
Review ariticle | DOI: https://doi.org/10.31579/2690-1897/183
North Manchester General Hospital, Department of Urology, M8 5 Rb, Manchester United Kingdom.
*Corresponding Author: Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, M8 5 Rb, Manchester United Kingdom.
Citation: Grey Venyo AK, (2024), Adenocarcinoma of Seminal Vesicle: Review and Update, J, Surgical Case Reports and Images, 7(4); DOI:10.31579/2690-1897/183
Copyright: © 2024, Anthony Kodzo-Grey Venyo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 April 2024 | Accepted: 06 May 2024 | Published: 10 May 2024
Keywords: primary adenocarcinoma of seminal vesicle; prostate cancer; bladder cancer; adenocarcinoma of rectum; biopsy; microscopy; histopathology; immunohistochemistry; papillary architecture
Primary adenocarcinoma of the seminal vesicle is a rare condition with only approximately 60 cases reported in the literature. The unusual characteristics of the neoplasm makes its diagnosis difficult and treatment strategies differ as there are no specific guidelines available. Diagnosis of primary adenocarcinoma of prostate gland is confirmed microscopically. Primary adenocarcinoma neoplasms of the seminal vesicle are localized primarily within the seminal vesicle and in order to confirm a diagnosis of primary adenocarcinoma of seminal vesicle, it is important to exclude invasion of malignant neoplasm from the prostate gland (by undertaking PSA / PAP tests), the rectum or other sites of the body. Primary adenocarcinoma of seminal vesicle usually exhibits a papillary adenocarcinoma simulating the architecture of normal seminal vesicle. Primary adenocarcinoma of seminal vesicle resembles prostatic duct adenocarcinoma Gleason patterns 3 or 4 or mucinous (colloid) carcinoma. Primary adenocarcinoma of seminal vesicle, is usually unresectable and patients who are afflicted by primary adenocarcinoma of seminal vesicle die within 2 years. The ensuing article has discussed in detail various aspects of primary adenocarcinoma of seminal vesicle, including an overview of primary adenocarcinoma of seminal vesicle, as well as miscellaneous narrations and discussions from some case reports, case series, and studies related to primary adenocarcinoma of seminal vesicle.
Yin et al. [1] stated the following:
Considering the rarity of PSVA, it would be envisaged that majority of clinicians all over the world would not have encountered or managed a case of PSVA before. The ensuing article on primary adenocarcinoma of the seminal vesicle is divided into two parts: (A) Overview which has discussed general overview aspects of adenocarcinoma of seminal vesicle and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to primary adenocarcinoma of the seminal vesicle.
To review and update the literature on primary adenocarcinoma of the seminal vesicle.
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Adenocarcinoma of seminal vesicle; seminal vesicle adenocarcinoma; carcinoma of seminal vesicle; and seminal vesicle carcinoma. --- references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed general overview aspects of adenocarcinoma of seminal vesicle and (B) Miscellaneous narrations and discussions from some case reports, case series and studies related to primary adenocarcinoma of the seminal vesicle.
[A] Overview
Definition / general statements
The ensuing general statements and definition had been provided on primary adenocarcinoma of seminal vesicle: [8]
Epidemiology [9]
It has been iterated that primary adenocarcinomas of the seminal vesicles are very rare [9] [10] [11] and they could be observed at a wide age range [9] [11].
Diagnostic criteria [9]
The following modified diagnostic criteria have been described for diagnosis [1] [11]:
Clinical Manifestation [9]
Complications [9]
Macroscopy pathology examination appearance [9]
Microscopy pathology examination appearance
It has been iterated that for a diagnosis of primary adenocarcinoma of the seminal vesicle to be made, microscopically, the tumours need to be consistent with adenocarcinomas [9] [13]. The histological examination features had been summated to include the following: [9] [11]:
Immunophenotype [9]
Markers [9]
Immunohistochemistry studies summations related to primary adenocarcinoma of seminal vesicles: [8]
Positive stains
It has been iterated that primary adenocarcinoma tumour cells exhibit positive staining for: [8]
Negative stains
It has been iterated that primary adenocarcinoma tumour cells exhibit negative staining for: [8]
Radiographic features [9]
Computed Tomography (CT) scan [9]
Magnetic Resonance Imaging (MRI) scan [9]
Nuclear Medicine [9]
Radiology Report [9]
It has been advised that the radiological report of primary adenocarcinoma of seminal vesicle should include a description of the following: [9]
Treatment and prognosis [9]
History and etymology [9]
Differential diagnoses [9]
Some of the conditions simulating the clinical manifestation or radiology imaging appearance of primary adenocarcinoma of the seminal vesicles had been summated to include [10]
Differential diagnoses extra information
The ensuing summating documentations had been made about the differential diagnoses of primary adenocarcinoma of seminal vesicles: [8]
[B] Miscellaneous narrations and discussions from some case reports, case series, and studies related to primary adenocarcinoma of seminal vesicles.
Yin and Jiang [1] reported a 51-year-old man who did not have any history of past illness whose main manifestations were repeated hemospermia over the preceding 2 years and haematuria over the preceding 2 weeks and who came to Tongji Hospital in July 2012. His clinical examination, including digital rectal examination (DRE), did not demonstrate any abnormal findings. He had pelvic MRI scan which demonstrated a mass with mixed cystic and solid signals in the district of the right seminal vesicle (see figure 1A). No distant metastases were found in this patient. The results of his serum tumour markers had indicated that his carcinoembryonic antigen (CEA) and serum PSA levels were both normal, while CA-125 levels were above normal at 137 U/mL. Surgery was undertaken, and a tumour with a diameter of about 4 centimetres with an unclear border was identified adherent to the peripheral tissue and was carefully removed. Local lymphadenectomy was not undertaken. Post-operative histopathology examination of the excised specimen confirmed the diagnosis of primary seminal vesicle adenocarcinoma (PSVA) with immunohistochemistry (IHC) staining of that was negative for CEA, negative for PSA, and positive for CA-125 (see figures 2A to 2E). Unfortunately, the tumour was not resected en bloc according to the surgeon and was confirmed by a post-surgery MRI scan (see figure 1B) that demonstrated a ring-like cystic cavity with marginal enhancement above the prostate, behind the bladder, and in front of the rectum. After a multidisciplinary team discussion, 3 cycles of chemotherapy utilising a regimen of 150 mg/m2 paclitaxel plus 60 mg/m2 cis-platinum were undertaken; then, radical pelvic radiotherapy with a dose of 60 Gray in 30 fractions was carried out followed by 3 cycles of the same chemotherapy. The draining lymph node was not prophylactically eradiated since pre-surgery MRI imaging had shown no metastasis to the lymph node. Concurrent chemoradiotherapy was not considered in view of the fact that there was no evidence to support its use at that point. The side effects of sequential chemotherapy and radiotherapy were acceptable, and no severe adverse effects were observed in the patient. Endocrine treatment was not provided to the patient. After completion of his treatment, the patient was assessed every 3 months in the first year and every 6 months in the following 2 years (see figures 1C and 1D. His last follow-up was November 2017 (see figure 1E). The authors reported that the patient was still disease-free, and he had been followed for longer than any other PSVA patient in a published report.
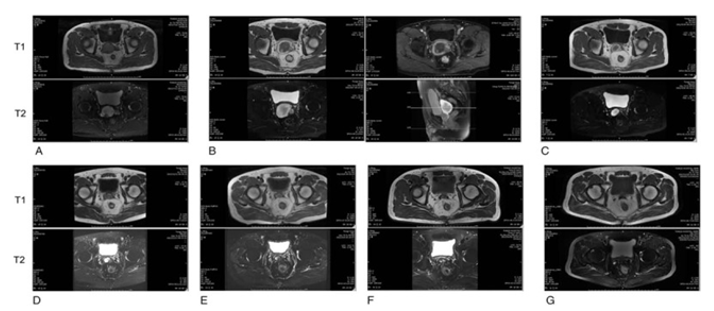
Figure 1: Reproduced from: [1] Medicine (Baltimore). And Wolters Kluwer Health, Inc. for granting permission for reproduction of contents of their journal article under copyright: Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial License 4.0 (CCBY-NC), where it is permissible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc/4.0 Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6203478/ Representative MRI for the patient. (A), pre-surgery; (B), post-surgery; (C), after 2 cycles of chemotherapy; (D), after 3 cycles of chemotherapy plus radiotherapy; (E), 6 months after surgery; (F), 1 year after surgery; (G), 5 years after surgery, T1, MRI T1 weight; T2 , MRI T2 weight. Reproduced from:

Figure 2: Reproduced from: [1] Medicine (Baltimore). And Wolters Kluwer Health, Inc. for granting permission for reproduction of contents of their journal article under copyright: Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial License 4.0 (CCBY-NC), where it is permissible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc/4.0 Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6203478/
Representative pathology images of the patient’s tumour by haematoxylin and eosin (HE) staining and IHC.A, HE staining; (B-E) IHC of CA-125, CEA, CK7, and CDX-2 respectively. 10 x amplified; 40 x, 40 times amplified. Reproduced from:
Yin and Jiang [1] made the ensuing educative discussions:
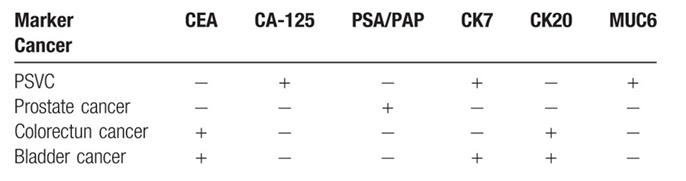
Table 1. Reproduced from: [1] Medicine (Baltimore). And Wolters Kluwer Health, Inc. for granting permission for reproduction of contents of their journal article under copyright: Copyright © 2018 the Author(s). Published by Wolters Kluwer Health, Inc. This is an open access article distributed under the terms of the Creative Commons Attribution-Non-Commercial License 4.0 (CCBY-NC), where it is permissible to download, share, remix, transform, and buildup the work provided it is properly cited. The work cannot be used commercially without permission from the journal. http://creativecommons.org/licenses/by-nc/4.0 Link: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6203478/
Common IHC marker for cancer.
Yin and Jiang [1] made the ensuing conclusions:
Bhat et al. [28] stated the following:
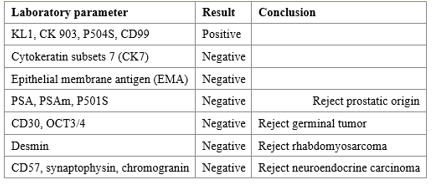
Terrisse et al. [29] reported a 43-year-old man, who had manifested with azoospermia, perineal insensitivity, lumbar pain and rectal pus, which he had been suffering over the preceding 6 months. His clinical examination demonstrated small testicles and his digital rectal examination revealed an enlarged prostate gland with no fixed adenoma. His Prostate specific antigen (PSA) level was 1.52 ng/mL He had MRI scan of his prostate gland, which demonstrated non-specific abnormalities with: an enlarged prostatic gland, heterogeneous signal in left central and transitional parts of the prostate and loss of seminal-prostatic and deferent differentiation. He had trans-rectal biopsies of the prostate gland and pathology examination of the biopsy specimens revealed a poorly differentiated carcinoma, probably of glandular origin. The immunohistochemistry staining study results are illustrated in Table 2. Based upon these data, the diagnosis of a poorly differentiated carcinoma of probably urothelial origin with massive prostate extension was confirmed.
Table 2. Reproduced from: [29] Terrisse S, Camblor ME, Vérine J, Gauthier H, Mongiat-Artus P, Culine S. Primary adenocarcinoma of the seminal vesicle. Rare Tumors. 2017 Oct 3;9(3):7074. doi: 10.4081/rt.2017.7074. Erratum in: Rare Tumors. 2019 May 03;11:2036361319848842. Comblor, Maria Eugenia [corrected to Camblor, Maria Eugenia]. PMID: 29081928; PMCID: PMC5643883. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5643883/
©Copyright S. Terrisse et al., 2017 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Immunohistochemical analysis of prostate biopsies in patient.
He had complementary assessment with computed tomography (CT) scan of thorax, which demonstrated a nodule in the left superior lobe of the lung. He had PET scanning which did not demonstrate any other metastasis. At that point, the patient had experienced an exacerbation of the symptoms with visible haematuria and perineal pain. Due to fast clinical evolution and risk of incomplete resection of the lung nodule, the patient underwent primary chemotherapy. He received six cycles of MVAC dose dense regimen (Methotrexate 30 mg/m2 D1, Cisplatin 80 mg/m2 D2; Vinblastine 3 mg/m2 D2, Doxorubicin 30 mg/m2 D2) once every 15 days. He had an excellent clinical response following his first chemotherapy cycle. A radiology imaging response was obtained following his fourth cycle with partial response at the pelvis and complete pulmonary response. Dose reductions of Cisplatin at 50 mg/m2 were made during the fifth and sixth cycles in view of his moderate renal insufficiency (creatinin: 166 umol/L vs 85 umol/L at Cycle 1). One month following the end of his chemotherapy sessions, the patient underwent surgical resection, by means of a cystoprostatectomy with an extended pelvic lymphadenectomy and an enterocystoplasty. The fiinal histopathology examination of the excised surgical specimen demonstrated a carcinoma proliferation which was centred upon the seminal vesicles, negative for CK7, CK20, PSA, P63 and P504S. The lesion was diagnosed and classified as an adenocarcinoma of the seminal vesicles with invasion of the prostate gland and the lower part of the urinary bladder. The margins of the resected specimen were described as negative, without lymph nodes metastases. Two months pursuant to his surgery, the patient was still under observation when a new, 10-mm lung nodule was found, which grew to 21 mm within two months subsequently. He underwent atypical complete resection of the nodule in the left superior lobe and the immunohistochemistry confirmed a metastasis of an adenocarcinoma of the seminal vesicle. He subsequently regained control over the disease and during his last follow up visit, he was in persistent complete remission 4 years pursuant to his pulmonary metastasectomy.
Terrisse et al. [29] made the ensuing educative discussing summations:
Terrisse et al. [29] made the ensuing conclusions:
Tanaka et al. [35] reported a rare case of primary adenocarcinoma of the seminal vesicle in an 87-year-old Japanese man. The neoplastic cells, especially poorly differentiated cells, exhibited a positive reaction with periodic acid-Schiff reagent and anti-carcinoembryonic antigen. The tumour cells had invaded the urinary bladder wall but not the prostate gland. No other primary tumour was identified.
Itami et al. [36] reported a 70-year-old man who manifested with visible haematuria and hematospermia, who was admitted for further assessment of a cystic formation of his right seminal vesicle, that measured 3.6 cm in diameter, which was detected by magnetic resonance imaging (MRI). He underwent cystoscopy which demonstrated no remarkable change, but his urine cytology was class III. His serum concentration of prostate specific antigen (PSA) was within the normal range of 1.83 ng/ml. He had trans-perineal needle biopsy of the prostate and cystic tumour of the seminal vesicle and pathology examination of the biopsy specimens revealed adenocarcinoma of the prostate gland and seminal vesicle, but immunostaining for PSA was negative, so a diagnosis of primary adenocarcinoma of the seminal vesicle was made. Bloody fluid of the cyst was obtained by trans-perineal aspiration, but no cancer cells were identified by cytological examination. Total prostatectomy was undertaken, and the pathological finding was infiltration of prostate cancer into the seminal vesicle (pT3b) because immunostaining of the PSA was positive.
Stenzel et al. [37] stated that criteria for the very rare diagnosis of primary seminal vesicle carcinoma had traditionally been highly stringent but may be relaxed with the application of immunohistochemistry to the diagnosis of mass lesions which occur within the male pelvis. Stenzel et al. [37] reported a case of disseminated carcinoma with a clinically occult primary site which apparently had its origin within the seminal vesicle. He had autopsy which demonstrated a 10-cm tumour enveloping the prostate and seminal vesicles without involvement of colonic or urothelial mucosa. Much smaller tumours were found present within other sites outside the pelvis. The tumour was noted to be composed of poorly formed glands and sheets of malignant-appearing cells, involved the seminal vesicle, and had the immunohistochemical profile of seminal vesicle carcinoma, notably strong immunoreactivity for CA-125 and no immunoreactivity for cytokeratin-20 or prostate-specific markers.
Ormsby et al. [6] stated the ensuing:
Ormsby et al. [6] immunostained four cases of SVCA-three cases of bladder adenocarcinoma and a rare case of adenocarcinoma arising in a mullerian duct cyst for CA-125, CK7, and CK20. Ormsby et al. [6] reported the results as follows:
Ormsby et al. [6] concluded that:
Conclusions
Primary adenocarcinomas of the seminal vesicle is an extremely rare malignant neoplasm which afflicts the seminal vesicle in that so far it does appear form the literature that only about 60 cases of the tumour had been reported.
Nil
Acknowledgements to:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
