
Case Report | DOI: https://doi.org/10.31579/2641-0419/123
1Institutions: University of Iowa Health Care
2 Institutions: Augusta University
3 Institutions: Cincinnati Good Samaritan Hospital.
4 Institutions: Cincinnati Good Samaritan Hospital.
5 Institutions: Cincinnati Good Samaritan Hospital and Trihealth health system.
*Corresponding Author: Ali Alkhayru, MD Adult Hospitalist Program. Department of Internal Medicine University of Iowa Health Care
Citation: Ali Alkhayru, Adria Madera-Acosta, Bassman Tappuni, Belal Kaseer, Kamal Shemisa (2021) Addressing Stroke Risk in a Patient with CREST Syndrome and Atrial Fibrillation with Left Atrial appendage Occluder Device (WATCHMAN). J. Clinical Cardiology and Cardiovascular Interventions, 4(1); Doi:10.31579/2641-0419/123
Copyright: © 2021 Ali Alkhayru, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 December 2020 | Accepted: 28 December 2020 | Published: 06 January 2021
Keywords: crest syndrome; atrial fibrillation; watchman device; gastrointestinal hemorrhage
CREST syndrome is rare autoimmune disease causing calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly and telangiectasias. We present a case of an eighty-two year old female with CREST syndrome who presented to our clinic with atrial fibrillation and prohibitive bleeding risk. Managing stroke risk in atrial fibrillation is essential to minimize the morbidity and mortality of the condition. Those with CREST syndrome presenting with recurrent gastrointestinal bleeding may require alternatives to anticoagulation. Recently, the left atrial appendage occluder device became widely used to manage patients at increased risk for bleeding. The device provides a safe and efficacious alternative in lowering atrial fibrillation associated stroke risk. Our patient underwent uncomplicated implantation of the left atrial appendage occluder device. She was closely monitored for one year where she remained stroke free and had one minor episode of gastrointestinal hemorrhage.
Short Title: CREST syndrome and stroke
CREST syndrome is a variant of scleroderma that is characterized by calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly and telangiectasia. Patients with CREST syndrome often suffer from cardiovascular diseases including coronary artery disease, myocardial fibrosis, primary pulmonary hypertension and arterial embolization [1].
Atrial fibrillation raises stroke risk. it is estimated that about 87% of strokes are ischemic in nature and atrial fibrillation is the underlying cause of 15-20 % of cases [2]. Management of this risk usually requires long-term anticoagulation if the CHA2DS2Vasc score is elevated (>2 in men and >3 women) [3]. However, in certain susceptible patient populations, long term anticoagulation can significantly raise the risk for spontaneous hemorrhage [4]. We present a case of a patient with CREST syndrome who suffered from atrial fibrillation and encountered recurrent bleeding due to multiple gastrointestinal telangiectasias.
Case report:
An eighty-two year old female with past medical history of CREST syndrome, diabetes mellitus, hypertension and permanent atrial fibrillation presented to the cardiology clinic after hospitalization for atrial fibrillation. She was previously treated with a rhythm control strategy and while on amiodarone, underwent two successive cardioversions. She maintained sinus rhythm for three months after the second cardioversion but presented to the hospital with increasing shortness of breath and melena and was found to have recurrent atrial fibrillation and severe microcytic anemia with a hemoglobin concentration of 6.4 grams/dl.
On evaluation she was hemodynamically stable and in mild respiratory distress. She was transfused three units of packed red blood cells and apixaban was discontinued. The hemoglobin increased appropriately to 9 grams/dl after transfusion. Administration of the apixaban reversal agent, adexanetalfa, was therefore differed. She was evaluated by our gastroenterologists with esophagogastroduodenoscopy (EGD) and a colonoscopy. The EGD revealed multiple small nonbleeding telangiectasias along the duodenum, cecum and ascending colon. These areas were successfully cauterized, and daily pantoprazole was recommended.
She was not a candidate for anticoagulation during this period. We estimated the stroke risk attributed to atrial fibrillation using the CHA2DS2VASc score which was five estimating a stroke risk of approximately 6.7% in the first year [3]. The HAS-BLED bleeding risk score was seven estimating a bleeding risk is 3.74% in the first year while on anticoagulation. Although resuming anticoagulation would have effectively addressed the stroke risk, she was high risk for recurrent and potentially life-threatening gastro-intestinal hemorrhage. Thus, we considered procedural options in the management of stroke risk associated with atrial fibrillation.
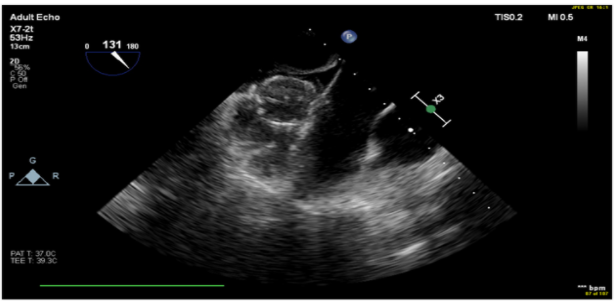
Treatment with the left atrial appendage occlusion device shortens the duration for anticoagulation to 45 days and thus minimizes the risk for bleeding. Because of recurrent bleeding, elevated stroke risk and risk of rebleeding, she was considered a suitable candidate for the left atrial appendage occluder device, (WATCHMAN device). A transesophageal echocardiogram demonstrated a left atrial appendage with “windsock” morphology, anatomically suitable for left atrial appendage closure. The right ventricular systolic pressure was 30 mmHg. She underwent successful deployment of the WATCHMAN device using standard technique (Figure 1, and Figure 2).

She was then anticoagulated with warfarin for 45 days following the device placement and did not suffer gastrointestinal hemorrhage during that period [5]. She was followed for one year where she remained stroke free and had one minor episode of gastrointestinal hemorrhage.
Systemic sclerosis is a rare autoimmune connective tissue disease with varying severity. The condition falls into two major categories; diffuse or localized scleroderma. The localized version is known as CREST Syndrome and has a fourfold higher prevalence among women compared to male counterparts [6]. Bleeding telangiectasias can cause severe gastrointestinal bleeding which have high mortality rate, up to 22% in some series. Women were 2.7 times more likely to have gastrointestinal bleeding due to telangiectasias [7]. Iron deficiency anemia due to severe acute upper gastrointestinal bleeding is common. Hence, Proper endoscopic evaluation is needed in patients with CREST syndrome who present with microcytic anemia. Recurrent bleeding from mucosal telangiectasia is possible [8].
Atrial fibrillation is widely encountered in medical practice. Its most feared consequence is stroke resulting in permanent neurologic sequelae [3]. The main scoring system used to predict thromboembolic stroke risk in patients with atrial fibrillation is CHA2DS2VASc score, a comprehensive scoring system using clinical variables to identify those at risk [1]. Patients with a CHA2DS2VASc score of 2 or higher require anticoagulation. Bleeding risk with anticoagulation can be estimated using the HAS-BLED bleeding score that incorporates known clinical risk factors that raise bleeding risk [10]. Anti-coagulation raises both the risk of intracranial bleeding and gastrointestinal bleeding [4]. Gastrointestinal bleeding is more common and is not an absolute contraindication to anticoagulation. Risk of recurrence and individual patient factors need to be carefully considered prior to resuming anticoagulation. Those with gastrointestinal telangiectasias are at higher risk for recurrent bleeding [11,12].
In our patient, we considered strategies to occlude the left atrial appendage and therefore reduce the duration of treatment with anticoagulation. The WATCHMAN Device is a minimally invasive procedure that can occlude the left atrial appendage. The device was non-inferior to warfarin as a strategy to lower stroke risk (2.3 events per 100 patient-years with WATCHMAN compared to 3.8 events per 100 patient-years with warfarin (rate ratio, 0.60; 95% credible interval, 0.41-1.05, noninferior margin rate ratio of < 2). The estimated relative risk reduction for stroke was as low as 1.1 in those with high CHA2DS2VASc score. The Watchman device has a high success rate of about 95% in sealing the left atrial appendage and shortens the period of anticoagulation to 45 days [13].
The parachute shaped implantable nitinol device is encased within a trans-septal access sheath and delivery catheter. After successful trans-septal puncture of the atrial septum, introduction of the WATCHMAN access system is followed by isolation of left atrial appendage with a pigtail catheter to allow for safe advancement of the WATCHMAN delivery system and finally deployment of the device.
When performing trans-septal puncture of the atrial septum, there should be careful consideration of patients at risk for pulmonary hypertension such as our patient. Pulmonary hypertension can occur in as many as 35% of patients with CREST syndrome. If untreated, transseptal puncture can lead to right to left shunting patients and cyanosis in such patients. Therefore, patients with CREST affected by pulmonary hypertension who undergo the procedure should be treated with an atrial septal occlude device (Amplatzer) in order to avoid such complications [14].
Conclusion:
WATCHMAN device has proven safety and efficacy and maybe the more appropriate option for stroke prevention in patients with Atrial fibrillation and Crest Syndrome who are at higher risk of bleeding from gastrointestinal telangiectasias.
Teaching points:
Disclosures:
Kamal Shemisa, MD, FACP, FACC: Speakers Bureau: Boehringer Ingelheim, Espiron, and Zoll Cardiac Devices.
Other Authors: Nothing to disclose.
Acknowledgements: None
List of Support/Grant Information: None
Statement of contribution: All authors contributed equally to the manuscript.
Word count: 1500 (Excluding Abstract).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
