
Research Article | DOI: https://doi.org/10.31579/2690-8794/100
1 Department of Pathology, Institute of Medicine, Yerevan Haybusak University, Armenia.
2 Department of Pharmacy, Institute of Medicine, Yerevan Haybusak University, Armenia.
*Corresponding Author: Tigran R. Petrosyan, Department of Pathology, Institute of Medicine, Yerevan Haybusak University, Armenia.
Citation: Tigran R. Petrosyan and Nihad Imad Kanaan (2021) Adverse Event Reporting in Patients with Thyroid Dysfunction Treated with Levothyroxine in Armenia. A Cross Sectional Pilot Study. Clinical Medical Reviews and Reports. 3(8); DOI: 10.31579/2690-8794/100
Copyright: © 2021, Tigran R. Petrosyan, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 09 August 2021 | Accepted: 26 August 2021 | Published: 03 September 2021
Keywords: levothyroxine, thyroid-stimulating hormone, hypothyroidism, oral levothyroxine
Background and Aim. Currently two forms of levothyroxine are presented in pharmaceutical market of Armenia: Euthyrox and L-thyroxine. Local physicians have a choice of two different levothyroxine preparations, each of them with different dosage from 25 to 150mg. Oral levothyroxine (LT4) is the standard therapy for patients with hypothyroidism. The purpose of this report is to describe the adverse outcomes reported by endocrinologists, the frequent prescribers of levothyroxine, practicing in Armenia and to compare the rate of adverse reactions with data from different international research reports.
Materials and methods. A Pharmacovigilance questionnaire was developed based on the literature reports to assess potential adverse events attributable to the use of levothyroxine products. Statistical Analysis Results were collected, interpreted and presented as percentages.
Results. The study was with a cross-sectional design conducted in medical centers of Armenia using convenience sampling. The respondent parents of patients were selected using simple random sampling. Of the total 56 survey responses received, the majority 35 [63%]) reported no adverse events. The adverse effects were due to new or unexpected symptoms in 2 (25%), a TSH change alone in 1 (12%), or both in 6 (75%). Most the symptoms (5/8 [65%]) were consistent with thyrotoxicosis, arrhythmias were documented in three cases, while 35% (3/8) of cases had symptoms typical of hypothyroidism.
Conclusions. Clinicians prescribing Euthyrox and L-thyroxine should be reminded that these products are from different manufacturers and patients/physicians should be made aware of all possible adverse reactions results, which could be different for these two products.
Currently two forms of levothyroxine are presented in pharmaceutical market of Armenia: Euthyrox and L-thyroxine. Local physicians have a choice of two different levothyroxine preparations, each of them with different dosage from 25 to 150mg [1].
Oral levothyroxine (LT4) is the standard therapy for patients with hypothyroidism. Oral LT4 is available internationally in several formulations, including tablets, soft gel capsules and oral solution. Multiple brand-name and generic LT4 tablets are available. In the US, the Food and Drug Administration (FDA) has developed a protocol for establishing bioequivalence of LT4 formulations based on serum thyroxine (T4) levels after a single oral dose administered to healthy volunteers [2]. This protocol has been criticized by professional endocrinology associations for ignoring serum thyroid-stimulating hormone (TSH) levels [3, 4]. There are concerns that the FDA’s protocol could allow products with clinically significant differences in bioavailability to be declared therapeutically equivalent and interchangeable. Often, the substitution is made by the pharmacy without the physician’s knowledge [5]. Even small differences between LT4 formulations can cause significant changes in TSH levels. This may be a particular concern in vulnerable populations, including elderly, pregnant, and pediatric patients [6, 7]. Problems that can be encountered when switching between formulations or when original products are reformulated include altered efficacy and adverse events, some of which can be caused by excipients. Patients should be maintained on the same LT4 preparation if possible. If the LT4 preparation is changed, TSH levels should be evaluated and, if necessary, the dose of LT4 adjusted [8-10].
The more common side effects of levothyroxine can include: increased appetite, weight loss, heat sensitivity, excessive sweating, headache, hyperactivity, nervousness, anxiety, irritability, mood swings, trouble sleeping, tiredness, tremors, muscle weakness, changes in menstrual periods, hair loss (usually temporary), diarrhea, vomiting and stomach cramps. If these effects are mild, they may go away within a few days or a couple of weeks. If they are more severe then patients need medical attention [11-14].
The purpose of this report is to describe the adverse outcomes reported by endocrinologists, the frequent prescribers of levothyroxine, practicing in Armenia and to compare the rate of adverse reactions with data from different international research reports [15, 16].
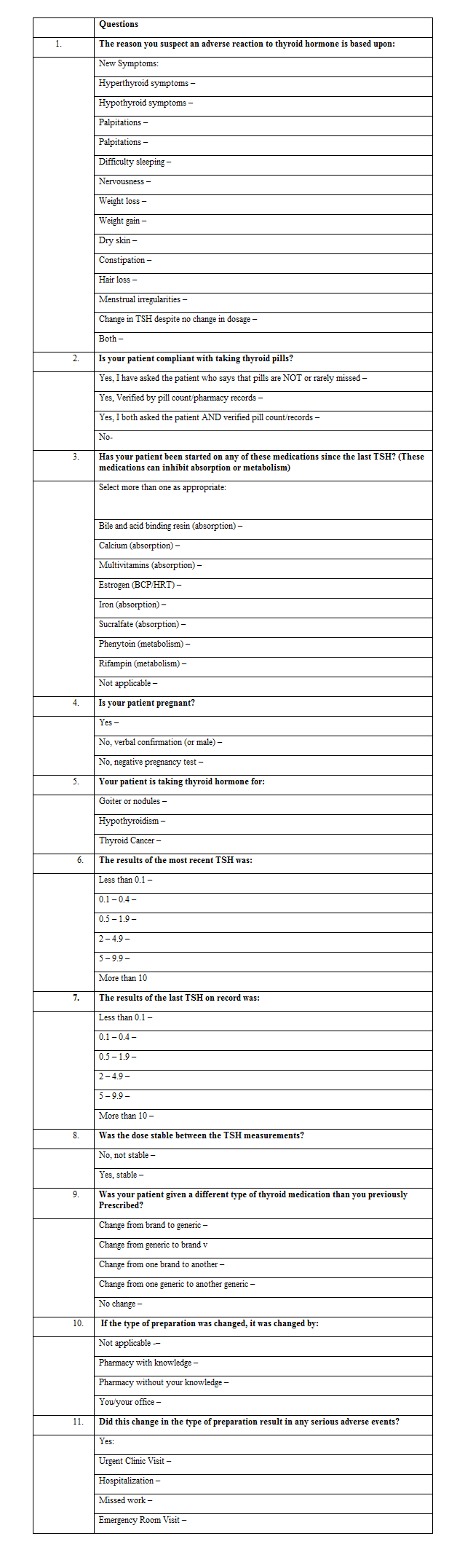
A Pharmacovigilance questionnaire was developed based on the literature reports to assess potential adverse events attributable to the use of levothyroxine products. We used a modified survey tool that was created to gather data similar to that used by FDA and developed by the American Association of Clinical Endocrinologists (AACE) and The Endocrine Society (TES) to survey the experience of physicians caring for patients with thyroid disease on thyroid extract or LT4 therapy [17].
Participants of the study were patients with thyroid dysfunction who sought therapy services in specialized departments. The study was with a cross-sectional design conducted in medical centers of Armenia using convenience sampling and included randomly selected endocrinology services in the district towns and in the capital city. We used convenience sampling model and not a randomized approach as not all regional hospitals in the country include endocrinology departments. The respondent parents of patients were selected using simple random sampling. A minimum sample size of 56 patients was derived using the formula N = [z2 p (1-p)] ÷ ME2 [18], where z = confidence interval at 95% thus 1.96; p = assumed prevalence of adverse reactions, 50%; and ME = margin of error, 0.05. Criteria for the inclusion in the study sample were the impaired level of TSH and/or thyroid hormones and confirmed diagnosis of thyroid disorder.
The questionnaire was distributed among endocrinologists working in different centers and the result of reports received from physicians were compared to international data reported from variety of authors. Following the development of the questionnaire we contacted the physicians in Armenian Canadian medical Center, Erebuni clinic, and Kotayk regional hospitals. A total of 14 responses were received between March 2021 and May 2021. The current report describes the adverse events reported by physicians caring for 56 individuals using thyroid formula Euthyrox or L-thyroxine.
Statistical Analysis Results were collected, interpreted and presented as mean and percentages. For statistical and graphical evaluations Microsoft Excel 2013 (Roselle, IL, USA) was used.
"N-1" Chi-squared test was used to compare the proportions registered in the local study and in previous reports.
The modified pharmacovigilance survey questionnaire [17] included 11 questions with subpoints.
Of the total 56 survey responses received, the majority 35 [63%]) reported no adverse events. A total of 21 completed adverse event (AE) reports (37% of total responses) were further reviewed. Of these, 12 (59%) reported adverse experiences with levothyroxine. Of the 12 patients reported, only 10 patients were on it as sole treatment for their thyroid disorder and among these 10 reports, 2 of the adverse events indicated that there had been recent dose adjustments which would account for the symptoms and altered thyroid function assessments.
All the reports were focused on adverse events observed by physicians caring for patients on thyroid hormone prescription. After elimination of reports related to noncompliance with Euthyrox (11), erroneous reporting (4), interfering medication use (4), pregnancy (3), recent changes in levothyroxine dosing and the reporting of symptoms only associated with an unchanged TSH values (6), after these adjustments, 8 reports of adverse events remained.
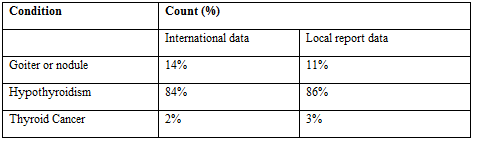
Compliance with the levothyroxine treatment was confirmed by the reporting physician based on verbal report of the patient in 47/56 (84%) of the cases. Levothyroxine therapy was being administered for the indications of hypothyroidism in 48 of the 56 patients (86%), thyroid cancer in 2/56(3%), and goiter or nodule suppression in the remaining 6/56 (11%) report. Therefore, biochemical euthyroidism would have been expected in 86% or more of the reports and TSH suppression of some degree would have been expected in the remaining cases.
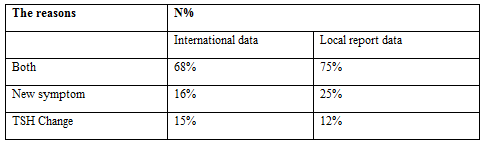
Of the 56 completed pharmacovigilance reports on compliant individuals on stable doses of levothyroxine, the adverse effects were due to new or unexpected symptoms in 2 (25%), a TSH change alone in 1 (12%), or both in 6 (75%). Symptoms include both typical thyrotoxic symptoms (e.g., weight loss, nervousness, difficulty sleeping, palpitations, and tiredness) and typical hypothyroid symptoms (weight gain, constipation, menstrual irregularity, dry skin, fatigue and hair loss). Most the symptoms (5/8 [65%]) were consistent with thyrotoxicosis, arrhythmias were documented in three cases, while 35% (3/8) of cases had symptoms typical of hypothyroidism.
The TSH distribution from suppressed to elevated levels found during the survey is described in this figure. Prior to the reported adverse event, TSH values were within the normal range (0.5 to 5) in 4 of 8 (50%) of the reports, TSH was suppressed below normal in 3 of 8 (38%), and exceeded the upper limit of the reference range in 1/8 (12%) TSH values reported. At the time of the reported adverse event, 6 of the 8 (75%) TSH values were below normal with 1 of 8(12%) of TSH values were suppressed but detectable and the majority, 1 of 8(12%) being undetectable.
The overall trend in TSH change at the time of the reported event was a substantial increase of the number of subjects demonstrating evidence of excess thyroid hormone (5/8) exposure a rate which nearly doubled.
Free text comments were made by 4 physicians during the survey. The most common reason cited for discontinuing the drug was an inability to dose the drug based on symptoms and TSH values (2 out of 4 comments). 1 of these 4 physicians stated that the drug was initially prescribed by a different provider. Arrhythmias were documented in two patients. The tables presented show the rate of adverse events collected in Armenia and compare them with data of international reports:



This survey of Levothyroxyne documents 8 validated reports of adverse events accompanied by objective changes in the thyroid function that were associated with the use of stable doses of the compound in compliant subjects.
The purpose of this pilot study was not only the assessment of adverse reactions registered in patients with thyroid disorder treated with Euthyrox and L-thyroxine, and estimation of the prevalence of these adverse effects. The study aimed to compare the rates with data available from the previous research reports. The tables presented in results reveal somewhat higher prevalence of adverse reactions in a previously reported study (32% vs 24%) [17]. The sample sizes compared were different (565 vs 56), but statistical comparison of results revealed no significant difference in proportions (Chi-squared = 1.515; P = 0.2184).
The sample size of this study was relatively small, also limiting the generalizability of our findings. There may also have been selection bias as the most dramatic cases seen would have been preferentially put forward as adverse events. However, since the reporting was voluntary and provided by practitioners, the frequency of adverse events was likely under-reported.
Although the manufacturers of levothyroxine have made great strides to standardize the content of their products, the preparations remain not fully controlled by the regulatory bodies. The responses documented in this survey raise clinical concerns. It is important to provide a broader understanding of issues that may arise from use of the Euthyrox and L-thyroxine among physicians, pharmacists, and patients to achieve optimal treatment for hypothyroidism. Clinicians prescribing Euthyrox or L-thyroxine should be reminded that these products are from different manufacturers and patients/physicians should be made aware of all possible adverse reactions results, which could be different for these two products. These data show that the frequency of dose adjustments in levothyroxine users appears to be much more common when compared to rates observed in different international reports. Most symptoms encountered in those using levothyroxine were consistent with exposure to excessive thyroid hormone use.
We have no evidence that the potency of levothyroxine preparations varies with currently available products: Euthyrox and L-thyroxine, nor that any such variability played any role in the events reported here. Further studies are required to compare the adverse events of Euthyrox and L-thyroxine with that of other levothyroxine preparations and assess the rate of these events to justify the continued use of selected preparations.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
