
Research Article | DOI: https://doi.org/10.31579/2578-8965/186
1 Tengandogo Teaching Hospital, Burkina Faso.
2 Yalgado Ouédraogo Teaching Hospital, Burkina Faso.
3 Ouahigouya Teaching Hospital, Burkina Faso.
*Corresponding Author: Dantola Paul Kain, Joseph Ki-Zerbo University, 03 BP 7021 Ouagadougou 03, Burkina Faso.
Citation: Dantola P. Kain, Hyacinthe Zamané, Issa Ouédraogo, Sibraogo Kiemtoré, Ali Ouédraogo, et al, (2023), Adolescent Childbirth: Epidemiological and Clinic Aspects, Maternal and Perinatal Prognosis in Tengandogo Teaching Hospital, Burkina Faso, J. Obstetrics Gynecology and Reproductive Sciences, 7(6) DOI:10.31579/2578-8965/186
Copyright: © 2023, Dantola Paul Kain. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 September 2023 | Accepted: 05 October 2023 | Published: 11 October 2023
Keywords: adolescent childbirth; clinic aspect prognosis; tengandogo; burkina faso
Background/Aim: Adolescent pregnancy is considered as a public health issue. This study aims at describing the epidemiological and clinical aspects, as well as the maternal and perinatal prognosis of adolescent childbirth.
Materials and Methods: This was a descriptive and analytical study. Data were collected prospectively. The study population included all women admitted for delivery. Adolescents were sampled exhaustively. In order to identify factors associated with adolescent childbirth, we selected a control group of women aged between 20 and 39.
Results: Adolescent deliveries accounted for 12.6% of all deliveries. The average age was estimated at 18.2 years. Patients aged 19 accounted for 55.1% of cases. Upon admission, 88.9% of adolescent girls were nulliparous. Adolescents were referred in 93.5% of cases. As for admission reasons, abdominopelvic pain with uterine contractions accounted for 39.81% of cases. In 21.3% of cases the gestational age as below 37 weeks of amenorrhea. Fetal breech presentation was observed in 8.3% of cases. Caesarean section was the mode of delivery in 60.2%. In our series, two adolescent girls presented a hemorrhage of deliverance. One case of maternal death was recorded. The prematurity birth rate was estimated at 20.4% and neonatal resuscitation concerned 24.9% of newborns. The perinatal mortality rate is estimated at 11.2% corresponding 112 deaths per thousand births.
Conclusion: Adolescent childbirth, compared to that of adult women is still associated with a poor prognosis. There is the need to enhance appropriate measures in education, contraception, prenatal care and the fight against early marriage need to reduce the rates of early pregnancy and obstetric complications in this high-risk population.
The World Health Organization defines adolescents as young people aged between 10 and 19 [1]. Adolescent pregnancy is considered as a public health issue because of the risk of maternal and fetal morbidity and mortality [2]. About 12.8% of pregnant adolescents are affected by childbirth complications, with eclampsia and post-partum hemorrhage being the most frequent ones and death the major complication [3]. Adolescent pregnancy is also risky for the baby to be born [4]. Therefore, adolescent mothers are more likely to give birth to low-birth-weight babies than adults [4]. The risk of prematurity is higher in mothers aged under 20 than in others [4].
High fertility in adolescent is a concern in Burkina Faso. Indeed, the fertility rate for adolescents aged 15-19 is estimated at 130 per thousand [5]. As a solution to the problem, Burkina Faso has adopted a strategic plan for adolescent health for the period 2015-2020. Despite these measures and strategies, the problem remains persistent, hence the need to conduct in-depth studies on this issue, which is a pressing health concern. This study aims at describing the epidemiological and clinical aspects, as well as the maternal and perinatal prognosis of adolescent childbirth in the mother-child department of the Tengandogo Teaching Hospital (CHUT) in order to contribute to the fight against maternal and perinatal morbidity and mortality.
This was a descriptive and analytical study conducted within the mother-child department of Tengandogo Teaching Hospital. Data were collected prospectively. The study was held from January 1st , to December 31st , 2021. The study population included all women admitted for delivery in the mother-child department of Tengandogo Teaching Hospital during the concerned period. Adolescents were sampled exhaustively. In order to identify factors associated with adolescent childbirth, we selected a control group of women aged between 20 and 39.
The control person of an adolescent who gave birth is the immediate person to have given birth on the delivery register. All the adolescents and control groups had a gestational age of at least 28 weeks' amenorrhea. Data were collected from interviews with patients and/or their companions, from patient clinical records including delivery registers, admission registers and pregnancy follow-up booklets. Study variables were socio-demographic characteristics, clinical data and maternal and perinatal prognostic elements. Refusal to participate in the survey and being admitted for a postpartum complication were the exclusion criteria.
Data entry and analysis were carried out on a microcomputer through KoBoCollect software version 1.30.1. In addition, EPI Info software version 7.2.3.0, Excel and Word from the Microsoft Office package were used for drafting and designing tables. Percentages were compared using the Chi2 test with a significance level of 5%. Odds ratios were also calculated for a confidence interval of 95% to measure the strength of the association between variables. The study was carried out with the authorization from the Director General of Tengandogo Teaching Hospital. Patients ‘informed consent was verbally obtained and the anonymity and total confidentiality of the participants was kept.
During the study period, 216 adolescents gave birth out of a total of 1,714 deliveries in the mother-child department of the Tengandogo Teaching Hospital. Adolescent deliveries accounted for 12.6% of all deliveries.
The average age was estimated at 18.2 years, with extremes of 15 and 19 years. Patients aged 19 accounted for 55.1% of cases. Those living with a partner (married or cohabiting) accounted for 80.5% of cases. Adolescents with at least a post-primary educational level accounted for 52.7% of cases while those with an employment (traders, farmers and salaried employees/civil servants) accounted for 84.2% of cases. Adolescent girls living in urban areas accounted for 74.1% of cases. Upon admission, 88.9% of adolescent girls were nulliparous.
Adolescents were referred in 93.5% of cases. The average number of prenatal consultations was 3.4 with extremes ranging from 0 to 5. Patients had less than 4 prenatal visits in 48.6% of cases. As for admission reasons, abdominopelvic pain with uterine contractions accounted for 39.81% of cases. The distribution of adolescents according to the admission reason is presented in table 1.

Table 1: Distribution of adolescents according to the admission reason (n=216).
In 21.3% of cases the gestational age as below 37 weeks of amenorrhea. Fetal breech presentation was observed in 8.3% of cases. 18.5% of adolescents had a clinically impracticable pelvis. Labor beginning was spontaneous in 88.4% of adolescents. Acute fetal distress was observed in 39.3% of cases. Caesarean section was the mode of delivery in 60.2%. The distribution of adolescents according to cesarean section indications is presented in table 2.
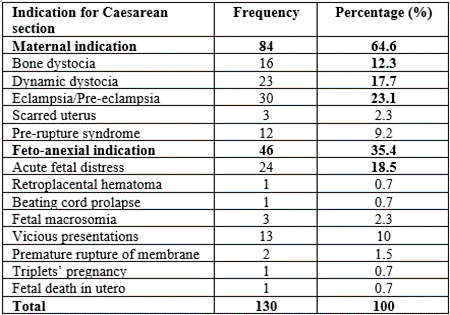
Table 2: Distribution according to caesarean section indication (n=130)
In our series, two adolescent girls presented a hemorrhage of deliverance. 81.4% of the adolescent girls who gave birth vaginally received an episiotomy. 11.6% of adolescent girls who gave birth vaginally had perineal tears. Eight patients corresponding to 3.7% presented an endometritis puerperal infection, 29 adolescent girls with decompensated anemia corresponding to 13.4% of cases were identified. One case of maternal death was recorded.
As for the live births, the APGAR score was less than 7 at the 1st minute in 19.9% of cases. The average weight was 2645 grams and low birth weight concerned 31.1% of newborns. The prematurity birth rate was estimated at 20.4% and neonatal resuscitation concerned 24.9% of newborns. At the end of delivery, 21 stillbirths were recorded corresponding to 9.3% among which 16 fresh stillbirths and 5 macerated stillbirths. The total number of early neonatal deaths was 4 corresponding to 2% of cases. The perinatal mortality rate is estimated at 11.2% corresponding 112 deaths per thousand births.
In multivariate analysis, there was a statistically significant association at a 5% threshold between adolescent birth and certain factors. The results of this analysis are presented in tables 3 and 4.
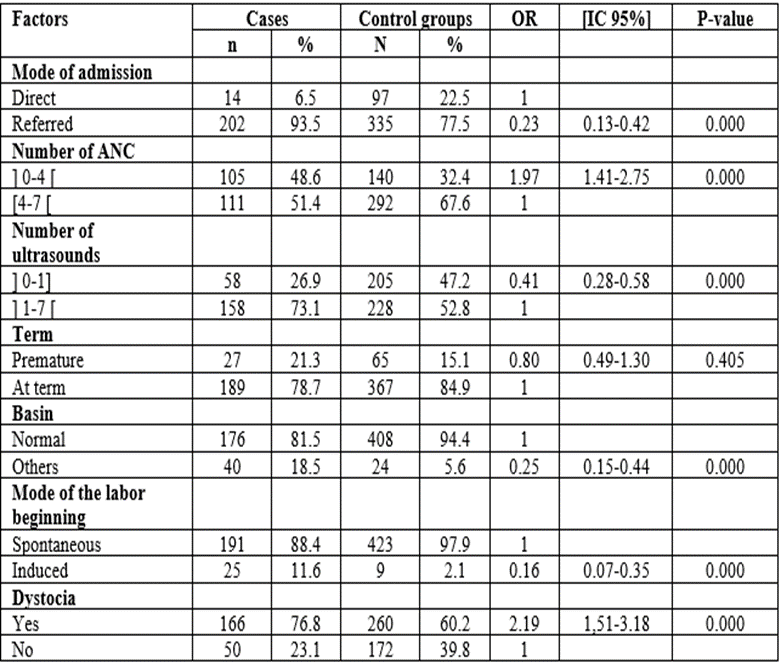
Table 3: Factors associated with ado delivery in multivariate analysis
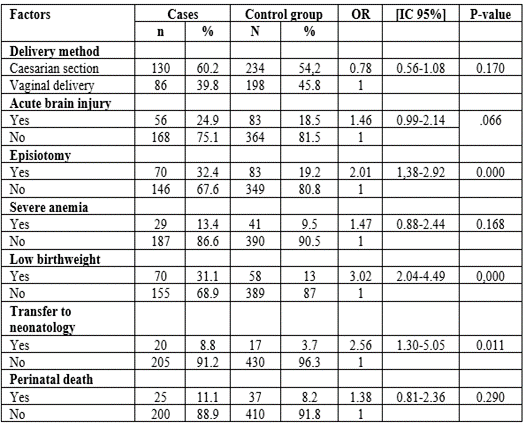
Table 4: Factors at childbirth in adolescents in multivariate analysis (continued).
The number of prenatal consultations between 0 and 4 was higher in adolescent patients than in adult ones, respectively with proportions of 48.6% and 32.4%. The difference was statistically significant (p=0.000). Compared with adult patients, adolescents have achieved less than 1.9 times prenatal consultations. Dystocia was more frequent in adolescent patients than in adult ones, respectively with proportions of 76.8% and 60.2%. The observed difference was statistically significant (p=0.000). In comparison with adult patients, adolescent ones were 2.19 times more likely to experience dystocia (OR=2.19; CI=1.51-3.18).
Episiotomy was more common in adolescent patients than in adult ones respectively with proportions of 34.4% and 19.2%. The difference was statistically significant (p=0.000). Adolescent patients were 2 times more likely to have an episiotomy than adult ones. The proportion of low birth weights (birth weight below 2500g) in newborns of adolescent mothers was estimated at 31.1%, against 13% in adult ones. The difference observed was statistically significant (p=0.000). The risk of adolescent mothers delivering a low birth weight baby was estimated at 3 (OR =3.02; CI=2.04-4.49). 8.8% of newborns from adolescent mothers were transferred to neonatology against 3.7% of newborns born from adult mothers. The difference observed between the two proportions was statistically significant (p=0.011), with newborns from adolescent mothers 2.5 times more likely to be transferred to neonatology (OR=2.56; CI=1.30-5.05).
Our frequency is close to those reported by Traoré et al [6] in Mali, and Nayama et al [7] in Niger who respectively found 15.5% and 10.9%. It is higher than those reported by Leno DWA et al [8] in Guinea, and Soula [9] in Guyana, whose respectively are 2.6% and 2.7%. However, it is lower than the one found by Nguembi [10] in Central Africa, which was estimated at
30.3%. The high rate pregnancy and childbirth among adolescents observed in several African countries is related to several factors such as poverty, illiteracy and early marriage.
The average age of the adolescent girls of our study was estimated at 18.2 years, a result similar to those of Foumsou L et al [3] in Chad, Ouédraogo. A [11] in Burkina Faso and Sepou A et al [12] in Central African Republic, which were respectively estimated at 17.2, 17.9 and 17.8 years. However, Iloki [13] in Congo, Aboubacary [14] in Togo and Ba MG [15] in Senegal found lower average ages respectively estimated at 14.5, 15.1 and 15.5 years. This variability in the average age is explained by the disparity in the definition of the adolescence age limit, which was set at 19 years for Foumsou [3] and Sepou [12], while Iloki’s [13] and Aboubacary ‘s [14] have set the upper limit at 17 years.
80.5% of adolescent girls in our study were married. These figures are in line with African literature data. Nayama et al [7] in Niger, Hamada et al [16] in Morocco and Traoré et al [6] in Mali have respectively found proportions of 77.2, 90.3 and 81.7. However, this rate is still higher than the one reported by Iloki et al [13], who found 16%. This high rate could be due to early marriage since African society does not generally tolerate pregnancy among unmarried women, and to certain social determinants such as mores, poverty, illiteracy and religious beliefs in Africa.
In our study, 48.6% of patients have achieved less than four antenatal visits. WHO [17] recommends to have at least 4 antenatal consultations during the nine months of pregnancy. Our data are in line with those from the literature. As an example, Iloki et al [13] in Congo, and Hamada et al in Morocco [16] respectively have found 22.1% and 22.6% of unfollowed pregnancies. In addition to the various age-related risks, there is also a significant risk of late detection of complications due to unfollowed pregnancies. This situation highlights the need to monitor pregnancies so that to identify any complications in good time.
As for the delivery mode, the results of our study have showed that 60.2% of deliveries were made by caesarean section. This rate is higher than those reported by Ayuba [18] in Nigeria, Traoré B et al [6] in Mali and Foumsou L et al [3] in Chad, who respectively found 23.9%, 21.4% and 17.5%. The high caesarean section rate in our series could be explained by the fact that our study took place in a hospital of last resort, where almost all parturients referred to us required surgical management.
Perinatal morbidity was assessed through prematurity, birth weight, Apgar score, notion of resuscitation and transfer to neonatology.
The prematurity rate observed in our series was estimated at 20.4%. Our rate is higher than that of Luhete [19] in Congo Brazzaville, who found 12.7% of premature babies born from adolescent mothers. Iacobelli [20] found an increased risk of prematurity among adolescent girls and even believes that there is a direct correlation between the mother's age and the risk of prematurity.
As for birth weight, the proportion of low-birth-weight newborns was 31.1%. Nayama [7] in Niger and Niang et al [21] in Senegal found rates similar to ours with respectively 28.7% and 36.1%. Some authors agree that low birth weight is a major characteristic of children born from adolescent mothers. Fraser AM [22] describes a nutritional competition between the young mother whose growth process is still underway and her fetus.
The Apgar score is one of the objective methods for assessing the newborn condition at birth. It enables to establish an early diagnosis of neonatal distress. In our study series, this first-minute score was above 7/10 in 80.1% of cases. Newborns with a poor score accounted for 19.9% of cases. Obstetric pathologies during labor and parturients’ indocility during the expulsion phase could explain this rate. The perinatal mortality rate was estimated at 11.2%, a result similar to those of Nayama et al [7] and Foumsou et al [3], who respectively found 11.2% and 12.7% . However, it is higher than that of Traoré et al [6], who found 9.3%. Low birth weight, neonatal distress and adolescent primiparity are interrelated factors with high perinatal mortality risk.
As limitations of the study we note a selection bias: the age of the patients was obtained by questioning. The comparison of this with that recorded on the national identity card having not been done, this could be the origin of a bias.
The frequency of pregnancy among adolescents remains high. Adolescent childbirth, compared to that of adult women is still associated with a poor prognosis. There is the need to enhance appropriate measures in education, contraception, prenatal care and the fight against early marriage need to reduce the rates of early pregnancy and obstetric complications in this high-risk population.
The studies involving human participants were reviewed and approved by the authorization of the ethics committee. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Kain DP and Zamané H prepared the manuscript, Ouédraogo I collected the data, Kiemtoré S. analyzed the data, Ouédraogo A and Thiéba/Bonané B provided a useful review of this manuscript. All authors contributed to the article and approved the submitted version.
The authors would like to thank all patients for their consent obtained. The authors also thank all the staff who contributed to the care of the patients.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
