
Review Article | DOI: https://doi.org/10.31579/2690-4861/610
1 Medical Clinic II, University Wuerzburg, Occupational Department, Germany.
2 Institute of Pathology, University Wuerzburg.
3 Institute of Anatomy, University Wuerzburg.
4 Institute of Experimental Biomedicine, University Wuerzburg.
*Corresponding Author: F.W. Schardt, Medical Clinic II, University Wuerzburg, Occupational Department, Germany
Citation: F.W. Schardt, B. Schmausser, E. Henke, A. Zernecke-Madsen, (2024), Advances in Therapies against Malignant Cells, International Journal of Clinical Case Reports and Reviews, 20(3); DOI:10.31579/2690-4861/610
Copyright: © 2024, F.W. Schardt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 November 2024 | Accepted: 22 November 2024 | Published: 07 December 2024
Keywords: malignant cells; heparins; fibrinolytics; antiplatelet drugs; fibroblasts
Malignant cells have an uncontrolled growth which follows the activation of oncogenes and deactivation of tumor suppressor genes. All cancer cells produce factors for the clotting system. Malignant cells build up a protective scaffold in form of fibrin meshwork surrounding the tumor cells and produce an extracellular matrix (ECM) consisting of proteoglycans, collagens, glycoproteins, and glycosaminoglycans. They are connected by a countless number of covalent bonds and form an impenetrable scaffold. In addition, malignant cells provide with intracellular signaling pathways like MAPK, FAK, and LOX cell adhesion and migration promoted and supported by hypoxia. Simultaneously, they produce stem cells in an
early cancer stadium, which gain the energy and oxygen for their metabolism from the anaerobic glycolysis and are therefore independent of arterial supply. Encephalin production activates mainly at the beginning a pain modulating system. Many publications show that heparins have a wide variety of efficiencies to tumor metabolism because they have the highest negative charge density of any known biological molecules. Therefore, they should be exogenously added in high dosages. Multiple studies have also shown that heparins combined with clopidogrel and aspirin are able to reduce cancer incidence. Opioids such as D, L methadone induce cell death in malignant cells by downregulation of cAMP and can together with chemotherapy, radiation and biologica destroy tumors and metastasis.
LOX = Lysyloxidase
MAPK= mitogen activated protein kinase
ECM = extracellular matrix
Malignant cells build up a protective shield of a fibrin meshwork surrounding the tumor which helps it to escape the body`s immune system. In addition, tumor and stromal cells (esp. platelets, fibroblasts) provide with an abundant ECM consisting of proteoglycans, collagens, glycoproteins and glucosaminoglycans a further scaffold.
The pathogenesis of hemostatic disorders caused by malignant cells is complex and reflects activation of the coagulation endothelial factors and activation of additional components like platelets and fibroblasts which increase rigidity and stiffness in ECM [1]. Moreover,
tumor escape mechanisms and scaffolds against the immune system are emerged as the most significant barrier to cancer therapy. Therefore, cancer is till now one of the world’s most lethal diseases. [2]
Chronic inflammations cause epigenetic changes such as DNA methylation, demethylation and amination, deamination especially it is relapsing or protracted [3] Our investigations showed that malignant cells are the origin of hypercoagulability by producing fibrin as a protective wall against the immune defence and they inhibit also the fibrinolytic system (Figure D). [4] These fibrin deposits detected by monoclonal antibodies can be also used as diagnostic markers for malignant cells. [5] The proliferation, migration and invasion of cancer cells in various ways will be supported by this fibrin scaffold, too. [6] Therefore thrombosis is often preceding a diagnosed cancer. In consequence to these symptoms, it seems that the migration phase of malignant cells is very early. But it is also a weak point because the malignant cells have in this phase only one scaffold by fibrin [7] in conclusion and basing on our findings, therapies with a fibrinolytic substance (i.e. rt-PA) and heparins should be undertaken to support the therapy with tumor cell antibodies and enhance the phagocytosis. Fibrinolytic and heparins are surely effective in haematological malignancies and during the migration phase of malignant stem and adult cells. Moreover, the high concentration of heparins is obviously the reason that here is nearly no cancer in small intestine although it is a big abdominal organ and 5-6 m long. Heparins are mainly extracted from pork small intestine. The effects of natural or unfractionated heparins are more unpredictable than low-molecular-weight heparin (LMWH) and have the advantage for outpatient treatment. It should be given in the dosage of 200 IE per kg body weight one or two times a day (8,9,10,11). They have a wide variety of positive effects counteracting the scaffolds and immunosuppressive properties of ECM. (Figure. 4) In addition, malignant cells provide with intracellular signaling pathways like MAPK, FAK, and LOX cell adhesion and migration promoted and supported by hypoxia [12,13]
Another property of malignant cells is to escape replicative cell senescense either by producing telomerase or by acquiring another way of stabilizing their telomeres. This has two opposing effects during cancer development. Either telomere shortening can exert a tumor-suppressive effect through proliferation arrest induced by activating kinases. Or the loss of telomere protection can lead to telomere crisis, which is a state of extensive genome instability and promote cancer progression [14].
An additional escape mechanism of malignant cells is to produce encephalins. They control with this endogenous opioid system not only cell proliferation but also activate a pain-modulating system. [15] Maybe, this is the reason that cancer is remarked by the patient yet in a later stadium. In a special study we investigated the anaerobic glycolysis blocking properties of the bisphosphonate zoledronic acid in leukemia and breast cancer cells. [16]. Although, zoledronic acid had little effect at normoxid conditions, it significantly inhibited lactate production at reduced oxygen levels. Under these hypoxid conditions (2%O2) that resembles the oxygenation levels in many tumors especially in bone niches zoledronic acid was also of significantly higher toxicity. Moreover, we showed that it strongly increased the sensitivity to chemotherapy. These results support the Warburg hypothesis of the dependence of malignant cells of anaerobic glycolysis [16].
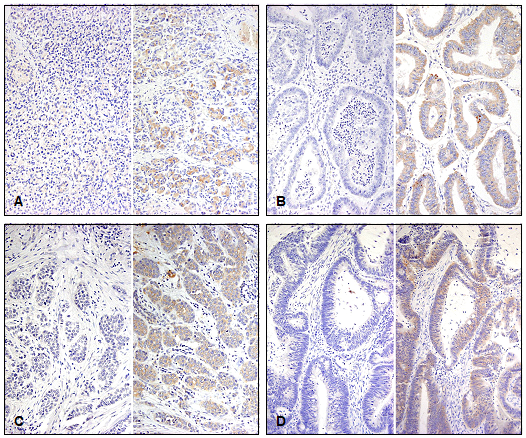
Figure 1: Fibrin was also epressed on tumor cells of
A Pancreatic carcinoma (isotype control x 20, immunohistochemistry)
B Ovarial carcinoma (isotype control x 20, immunohistochemistry)
C Breast carcinoma (isotype control x 20, immunohistochemistry)
D Colon carcinoma (isotype control x 20, immunohistochemistry)
Slides were counterstained by hematoxylin and eosin, x20.

Figure 2: Fibrin was also epressed on tumor cells of
A Leiomyosarcoma (HE x 20)
B Leiomyosarcoma (isotype control x 20)
C Leiomyosarcoma (immunohistochemistry x 20)
D Acute myeloblastic cells HMO2 (immunohistochemistry x 40)
E Gastric carcinoma cell line (isotype control, zytospin MKN 45 x 40)
F Gastric carcinoma cell line (immunohistochemistry, zytospin MKN 45 x 40)
Already 2013 could be shown that D, L methadone activates a opioid receptor and inhibitory G-proteins. The downregulation of cAMP kills and sensitizes leukaemia cells and other malignant cells especially for doxorubicin treatment. Nevertheless D, L-methadon improves the therapy of other malignant diseases as well as the therapy resistant glioma stem cells [17]. A deficient caspase activation was also observed in chemo andradioresistent glioblastoma and other malignant cells treated with radiation or chemotherapy [18]. However, long term observation with monotherapy of D, L-methadone showed relapses of cancers. The reason for that could be the unhindered energy production of the malignant stem or adult cells by the anaerobic glycolysis. This will be interrupted by zoledronic acid every two or three months [19]. Some studies with dual clopidogrel and aspirin treatment supported the hypothesis that both together reduce cancer incidence. There is a feedback or mutual influence between activated platelets induced by ADP, cancer-associated fibroblasts and malignant cells. Therefore, clopidogrel and aspirin are very essential for a successful therapy. [20]. The advantage of the dual therapy over the aspirin-only group was apparent even after adjustment for duration of aspirin therapy. The reason is surely the supplementary effect of both substances. Clopidogrel is an irreversible thienopyridine prodrug inhibiting the P2Y12 subtype of ADP receptors. By this it prevents mainly the release of Ca-ions, fibronectin, fibrinogen, coagulation factors V and XIII and glycoprotein VI by different granules and microtubules. Whereas aspirin acted on two different types of cyclooxygenases, COX-1 (irreversibly) and COX-2 (modified). As additional mechanisms it induces the formation of NO-radicals and reduces leukocyte adhesion [21]. The consequence of all these findings is to prevent the development of this impenetrable ECM by heparins, which have a wide variety of efficiency to tumor metabolism (Figure 4). Additionally, it is necessary to inhibit the activated cells (platelets, fibroblasts) by clopidogrel/ aspirin. The same effects are surely to expect with prasugrel and ticagrelor. The cross-linking of the different kinds of collagens, fibronectins, paxillin, tenascin, nidogen, aggrecan aggregates, decorin, perlecan connected by countless covalent bonds of NH2, COOH, disulfides, NHSO3 andCH2OSO3 are components of ECM [22,23]. Especially around malignant cells of bind web tumors proteoglycans are often composed with glycosaminoglycan chains and covalently tight linked to a core protein [24,25] The high number of covalently bonds in ECM often found in collagen rich sarcoma represents an effective scaffold against the immune system and therapy (Figure 1, A-D; Figure 2, A, B, C, E, F) This tumor extracellular matrix represents a tight and impenetrable network like steel concrete and is surely often the reason for therapy failure [26,27].

Figure 3: Tumor cells with the meshwork of fibrin, activated platelets, cancer associated fibroblasts (ROS = reactive oxygen species, RTK = Ras PI3k pathway) and extracellular matrix with different glycoproteins and proteoglycans (schematically). These substances form by tight connections (FAK, LOX) together with the fibrin meshwork an additional scaffold for malignant cells in the extracellular matrix (ECM). This causes an increase of rigidity and stiffness in the extracellular matrix. GPCRs are also known as G protein-couple receptors.
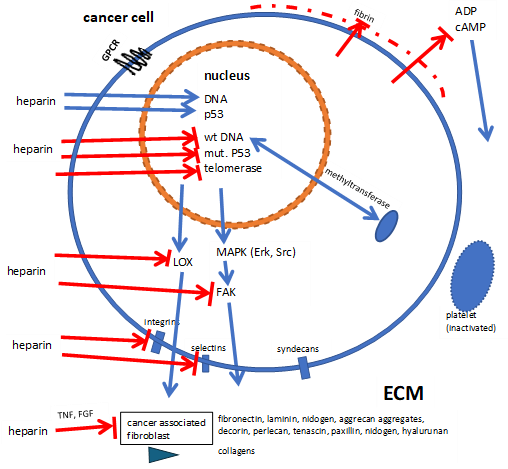
Figure 4: Heparins stimulate (------ ) DNA, p53, and inhibit (-----I) the production of mutated or wild type (wt) DNA, mutated p53 and different glycosaminoglycans, proteoglycans, collagens and glycoproteins depending on the applied dosage. Thereby the formation of scaffolds for malignant cells in ECM are reduced. GPCRs are also known as G protein-couple receptors.
According to the extensive scientific literature and own studies the supplementary therapy to chemotherapy and/or radiation consists of following elements:
1. Sensitization of malignant cells by D/L-methadone
2. Prevention of a network of fibrin and a scaffold of an impenetrable ECM around malignant cells by heparins and fibrinolytics with inactivation of fibroblasts and platelets
3. Prevention of growth/ relapses of metastasis and resources of malignant stem cells by zoledronic acid and heparins.
Based upon available scientific publications, own investigations and studies of the authors a strategy as supplement of the actual oncological therapy was developed with fibrinolytic substances, heparins, antiplatelet drugs, zoledronic acid and methadone by destroying malignant cells and prevention of a cancer induced fibrin network and ECM.
Comparable to malignant cells, still existing medieval fortresses have two walls with different tasks for defence. Therefore, it was the goal of our researches to find possibilities and advances for the therapy against cancer. The weak points of malignant cells and stem cell are the phases of migration and invasion and the anaerobic metabolism.
The authors declare the absence of any conflict of interests.
All authors reviewed the manuscript.
We thank very much Mrs. Dr. Claudia Friesen for her profound investigations about methadone and Mr. Christopher Schardt for text processing and configuration of the figures.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
