SVG to the RCA (duration of occlusion of SVG unknown). There were epicardial collaterals originating from the Cx to the inferolateral (IL) branch from the RCA (Figure 3A).
Because of the presence of ischemia and preserved contractility of the inferior wall on TTE, CTO desobstruction was planned. Double arterial access was implemented with use of supportive guiding catheters. Contrast injection of the LIMA was performed by 6 French (Fr) IMA guiding catheter through the left radial artery. Contrast injection of the RCA was performed by 7 Fr AR II through the right femoral artery. Because of unsuitable interventional epicardial collaterals from Cx to the IL-branch, we switched from the LIMA to the occluded SVG (the SVG was injected by 6 Fr AL 0.75 guiding catheter).
The first step is to “blindly” wire the SVG towards the native coronary artery (Figure 3B + C) by using a polymer jacket wire and MC. To confirm the wire being in the distal true lumen, visualization of the distal target via collaterals from the other branches is needed. This is confirmed by contrast injection in the donor artery (double access and in selected cases triple access is needed). Here, the SVG is wired using a Pilot 200 (Abbott, US) and Corsair MC (Asahi, Japan).
After this, the native coronary artery is wired retrogradely from the SVG. Sometimes the SVG connects with a sharp angle and the use of Supercross 120° (Teleflex, US) or double lumen MC is needed (Figure 4A). A double lumen catheter is advised if the SVG anastomosis is proximal from the distal cap. In this case, the native RCA was retrogradely wired through the SVG using a Gaia 3 (Asahi, Japan) and Corsair MC (Asahi, Japan).
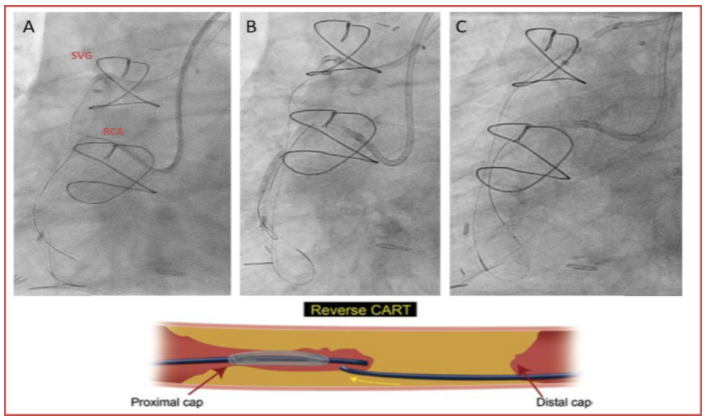
If this is successful, the next step is retrograde wire escalation (RWE), reverse controlled antegrade and retrograde subintimal tracking (reverse CART) or CART. In this case, reverse CART was used (Figure 4B). First, balloon insufflation of the RCA was performed over the antegrade wire in the native RCA, followed by wiring of the created space with the retrograde wire. This wire enters the AR II guiding. The retrograde MC is also advanced into the AR II guiding, after which the retrograde wire is exchanged for a RG3 (Asahi, Japan) or R350 (Teleflex, US) wire (externalization) (Figure 4C).
Lesion preparation with antegrade ballooning is performed over the externalized system (Figure 5A + B).
The final step is to visualize and wire the distal vessel, either through collaterals or through contrast injection with a microcatheter/double lumen side port (Figure 6A). Once an antegrade system is in place and has reached the distal vessel, the retrograde gear has to be removed to avoid jailing the retrograde wire with a stent. A Corsair MC (Asahi, Japan) and Sion Black (Asahi, Japan) were used to wire the distal portion of the vessel (the anastomosis of the occluded SVG was close to the distal cap). Pre-dilatation was again performed, followed by stenting with drug-eluting stents (2.5 x 48 mm Xience Xpedition, Abbott, US in the distal portion of the RCA, 3.0 x 48 mm Xience Xpedition in the mid and proximal portion and a 3.5 x 15 mm Xience Xpedition in the ostium). The end result showed restoration of the antegrade flow in the RCA (TIMI III flow) (Figure 6B).

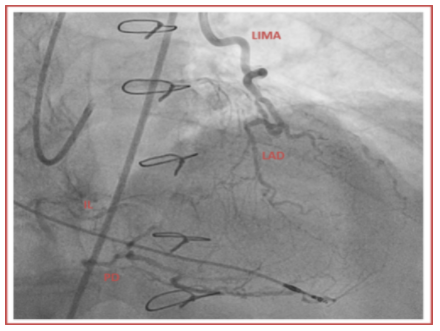
The second case is a 78-year old male who presented with unstable angina (UA). He was known with a double chamber pacemaker (because of 3th degree atrio-ventricular block), transient ischemic attack and CABG (in 1999) with LIMA-LAD and SVG-RCA. The SVG had already been stented 5 months before this episode of UA (Orsiro, Biotronik, US 3.0 x 13 mm in the mid segment + Orsiro 3.5 x 15 mm in the proximal segment). Coronary angiography showed patency of the LIMA-LAD CTO of the native RCA and occlusion of the SVG (occlusion of the stent in the proximal segment). There were collaterals originating from the septal branches to the posterior descending branch (PD) and inferolateral branch (IL) and also collaterals originating from the Cx to the IL branch (Figure 7).
TTE showed preserved left ventricle function without regional contractility abnormalities. Because of the unstable angina and preserved contractility of the inferior wall on TTE, CTO desobstruction was planned.
Triple arterial access was implemented. Contrast injection of the LIMA was performed by 6 Fr IMA guiding catheter through the left radial artery. Contrast injection of the left main was performed by 6 Fr EBU 3.75 through the left femoral artery and the occluded SVG was injected by 6 Fr AL 0.75 guiding catheter through the right femoral artery. During the procedure, we switched the EBU 3.75 to a 7 Fr AR II guiding catheter for injection of the native RCA.
Following the same steps in the flowchart, the first step is to “blindly” wire the SVG towards the native coronary artery with visualization of the collaterals (Figure 8A). The next step is to wire the native coronary artery retrogradely through the SVG, here by using Caravel (Asahi, Japan) MC and Gaia 3 (Asahi, Japan) wire (Figure 8B).

The next step was reverse CART (Figure 9A) and externalization (Figure 9B).

Lesions preparation (Figure 10A) and stenting of the mid and proximal segment (respectively 3.0 x 46 mm Cre8 Evo, Alvimedica, Italy + 3.0 x 26 mm Cre8 Evo) was performed with restoration of the antegrade blood flow in the RCA (TIMI III flow) (Figure 10B).

The third case is a 72-year old male who presented with stable angina. He had a normal ECG without elevated cardiac markers. He was known with CABG (SVG-RCA and LIMA-LAD). TTE showed mildly depressed left ventricle function due to hypokinesia from the inferior wall. Coronary angiography showed a CTO of the RCA with a severely diseased SVG and poor retrograde filling from septal branches (Figure 11).

Double arterial access was implemented. Contrast injection of the SVG was performed by 6 Fr AL I guiding catheter through the right radial artery. Contrast injection of the RCA was performed by 7 Fr EBU 3.5 guiding catheter through the right femoral artery. Also following the same steps in the flowchart, the first step is to wire the SVG towards the native coronary artery. To connect the proximal cap with the distal vessel, the technique of facilitated ADR was used. A knuckle wire was used to dissect from the proximal CTO cap of the RCA beyond the graft anastomosis (Figure 12).
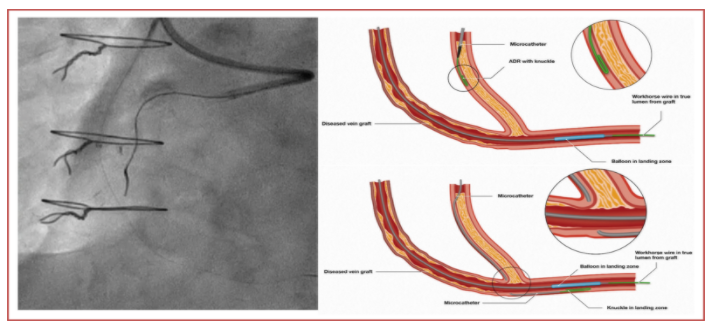
Re-entry from the subintimal space towards the true lumen was performed using the Stingray LP (Boston Scientific, US) at the distal RCA landing zone (beyond the graft anastomosis, but before the crux) (Figure 13).

The re-entry was facilitated by a 3.0 mm compliant balloon via the SVG in the landing zone of the distal true lumen. This balloon is inflated to maximize the target for re-entry by using the Stingray wire (Boston Scientific, US) (Figure 14).
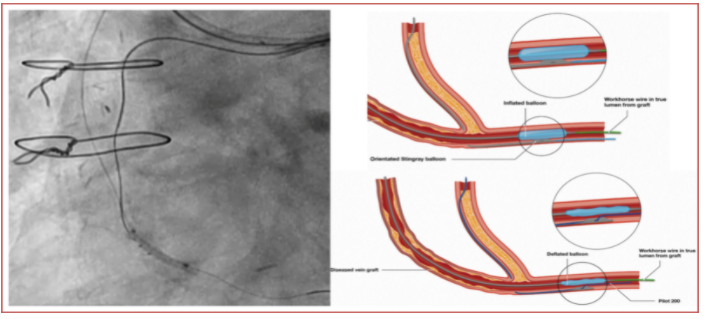
Next, the 3.0 mm balloon is deflated and the Stingray wire can puncture and be advanced through the tissue plane towards the true lumen. After penetration in the true lumen, this wire was exchanged for a Pilot 200 wire (Abbott, US) to wire the distal portion of the RCA (stick and swap technique). Finally, lesion preparation and stenting of the RCA was performed (3.0 x 48 mm + 3.5 x 30 mm, Synergy, Boston Scientific, US) (Figure 15).

Total coronary arterial bypass grafting (CABG) provides better outcome then internal mammary artery (IMA) in combination with saphenous vein grafts (SVGs) [7]. Nevertheless, CABG with SVGs is still widely applied. SVGs will develop over time more atherosclerosis and will be occluded in 50% of the cases in 10 years’ time post CABG [8]. Native coronary arteries also show accelerated atherosclerosis in post CABG patients [9] and therefore new CTOs could originate.
The three conventional techniques of CTO PCI remains the basis, but a retrograde approach through the SVG is suitable. Literature on retrograde CTO recanalization through a SVG is limited [10,11]. More recently, a larger United States (U.S.) registry was published [12].
Dautov et al [10] studied the outcome of CTO PCI through a SVG in 175 patients. Retrograde approach using a SVG was performed in 19% of the patients and through different collaterals in 36%. Antegrade approach was performed in 45% of the patients. The use of either patent of occluded SVGs was associated with a higher success compared with other collateral channels (97% vs 86%; p = 0.02). The final technical success was similar among the 3 different groups: 94%, 84% and 94% respectively for retrograde approach through SVGs, retrograde approach through other collateral channels and antegrade approach.
[11] Nguyen-Trong et al. retrospectively reviewed retrograde CTO PCI through SVG in 21 patients. Procedural success rate was 86% in patients in whom retrograde SVG crossing was successful.
Recently Xenogiannis et al presented their data of PROGRESS-CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention). In this multicenter U.S. registry, 1615 patients were included with comparison of CTO PCI through a SVG (189 patients) versus other collaterals (1426 patients) [12]. The registry showed that the use of SVGs for retrograde crossing was associated with higher rates of procedural success (81% vs. 74%; p = 0.04) and no difference in in-hospital major adverse cardiac events (6.4% vs. 4.4%; p = 0.22) in comparison with retrograde CTO PCI through other collaterals. Moreover, they also report that SVGs are used as collateral conduits in 11.7% of the retrograde PCIs, which is less in Europe and Japan (3.9 % to 8.2%).
Post CABG patients represent an important portion of the CTO procedures. In Japan, these number is relatively low (9.7%) [13]. In Europa it is intermediate (17%) [14] and in the United States high (36.5 %) [15].
J-CTO score in post CABG patients is higher, making the procedure more complex. But, it’s worth of investment for treating the native coronary arteries because of the poor rate of patency success of SVG on the long term [8]. PCI of SVGs is associated with poor long-term results and higher event rates [16].
The ongoing multicenter and randomized PROCTOR (Percutaneous Coronary Intervention of the native coronary artery versus venous bypass graft in patients with Coronary Artery Bypass graft) study will provide new insights in recanalization of the native coronary artery versus recanalization of the SVG in post CABG patients.
Conclusion
Despite all the different techniques which can be used for CTO desobstruction in post CABG patients, the complexity remains. Retrograde crossing of a SVG for native CTO PCI is associated with high rates of success, but is challenging. Therefore we propose a flowchart with algorithm for practical guidance.
Declaration of conflict of interest:
No potential conflict of interest was reported by the authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
