
Review Article | DOI: https://doi.org/10.31579/2768-2757/130
Breast Onco Surgery Unit, Sugical Oncology Depatment, B.P. Koirala Memorial Cancer Hospital, Bharatpur, Nepal.
*Corresponding Author: Deepak Singh Mouni., Breast Onco Surgery Unit, Sugical Oncology Depatment, B.P. Koirala Memorial Cancer Hospital, Bharatpur, Nepal.
Citation: Deepak S Mouni., Shrestha S., Adhikari A., (2024), Adenomyoepithelioma of the Breast: A Rare Case Report from B.P Koirala Memorial Cancer Hospital., Journal of Clinical Surgery and Research, 5(6) DOI:10.31579/2768-2757/130
Copyright: © 2024, Deepak S Mouni. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 July 2024 | Accepted: 22 July 2024 | Published: 16 August 2024
Keywords: adenomyoepithelioma; asymptomatic; benign mass; case report; surgical excision
Adenomayoepithelioma is a rare, benign breast neoplasm characterized by the proliferation of both epithelial and myoepithelial cells within the breast lobules and ducts. Although it is most commonly seen in salivary glands and skin, Hamper reported the first case in the breast in the 1970 (1). While this benign tumor is predominantly found in older females, rare cases have been identified in young women as well. Adenomayoepithelioma is notorious for local recurrence, and malignant metastasis has been reported (2). Adenomayoepithelioma is very rare case and in 10 years period, out of 19000 cases treated in OPD , we have encountered only 2 cases of Adenomayoepithelioma, one was referred case & another one was diagnosed at our center.
A 35 years old female presented to the out patient department with the chief complaint of painless lump in the upper outer quadrant of the right breast that had been present for the past 1and half months. The patient had no history of pain, nipple discharge, skin changes or increase in the size of the mass. The patient had no personal history of oral contraceptive pills (OCP) intake ,is non smoker, non alcoholic and no family history of breast tumors .On examination, a 2 x 1.5 cm, firm, well defined, round, partially mobile lump with a smooth margin was palpated over the upper outer quadrant of the breast, with no skin changes .Ultrasonography revealed an ill-defined, heterogeneous lesion measuring 20 x 14 x 13mm in the fibroglandular tissue of the right breast at the 7 to 8 o'clock position, with minimal vasculature noted within the lesion.A fine-needle aspiration cytology (FNAC) was performed and showed features consistent with a benign proliferative disease of the breast, specifically a fibroadenoma.The patient underwent wide local excision under intravenous anesthesia and was discharged on the same day with no postoperative complications. The histopathology report revealed adenomyoepithelioma, with immunohistochemistry markers showing P63 diffusely immunoreactive in the myoepithelial component,S-100 diffusely immunoreactive in the myoepithelial component, and HMWCK immunoreactive in the epithelial component. The proliferation index Ki-67 was 1-5%. ER was patchy immunoreactive in 10-15% of neoplastic cells.The patient has been advised to undergo strict six-monthly follow-up with ultrasound of the breast and axilla to monitor for local recurrence and metastatic spread.
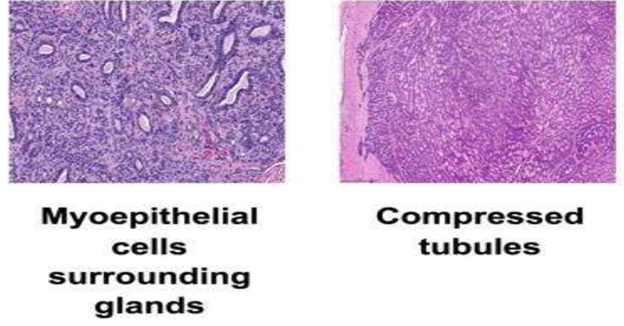
Adenomyoepithelioma can be classified into three types: tubular, lobulated, and spindle cell. Tubular adenomyoepithelioma has an ill-defined margin, similar to tubular adenoma. Lobulated
adenomyoepithelioma presents as nests of myoepithelial cells surrounding compressed epithelial-lined spaces. Spindle cell adenomyoepithelioma shows sparse epithelial-lined spaces that resemble leiomyomalike cells. (3)
Diagnosis:
Adenomyoepitheliomas typically presents as a single, palpable, well-circumscribed, firm mass, with dimensions of up to 8 cm. Microscopic satellite lesions may be present in the periphery of the tumor at times, but it is mostly located in the central portion. Rarely, adenomyoepitheliomas may also present in phyllodes tumor or fibroadenoma. Pain and nipple discharge are rare symptoms associated with adenomyoepitheliomas. (15)
Radiology evaluation:
Radiology imaging is not specific and cannot distinguish between benign and malignant lesions (2).Ultrasonography (USG) shows that adenomyoepitheliomas are typically solid or have a combined solid and cystic appearance. On mammography, they present as a lobulated dense mass with a partially indistinct margin, with or without calcifications. Malignant adenomyoepitheliomas show irregular shapes with spiculated margins on mammography. (14)
Pathology evaluation:
FNAC and core needle biopsy are also rarely diagnostic due to the heterogeneity of the tumor, with many cases falsely diagnosed as fibroadenoma in the literature. However, the presence of tightly aggregated glands arranged in compact nodules and prominent clear cell or spindle cell myoepithelium can be clues to the diagnosis. (4) (8) (13)
Micrscopic description of adenomyoepithelioma: (10)
Immuno Histo chemistry (IHC):
IHC is an important tool in the diagnosis of adenomyoepithelioma. The panel of markers, including p63,S-100, and HMWCK.P63 is a transcription factor that is expressed in the nuclei of myoepithelial cells and is a very sensitive and specific marker for identifying these cells. In adenomyoepithelioma, P63 staining is typically positive and shows a consistent rim of staining around the epithelial cells, which can help to distinguish it from other breast tumors. Ki-67 proliferation index is also useful in predicting the recurrence rate of the tumor. ER, PR, and HER-2 are usually negative in malignant adenomyoepithelioma. (6) (7) (9)(12)
Differential diagnosis:
Treatment
No specific guidelines have been established for the treatment of adenomyoepithelioma. However, wide local excision with negative margins is recommended due to the local recurrence nature of the tumor.Some cases of malignant adenomyoepithelioma have also been reported in the literature, where mastectomy and sentinel lymph node biopsy are recommended. (10) (11)
Prognosis
Benign adenomyoepitheliomas generally have a good prognosis but require close monitoring and followup. In cases of local recurrence, radiotherapy has been used with positive results. However, malignant adenomyoepithelioma has a poor prognosis due to its low-grade invasiveness, high recurrence rate, and resistance to chemotherapy. Malignant tumors are more likely to metastasize via hematogenous spread to distant organs such as the brain, liver, and lungs rather than through the lymphatic system. (10) (11)
Adenomyoepitheliomas (AMEs) are rare benign breast tumors that should be considered in the differential diagnosis of solid breast lumps. While imaging features are not specific, suspicion of benign or malignant nature can be raised through radiologic examination. FNAB is often not diagnostic.
Currently, there are no established guidelines for treating either benign or malignant AME. Surgical excision with negative margins is recommended for both types of AME due to the high recurrence rate for benign tumors and the aggressiveness of malignant ones. Close monitoring and follow-up are necessary for benign cases, while malignant cases have a poor prognosis and are characterized by low grade, invasiveness, and high recurrence rate. Chemotherapy is not effective for treating malignant AME, and metastasis occurs through hematogenous spread to organs such as the brain, liver, and lungs.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
