
Research Article | DOI: https://doi.org/10.31579/2692-9562/049
1 DR. RAHUL KUMAR SHAH, M.S ENT, M.CH. Head and Neck surgery, Gujarat, India.
2 M.S. E.N.T., Department of E.N.T. & Head-Neck Surgery, Baroda Medical College, Vadodara, Gujarat.
3 Dr. Rahul Gupta - M.S. E.N.T., Associate Professor, Department of E.N.T. & Head- Neck Surgery, Baroda Medical College, Vadodara, Gujarat.
4 M.S. E.N.T., Professor and Head, Department of E.N.T. & Head- Neck Surgery, Baroda Medical College, Vadodara, Gujarat.
*Corresponding Author: Rahul kumar Vijaykumar Shah, Professor Samileh Noorbakhsh, pediatric infectious diseases Department &Research center, Iran University of Medical Sciences. Tehran, Iran.
Citation: Rahul k.v Shah, Atisha Modi , R Gupta, R. G. Aiyer(2022) Aerodigestive Foreign Bodies: Our Experience Journal of Clinical Otorhinolaryngology 4(3); DOI: 10.31579/2692-9562/049
Copyright: © 2022, Rahul kumar Vijaykumar Shah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 15 April 2022 | Accepted: 20 May 2022 | Published: 25 June 2022
Keywords: aerodigestive tract foreign bodies; coins; endoscopy
Foreign body ingestion and aspiration is a common cause of morbidity and mortality, usually occurs in children. A detailed history and physical examination with a high index of suspicion, despite negative imaging are required. Often, a diagnostic endoscopy may be required to definitively investigate the upper aerodigestive tract to rule out foreign body in equivocal findings. Non caustic oesophageal foreign bodies can be observed for a short period of time while Airway foreign bodies require immediate removal in the operating room. A team-based approach with coordination between the trained anaesthetist, surgeon, and operating room staff is required during this foreign body management.
FB- Foreign body, ENT- Ear Nose Throat, PA- posterior-anterior
Killian did first successful bronchial foreign body removal by passing a 9 mm endoscope. After that, in 1905, Chevalier Jackson did bronchial foreign bodies removal and developed instruments for laryngoscopy and bronchoscopy [1], truly known as the father of endoscopic aerodigestive foreign body removal. Aerodigestive foreign body ingestions and aspirations occur more commonly in children under the age of 3 years [2-4], due to their increased mobility, tendency to play and eat at the same time, lack of cognitive recognition of edible versus inedible objects, high propensity for placing objects in the mouth addition, incomplete molars making chewing difficult and an immature or underdeveloped ability to swallow [5].
Most foreign bodies are expelled immediately by protective cough and spitting reflexes. Inhaled foreign bodies more commonly include organic materials such as nuts, seeds, vegetable matter, or dried fruits [2,3,6,7] When aspirated, they frequently become lodged in the bronchial tree, with the right main bronchus being more common because of its wider lumen and more vertical path8. Oesophageal foreign bodies lodge commonly in cricopharynx, but most of these pass on to the stomach and may not necessarily require removal [9,10]. Coins and pins are the most commonly ingested items [11]; other common items include batteries, toy parts, bones (fish, chicken), and jewellery [12,13].
A total of 102 patients with definitive history or suspicion of aerodigestive foreign body were admitted or referred to ENT department of Sir Sayajirao General Hospital, Vadodara, Gujarat over a period of two year were reviewed retrospectively [from January 2018 to December 2019]. All these cases are studied in detail for age, sex, type of foreign body, site of lodgement, radiographic evaluation details and treatment given.
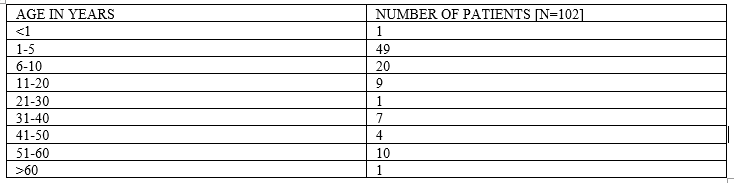
Total number of reviewed patients are 102. The patients’ age distribution is shown in table 1. Children between age of 1 year to 10 years were the most involved (67.64%). The patient’s Sex distribution is shown in table 2. The patient’s male to female ratio was 1.42. In the majority of children, the FB ingestion or aspiration was witnessed or strongly suspected by a bystander after the sudden onset of symptoms.
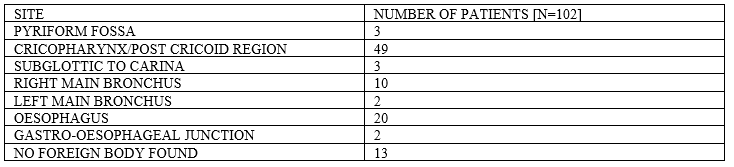
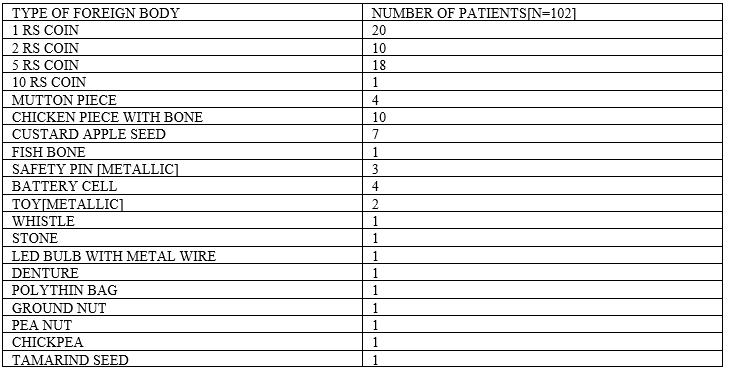
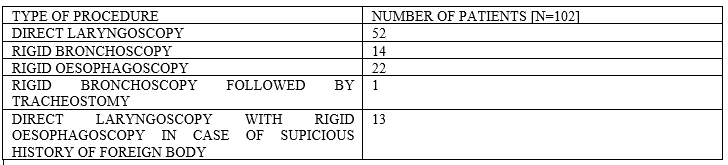
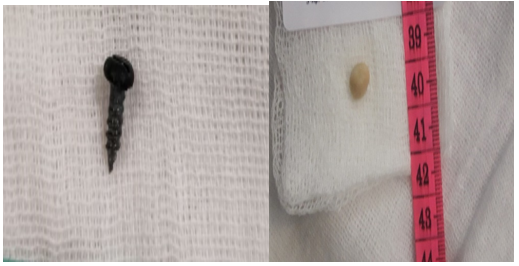
Site of FB lodgment, Type of foreign body found and Type of endoscopy performed is shown in table 3 ,4 and 5 respectively. A total of 102 rigid endoscopies were performed under general anesthesia. Rigid Esophagoscopy was performed in 22 cases (21.56%), Rigid bronchoscopy in 14 cases (13.72%), hypopharyngoscopy and direct laryngoscopy in 52 cases (50.98%). Rigid bronchoscopy followed by tracheostomy was done in 1 patient due to non-retrievable FB via endoscope. Direct laryngoscopy with Rigid Esophagoscopy were done in 13 cases. (12.74%)-cases of no FB found. FB were encountered in 89 patients (87.25%). In 13 patients no FB were found (12.74%). The most common involved sites were the cricopharynx/post cricoid region (48%) followed by the esophagus (19.6%) and the tracheobronchial tree (14.70%). Pyriform fossa FB and Gastro-esophageal junction FB were found in 3 and 2 cases respectively. Coins were the most frequently encountered FB (48%), followed by chicken bone (9.8%), custard apple seed (6.86%), mutton piece (3.9%), battery cell (3.92%), safety pin metal (2.94%), denture (0.98%) and beans, whistle, led bulb with wire, stone etc. The complication rate in our patient series was 2.94% [3 case], two patients had esophageal mucosa erosion after esophagoscopy, one patient had to undergone tracheostomy for FB removal and for airway management. All of these patients were fed with nasogastric tube for a minimal period of 10-14 days and intravenous antibiotic therapy including Cefotaxime and Metronidazole with dexamethasone according to weight were given. All these cases had full recovery.

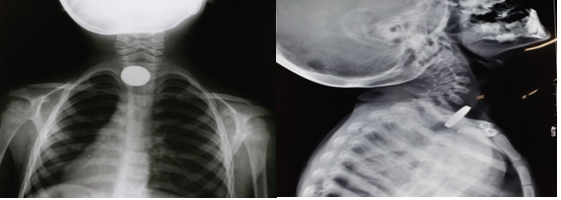


There are three clinical stages of aspiration and ingestion of foreign bodies - The first stage is the impaction of the foreign body causing choking, coughing, or gagging. In second stage symptoms wane as the foreign body settles into a stationary location and the tracheoesophageal reflexes attenuate. This stage lasts for hours to weeks, delaying diagnosis. In third stage complications like obstruction, infection, or perforation [5] occurs. During evaluation of foreign body case, it is advisable to elicit information from the parents like, approximate time of ingestion or inhalation, a history of esophageal dysfunction, severity and duration of swallowing or respiratory dysfunction. In majority of cases, it may be helpful to ask the parents to bring in a similar object from home, particularly for unusual foreign bodies [14]. Foreign body inhalation most commonly causes cough, dyspnea, wheezing, cyanosis, or stridor [3,7] whereas esophageal foreign body ingestion causes drooling, dysphagia, emesis, food refusal, and chest pain. After careful evaluation of history, chest auscultation is must because asymmetry of breath sounds or a prolonged expiratory phase of respiration can give clue to bronchial foreign body, although a normal imaging study does not rule out the presence of a foreign body. Standard frontal and lateral radiographs are the imaging tests of choice for suspected airway foreign bodies [15]. Radiopaque airway foreign bodies are easy to diagnose, whereas organic and other radiolucent airway foreign bodies are more difficult to diagnose. In these cases, other radiographic signs such as unilateral emphysema, hyperinflation, localized atelectasis or infiltrates, and mediastinal or esophageal air trapping may also be indicative of an airway foreign body. In majority of cases, the only evidence of an airway foreign body will be localized air trapping or atelectasis [16]. The classical teaching that sagittal oriented foreign bodies lie in the trachea and coronally positioned foreign bodies are in the esophagus does not hold true in all cases. Esophageal foreign bodies may be found in either the sagittal or coronal configuration. The tracheal foreign bodies more commonly lodge in the sagittal plane because of the longitudinal orientation of the vocal cords and lack of cartilage in the posterior tracheal wall [17]. If the foreign body appears to overlap the tracheal boundaries on a PA view, it is highly unlikely to be in the trachea and a lateral radiograph in this case may confirm that the foreign lies in the esophagus, posterior to the trachea, or demonstrate soft tissue swelling or loss of normal cervical lordosis [18]. Button batteries have a characteristic double contour on lateral view, also known as the “step-off sign,” but may be mistaken for coins on PA views. The characteristic “halo sign” or “double-ring” sign on PA views can help to differentiate a button battery from a coin [14]. Barium swallow is generally not done because it can make subsequent esophageal foreign body removal more difficult.
Low-dose airway CT scans, also known as “virtual bronchoscopy,” are useful when there is a low suspicion for airway foreign body along with a negative chest x-ray and lack of findings on lung auscultation. This Virtual bronchoscopy has high sensitivity so, a negative scan avoids unnecessary bronchoscopy under general anesthesia [19]. For esophageal foreign bodies, standard Posterior-anterior and lateral radiographs are used to identify the presence of and localize multiple foreign bodies [20].
There is a different opinion among surgeons regarding the decision and timing to intervene for an airway foreign body, the choice of anesthesia for bronchoscopy. The three main considerations are (1) method of induction, (2) type of ventilation during bronchoscopy, and (3) maintenance of anesthesia. Rapid sequence techniques is preferred if aspiration of stomach contents is a risk concern [13,23]. Generally, spontaneous ventilation with negative pressure inhalation has been the preferred method because it takes advantage of the natural increase in tracheal and bronchial cross-sectional area during inspiration, and the risk of distal migration of the foreign body with positive pressure ventilation is avoided. However, achieving an adequate depth of anesthesia can be challenging because too deep leads to apnea and consequent hypoxemia and too light risks patient movement and possible bronchial tree injury [18]. Alternatively, controlled jet ventilation ensures a steady level of deep anesthesia and ventilation, which ensures better oxygenation, less coughing or bucking, and less patient movement, but has the risk of displacing the foreign body further down the airway.
The decision to remove an esophageal foreign body depends on factors like type and location of the object, the patient’s age, and time elapsed since the ingestion. An asymptomatic older child with a distal or mid-esophageal object present for less than 24 hours and no history of esophageal disorders may be observed for a period of 8 to 16 hours to see if the object will pass. For young children, foreign bodies present longer than 24 hours, sharp metallic or caustic foreign bodies, or symptomatic patients, urgent endoscopy is warranted; observation for spontaneous passage is not appropriate in these settings. The spontaneous passage rates for esophageal coins in healthy children varies from 9% to 77% [21,22]. For the majority of esophageal foreign bodies, the child should be intubated to minimize the possibility of aspirating the foreign body upon removal and to reduce tracheal compression by the esophagoscope [5].
Postoperatively, if the procedure was uncomplicated, the child can be discharged from the recovery room with regular follow-up to ensure that symptoms have resolved completely. If there is concern regarding foreign body remnant, a repeat endoscopy can be performed [5]. Usually, a postoperative x-ray may be ordered to rule out perforation and mediastinal air.
Most children with aerodigestive foreign body ingestions make a full recovery without permanent sequelae. Complication rates of aerodigestive endoscopy are reported, from 1% to 8% [24]. The risk of complications increases with the duration of time that a foreign body remains in place. The most common complications of rigid bronchoscopy include failure to remove the foreign body, laryngeal edema, pneumothorax, pneumomediastinum, and subcutaneous emphysema. Laryngeal edema may rarely be significant enough to warrant intubation or tracheotomy. Mortality rates in the literature vary from 0.2% to 1.0% [18]. For esophagoscopy, complications include mucosal injury, bleeding and, rarely, perforation, which can cause mediastinitis [10]. In a minority of cases, esophageal endoscopic removal is unsuccessful and requires surgical intervention such as a thoracotomy, esophagotomy, gastrotomy, or jejunotomy [18].
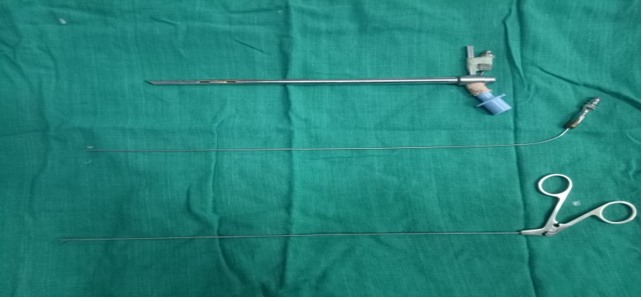
In our retrospective analysis, children below 10 years were most common culprit for foreign body ingestion or inhalation. Standard diagnostic evaluation in form of history, full ENT and chest examination, appropriate x-rays and virtual CT scans were done as and when required. With proper pre-operative preparations endoscopies were performed under general anesthesia. Laryngeal and hypopharyngeal FB were removed under Rigid direct laryngoscope with fiberoptic light carrier. Esophageal FB were removed under rigid esophagoscope with distal illumination. FB in the tracheobronchial tree were removed through the rigid bronchoscope with distal illumination. In our analysis bronchoscope with 4 mm diameter commonly used. All FB were removed with an alligator grasping forceps with double action jaws. Coins were the most common ingested foreign body and custard apple seed were more common inhaled foreign body.
Cricopharynx was most common site of lodgment in ingested foreign body and right main bronchus in inhaled foreign body. Intravenous antibiotic therapy, nebulization and steroids were administrated according to age and weight of patients. Nasogastric feeding tube was put when there where esophageal mucosa erosion or perforation. In immediate postoperative period close monitoring was done, especially after bronchoscopy and chest X-ray was performed after each esophagoscopy or bronchoscopy. Majority of patients were discharged on next morning with follow-up advice.


The ingestion or aspiration of foreign body is a significant cause of morbidity and mortality mainly in the paediatric population. Parental and physician education regarding these dangers are the most important factors in reducing the incidence of this problem. Prompt recognition and a comprehensive history can identify these affected children in a timely fashion. Management is individualized depending on the duration of symptoms, properties of the object or substance ingested and location of the object. An expedient evaluation and workup are important in limiting the number of complications.
There is no conflict of interest among authors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
