
Review Article | DOI: https://doi.org/10.31579/2690-1919/514
Department of Ophthalmology University of Medicine and pharmacy Carol Davila, Bucharest, Romania
*Corresponding Author: Marieta Dumitrache, Department of Ophthalmology University of Medicine and pharmacy Carol Davila, Bucharest, Romania.
Citation: Marieta Dumitrache, Marian Burcea, Miruna Cioboata, Mihai L. Cioboata, (2025), Age-Related Macular Degeneration – Clinical Therapeutic Etiopathogenic Considerations., J Clinical Research and Reports, 19(4); DOI:10.31579/2690-1919/514
Copyright: © 2025, Marieta Dumitrache. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 March 2025 | Accepted: 20 March 2025 | Published: 08 April 2025
Keywords: age-related macular degeneration (AMD); atrophic exudative; choroidal neovascularization; classic; occult (NVC); drusen; retinal pigment epithelium (RPE); choroidal neovascular membrane (CNM); Bevacizumab; ranibizumab; triamcinolone acetonide;
Age-related macular degeneration – AMD – is a primary irreversible condition, with macular localization, which is accompanied by profound alteration of central macular vision in people over 65 years of age. Senescent changes in the macula affect the retinal pigment epithelium, Bruch's membrane, choriocapillaries and are associated with the presence of retinal pigment epithelium (RPE) detachment, RPE rupture, choroidal neovascularization (CVN). AMD has 2 forms: atrophic (more common, 85%) and exudative. The atrophic form is accompanied by a slow decrease (approximately 5 years) of central vision, with preservation of peripheral vision, the patient having difficulty reading, spatial orientation. The specific lesion of this form of AMD is Drusen. Exudative AMD is accompanied by choroidal neovascularization (classical, occult), after detachment and RPE rupture. The etiopathogenic treatment of AMD is complex and prolonged, attacking multiple aspects: periodic control of risk factors, treatment of oxidative stress, control of lipid metabolism dysfunction, antiangiogenic treatment, corticosteroids. Regulation of the extracellular matrix by laser photocoagulation treatment can be effective for juxta and extrafoveal MNVC. Photodynamic therapy with verteporfin, gene therapy, surgical treatment, artificial vision and, if necessary, combined therapies have also been used to improve visual prognosis. Atrophic or exudative AMD are disabling, progressive conditions with irreversible loss of central vision.
Age-related macular degeneration – AMD is a common cause of irreversible vision loss in patients over 65. The risk of developing AMD increases with age (after 75 years the risk of AMD is 1/3).
AMD is a multifactorial condition that develops in adults over 60 years of age, which includes a set of degenerative, non-inflammatory, progressive, acquired lesions of the macular region occurring in a normal anterior eye.
AMD generates a central scotoma (a central black spot) in the area of the fixation point in the center of the macula, without alteration of peripheral vision.
AMD is responsible for blindness in approximately 11-18% of patients over 65 years of age with eye disease, in which age adjusts the prevalence of the disease. In patients with AMD, the quality of life in daily activity decreases due to quantitative/qualitative changes in central visual perception, with progressive difficulties in reading, driving, and spatial orientation.
AMD is the most common cause of irreversible vision loss in people over 65 years of age in industrialized countries, with the number of AMD patients increasing over the past 15 years.[1,2]
Etiology of AMD
Etiology of macular degeneration Although the cause of age-related macular degeneration is still unknown, genetic factors play an important role alongside other risk factors. A combination of risk factors interact to alter the Bruch's membrane/choroid complex, the retinal pigment epithelium, and the photoreceptor cells of the retina in the macular region.
AMD is thought to be caused by an aging process in the retinal pigment epithelium (RPE), which has limited possibilities for regeneration, with the accumulation of lipid material, through the degradation of the external segmental discs of the photoreceptors. These accumulations increase with age and lead to tissue dysfunction with changes in choroid perfusion. Secondary to hypoxia, VEGF (vascular endothelial growth factor) expression occurs, which contributes to the development of the neovascular form of AMD – the exudative form of AMD.
In the process of AMD formation, an important factor is physiological aging, which causes a series of changes in the macula, many of which are clinically undetectable, affecting the retinal layers, the pigment epithelium, Bruch's membrane, and the choriocapillaries.
All these changes do not represent macular degeneration itself, but just a normal aging process. Macular degeneration involves the appearance of abnormalities with or without neovascularization: detachment, rupture, EPR, choroidal neovascular membrane (NVC).
Risk factors
– the atrophic form is more common in light-colored eyes, with increased incidence in Asians
Pathogenic changes in AMD
- oxidative stress plays an important role in AMD, where an imbalance occurs between the production and elimination of oxygen, the retina being a major consumer of oxygen;
- lipid homeostasis – increased high-density lipoprotein cholesterol is associated with increased risk of AMD, low-density lipoprotein reduces risk of AMD
- inflammation and immunity
- neovascularization - is generated by VEGF, which is a determining risk factor for AMD, VEGF playing an important role in the occurrence of neovascularization
- other mechanisms
AMD Clinic
Clinically, AMD is:
Atrophic Am
Atrophic AMD is a condition with vision loss, with slow progression, approximately 5 years, with preservation of peripheral vision, because the degenerative process affects the central foveolar region of the macula, an area with high spatial resolution7,8.
Clinically, druse are small, round, yellow lesions located on the basal surface of the RPE and give a thickened appearance to Bruch's membrane.
They can be in the form of basal laminar deposits – they have a granular appearance, rich in lipids and collagen fibers between the basement membrane of the pigment epithelium and the plasma membrane or in the form of linear deposits – dense granules with phospholipid vesicles in the internal area of Bruch's membrane. These deposits can cause detachments of the pigment epithelium.9
According to their size, druse can be: - small under 63 microns in diameter, intermediate between 63-124 microns, large over 125 microns.
Drusen can coalesce, causing drusenoid detachments of pigment epithelium over 350 microns in diameter.
Drusen are: miliary, serous (represents the major sign of age-related macular degeneration), reticular, (reticular pseudodrusen), pigmentary migrations.
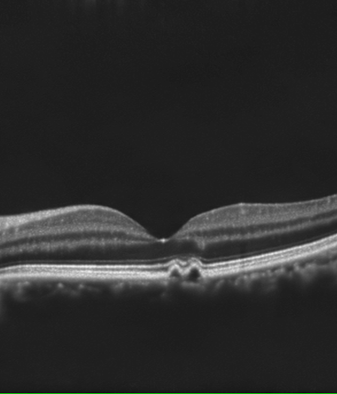
Figure 1: (left) Macular Druses-CT view, they occur as waves and elevations of the pigmentary epithelium with hypo reflective material underneath.

Figure 2: (Right) Millenary druses
Their evolution over time may be towards multiplication and their confluence transforming into serogranular druse. An evolution towards atrophy or choroidal neovascularization is rare.

Figure 3: Serosal macular druses
Atrophic AMD is the most common form of AMD, approximately 85% of cases, characterized by the disappearance of photoreceptors, pigment epithelium, and choriocapillaries.
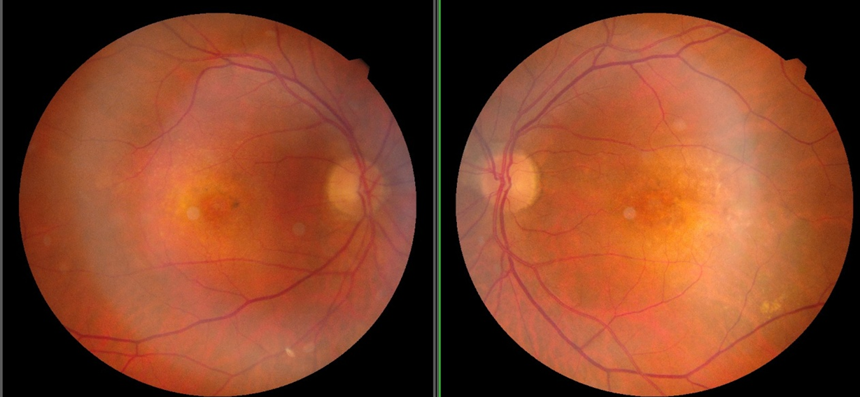
Figure 4: Pigmentary migration in the macula
Atrophy may be the consequence of drusen regression and pigmentary changes.

Figure 5: Geographic atrophy - atrophy of retinal pigmentary epithelium with view of coordain circulation
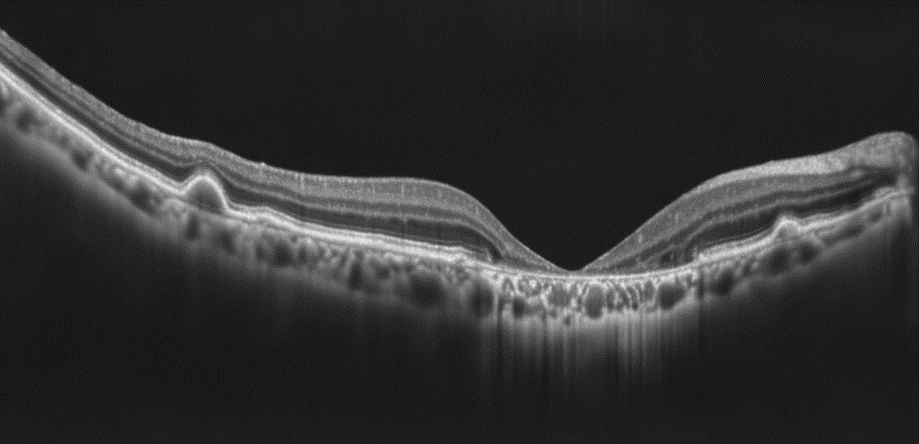
Figure 6: Geographic atrophy-CT view, lack of photo-receptors and atrophy of retinal layers in the macula
Differential diagnosis is made with atrophic changes in the RPE induced by central serous chorioretinopathy, hereditary macular dystrophies, late-onset vitelliform dystrophy of the macula, and toxic chloroquine maculopathy.
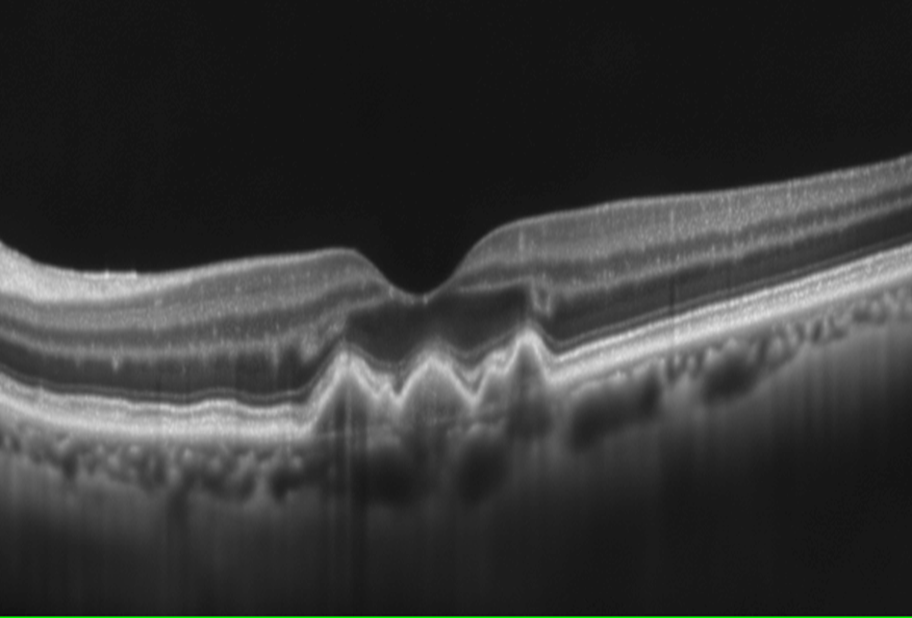
Figure 7: Retinal drusens behind the foveolar
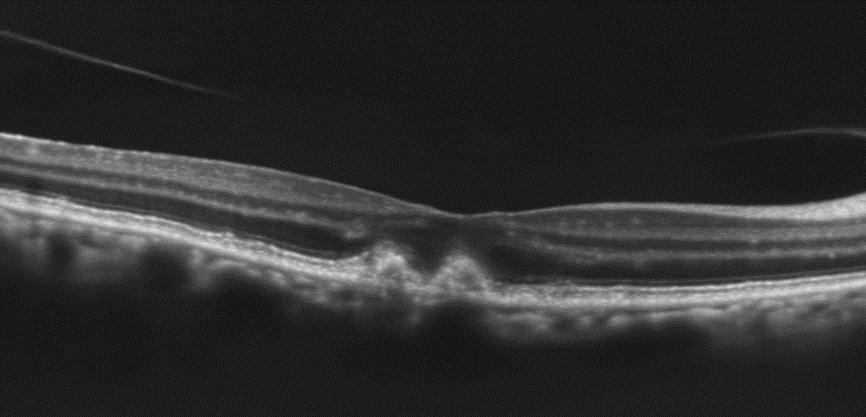
Figure 8: Pseudo-drusens, located above the pigmentar epitelium and immediately underneath the photo-receptors that are hyper-reflective
Clinically, in atrophic AMD it is highlighted:
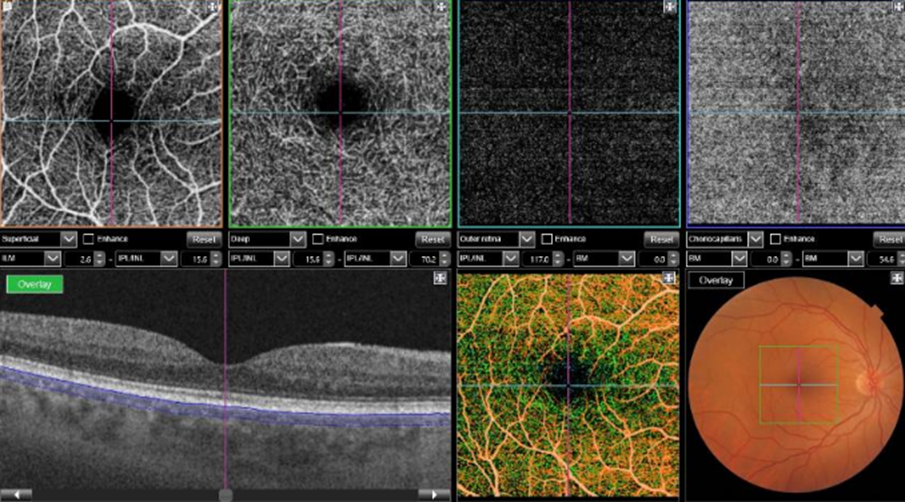
Figure 9: Ocular angiographic computer tomogram images-upper images (from left to right) superficial plexiform strata, deep plexiform strata, external avascular retina, and choriocapillaries, lower images various aspects of ocular CT and ocular angiographic CT
Investigations
Optical coherence tomography (OCT)It is a noninvasive method that makes sections of the retina and precisely locates lesions.
Optical coherence tomography with OCTA angiography
- uses a new technology that also detects the movements of red blood cells and thus blood vessels can be visualized in vivo.
Fundus autofluorescence FAF - is due to the accumulation of fluorophores in the retina that accumulate in the lysosomes of EPR cells as lipofuscin. Retinal areas lacking EPR cells cause a lack of autofluorescence and appear as dark areas.
Patient monitoring with macular diseases can be done with the AMSLER test
Amd Exudative – Wet – Neovascular Form
Exudative AMD:
Exudative AMD is accompanied by detachment and rupture of the RPE with the development of choroidal neovascularization – NVC [3,8]
The evolution of DEPR is towards: spontaneous resolution in young people, geographic atrophy with atrophic AMD or sensory retinal detachment with passage of subretinal fluid and development of classic and occult neovascularization, in the presence of spontaneous RPE rupture with neovascularization.
Exudative AMD is characterized by the presence of choroidal neovascular membrane (CNMV)
Differential diagnosis of neovascular AMD
Paraclinical evaluations in wet AMD10
AFG-highlights EPR dehiscence with long-term fluorescein retention, highlighting the edges of the lesion, with intense hyperfluorescence with rapid diffusion of fluorescein through the permeable Bruch membrane and pooling under the EPR
Therapeutic objectives in AMD [5,8,14,15,16]
AMD treatment is an adjuvant treatment to limit the major decrease in visual function, as there is no effective medical treatment for the recovery of visual function. AMD treatment is a treatment that blocks inflammation, blocks free radicals, inhibits the release of vasoforming factors, stimulants of choroidal neovascularization.
AMD treatment includes2,6,14,15:
AMD occurs through the correlation between primary degenerative lesions, related to the patient's age, associated with disturbances in cellular homeostasis. Cellular senescence is the initiating factor of AMD, and the progression of the disease is associated with multiple other, correlated mechanisms: oxidative stress, inflammatory factors, changes in immunity.
AMD treatment is a complex, prolonged treatment that must control the multiple disorders of the factors that generate serious eye disease.15,17
Etiopathogenic treatment in AMD
Anti-VEGF medication It is a complex, sustained treatment and requires permanent therapeutic administration after a rigorous periodic ophthalmological check-up.
AVASTIN – Bevacizumab (2005)
LUCENTIS – Ranibizumab
EYLEA – Aflibercept
MACUGEN – Pegaptamide (2004 (first used)
BROLUCIZUMAB – Beovu
PEGAPTANIB – intravitreal 0.3mg every 6 weeks
SUTINIB
CONBERCEPT, Abicivar, OPT-302, RG 7716
Anti-inflammatory treatment
CorticosteroidsIt acts by stabilizing the blood-ocular barrier, blocking inflammation, blocking angiogenesis by inhibiting macrophages that release angiogenic factors.
Intravitreal implants:
Anecortav is a corticosteroid derivative that inhibits angiogenesis by interfering with proteinases that promote vascular proliferation and endothelial migration.
Inhibitive C3, C5 - ZIMURA
Reduction of apoptosis, angiogenesis – (VEGF A) Risutegamib
Reducing blood viscosity – rheopheresis
Extracellular matrix regulation - Laser photocoagulation treatment
Laser photocoagulation aims to destroy neovessels to limit their proliferation and extension, thus limiting the progression of AMD.
Laser FC is indicated in juxta and extrafoveal NVC
Radiotherapy
Photodynamic therapy with verteporfin – PDT
It consists of the intravenous administration of a photosensitizing drug that localizes in the choroidal neovessels followed by local activation of the drug with a nonthermal laser.
Gene therapy
It consists of implementing a functional gene to correct a genetic error or to introduce a new function into a pre-existing cell for the treatment of disease.
Surgical treatment
The macular surgery approach remains a promising therapy in well-selected cases despite possible postoperative complications, achieving clearer vision.
Combined treatments
Artificial vision
Artificial vision with cortical, retinal prostheses.
There is no effective medical treatment at this time for AMD. Treatment in AMD is an adjunctive treatment to limit risk factors, block inflammation, block free radicals, inhibit the release of vasoforming factors, stimulators of neovascularization.
Age-related macular degeneration – AMD is a common cause of irreversible, progressive vision loss over the age of 65. AMD causes profound impairment of visual functions through degenerative lesions in the macula. AMD is caused by senescent degenerative lesions of the macular retina (decrease in photoreceptors, thickening of the Bruch membrane, thinning of the choroid) associated with subretinal fluid accumulation, detachment damage and RPE rupture with the appearance of classic and occult choroidal neovascularization (NVC), the atrophic form of AMD is more common (85%) and is accompanied by slow, progressive loss of central vision. Exudative AMD is accompanied by subretinal fluid accumulation, the presence of neovascular choroidal membrane, detachment with RPE rupture, classic or occult choroidal neovascularization. Exudative AMD is associated with progressive irreversible loss of central vision. Current treatment of AMD is etiopathogenic and attempts to limit the anatomical/functional degradation of the eye in order to limit the rapid degradation of vision loss. Complex and prolonged treatment, single or combined, includes: risk factor control, oxidative stress treatment, antiangiogenic treatment, anti-inflammatory treatment, C3, C5 inhibitor, laser photocoagulation treatment, photodynamic therapy, surgical treatment, gene therapy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
