
Research Article | DOI: https://doi.org/10.31579/26401045/079
1 Division of Health Sciences and Engineering, Department of Clinical Nursing, Campus Celaya-Salvatierra, University of Guanajuato; Celaya, Guanajuato, Mexico.
2 Division of Health Sciences and Engineering, Campus Celaya-Salvatierra, University of Guanajuato; Celaya, Guanajuato, Mexico.
3 Division of Health Sciences and Engineering, Department of Nursing and Obstetrics, Campus Celaya-Salvatierra, University of Guanajuato; Celaya, Guanajuato, Mexico.
*Corresponding Author: Vicente Beltrán Campos, Division of Health Sciences and Engineering, Campus Celaya-Salvatierra, University of Guanajuato; Celaya, Guanajuato, Mexico.
Citation: Reyna-Echeveste EI, Beltrán-Campos V, Tolentino Ferrel MR, García Campos ML, Jiménez-García SN, et al. (2021) Acylated Ghrelin increases in young adult with obesity due to lack of sleep. J. Endocrinology and Disorders. 5(4): DOI:10.31579/26401045/079
Copyright: © 2021 Vicente Beltrán Campos, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2021 | Accepted: 13 August 2021 | Published: 18 August 2021
Keywords: acylated ghrelin; obesity; young adult; sleep
Interruption or lack of sleep has been linked to chronic degenerative diseases including obesity, which has tripled its figures worldwide in the last 40 years according to data from the world Health organization (WHO). Obesity associated with lack of sleep affects the Circadian rhythm which is responsible for synchronizing the energy balance during the sleep- wake cycle, hormonal secretion, homeostasis of food/energy, among the others. The aim of the study was to determine plasma levels of acylated ghrelin in obese young adults with sleep deprivation to plasma levels of acylated ghrelin in obese Young Adults. Study was carried out a total of 56 young adults with obesity, one of the groups had the condition of lack of sleep, n = 28 per group, to determine the relationship between hours of sleep levels of acylated ghrelin Spearman's correlation test was applied, a negative correlation of Rho = -0.293 and p = 0.028 was found the results obtained suggest that lack of sleep may be a factor that alters hormonal regulation and promotes obesity.
The interruption or lack of sleep (LS) is associated with the increased neuroendocrine activity of the hypothalamus-pituitary-adrenal axis and the sympathetic system [1]. It affects immunological, metabolic responses, synchronicity of the circadian rhythm and neuroendocrine rhythm, promotes factors that trigger cardiovascular diseases, diabetes, hypertension, dyslipidemias, metabolic syndrome, and obesity [2-4].
Obesity has tripled its figures worldwide in the last 40 years according to data from the World Health Organization (WHO) [5], starting at increasingly early ages and is considered the leading cause of death, due to its comorbidities and complications, which are the first cause of consultation at all levels of care and generate high costs in health services [6].
Obesity associated with lack of sleep affects the Circadian rhythm; which is responsible for synchronizing the energy balance during the sleep-wake cycle, hormonal secretion, body temperature regulation, food/ energy homeostasis [7], cell cycle regulation [8], tissue and organic [9], as well how to ensure maximum activity time both individual, behavioral and physiological cells occur at the right time of day, in addition to governing the time and duration of sleep [10].
During phases I and IV of sleep (non-REM, NREM), endocrine activation [11] is generated, determined by the secretion of growth hormone (GH) [12, 13] and secondarily the secretion of ghrelin which it allows to make a positive feedback allowing to raise the GH levels [14], and the energy expenditure; this promotes the release of hormones that regulate food intake and satiety [15]. However, some studies have shown that LS itself allows the elevation of ghrelin levels (Ghr), which increases food consumption and secondarily to the generation of obesity [16]. Ghr is secreted mainly by endocrine cells of the enteric system type X/A [17, 18], is found in the bloodstream in higher concentrations as desoctanoyl or desacyl-ghrelin or deacylated Gh [19-21], and as Ghr acylated or acyl ghrelin, the latter responsible for the biological effects [22, 23]. Ghr levels promotes activation of the orexigenic hypothalamic axis [24], where r- Agouti protein (AgRP) and neuropeptide Y (NPY)[25] are secreted, both related to higher food consumption [23]. In addition, effects on the Central Nervous System (CNS) [26], on the regulation of adipokines and on immune functions [18, 27] are attributed. At the CNS level, a direct action on hypothalamic neurons activating protein kinase (AMPK)[28,29] has been reported, which establishes and inhibition of acetyl-CoA carboxylase [28], increases mitochondrial metabolism and generation of reactive oxygen species; these events induce the expression of orexigenic neuropeptides [30,31] and intervene in the activation of the mTor cytoplasmic nutrient sensor at the hypothalamic level [32], which maintains orexigenic function, which implies a dependence of the detection of nutrient in the pathway signaling of acyl ghrelin[33].
In studies conducted in animal models, the presence of Ghr immunoreactive cells has been demonstrated through immunohistochemical techniques, distributed in different areas of the hypothalamus such as the paraventricular, ventromedial, arcuate, dorsomedial, and lateral hypothalamus nuclei, proposing their participation in the regulation homeostatic, endocrine and autonomic [34,35]. Other studies in laboratory animals, which were administered Ghr in the paraventricular and lateral hypothalamic nuclei, showed that its administration allows these animals to stay awake., reducing the sleep of slow wave so non- REM (NREM) fast wave sleep or REM sleep, accompanied by increased need for food consumption [36,37]. In addition, when subjecting laboratory mice to a lack of sleep of 5 hours, an increase in the content of the hypothalamic Ghr was observed during the first hour of the lack of sleep, as well as; an increase in corticosterone (CORT) [38], and an increased in food consumption that is related to the increase in Ghr [15]. In addition, it has been shown that the secretion of this hormone occurs after the secretion of growth hormone during the NREM phase and before starting the REM phase of physiological sleep [14]. So, blood levels of this hormone exhibit a circadian fluctuation that aligns with meals, with preprandial elevation followed by rapid postprandial reductions [39]. Ghr contributes to the regulation of body weight that could be involved in the modification of somatometric parameters such as body mass index (BMI). On the other hand, in a study conducted by Broussard et.al., where plasma levels of total ghrelin were measured in 19 men with normal BMI, to see their eating behavior, it was shown that lack of sleep raises ghrelin levels compared to men with sleep restriction; finding a correlation of lack of sleep with higher calorie intake [40]. These authors recommend studies that assess the hormonal homeostatic factor.
Chapman et. al., in another study whose objective was demonstrate whether acute sleep deprivation affects food purchase options in a simulated supermarket, where 14 men with normal BMI were subjected to lack of total sleep. They find that there is a positive relationship between lack of sleep and the purchase of a greater number of high- calorie foods compared to purchases made after a normal 8 hour sleep night. In addition, no relationship was found with total Ghr levels [41]. Andarini et. al., in an experimental study, whose objective was to compare acylated ghrelin levels and appetite ranges at different times, in two groups of 16 subjects, one with obesity and normal BMI, it was shown that the levels of acylated ghrelin were higher in participants with normal BMI compared to the obesity group. There are no differences in appetite ranges between groups at different measurement times, nor was a correlation found between acylated Ghr levels and appetite ranges [42]. There are still controversies between the different studies on the relationship between lack of sleep, obesity and acylated ghrelin levels, which allows us to determine if the variations of this hormone have a direct influence on food consumption. This article aims to identify the relationship between lack of sleep and acylated ghrelin levels in young Adults with obesity.
Study was conducted with 56 young adults with obesity from the city of Celaya, Guanajuato, Mexico; divided into 2 groups. Control group with 28 young people with obesity without lack of sleep; group cases with 28 young people with obesity and lack of sleep. For the exclusion criteria, the diagnosis of chronic degenerative diseases such as hypertension, diabetes, sleep disorders, Prader Willis syndrome, who were under medical treatment to fall asleep, as well as the use of psychoactive substances.
The information of sociodemographic data was obtained through the self-application of data card; prior authorization and signed informed consent.
The weight and height measurement were performed for the calculation of the body mass index, subsequently the blood was collected in a tube with EDTA and Pierce 88265 protease inhibitor by venous puncture. The blood was centrifuged at 3500 rpm at 4° C, the plasma was separated for storage at -20° C until the level of acylated ghrelin levels was determined, using the ELISA technique.
Determination of Acylated Ghrelin Levels
For the determination of plasma acylated ghrelin hormone levels, using the ELISA technique, the Acylated ghrelin (human) express enzyme immunoassay kit# A05106.96 wells kit, Bertin pharma Brand, was used according to the manufacturer´s specifications.
Data analysis
The analysis of the results was carried out through the statistical package SPSS 24.
Descriptive statistics were applied for sociodemographic variables; for the numerical ones, central tendency measures were applied and for the categorical ones, frequencies (f) and percentages (%) were determined. For the analysis of the differences of means between the groups in the values of weight, height and BMI, the Student t test was applied for independent samples. After the analysis with the Levene test, the Mann Whitney U test was applied to obtain the mean difference; as well as Spearman´s correlation coefficient to determine the relationship between lack of sleep and elevated ghrelin levels, with an error value of 0.05.
Ethical and legal considerations
All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki.
The research project was approved by the Research Committee and the Bioethics Committee of the Celaya-Salvatierra Campus of the University of Guanajuato, with registration numbers CIDSC-3532910 and CBCCS-01626112018 respectively.
Sociodemographic data
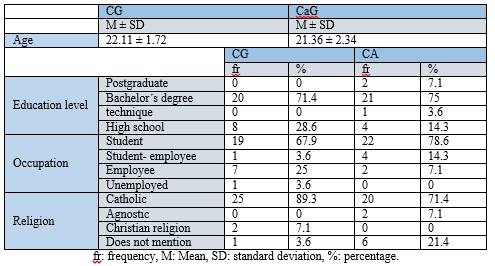
The sociodemographic data collected through a questionnaire, applied to a total of 56 participants(n=56), distributed in 2 groups, control group (CG) and case group (CaG) with a total of 28 participants each, showed that the average age of the participants in the GC is 22.11± 1.72 years and for the CaG 21.36± 2.34, a predominant degree level of studies was found with 3.6% of the GC and 14.3% of the CAG study and work, the most common religion was the catholic with 89.3% in the GC and 71.4 in the CaG (Table 1).
Anthropometric data
The analysis of the results obtained by Student´s t test for weight measurements, showed that there is no statically significant difference with a t(1,54) = -0.783; for measurement of body height t(1,54) = 0.192, and for BMI t(1.54) = -0.695 when comparing the CG against the CaG (Table 2).

Hours of sleep and levels of acylated ghrelin
For the analysis of the values obtained from the total hours of sleep and levels of acylated ghrelin, the Mann Whitney U test was applied, where it was shown that there are statistically significant differences with respect to the total hours of sleep when comparing both groups with a U= 0.0001, mid-range for the CG= 42,500 and for the CaG= 14,500.
With respect to the results obtained from ghrelin levels, it showed that there are statistically significant differences when comparing both groups with a U= 234, p= 0.0096, and mid-range for the CG=22.857 and for the CaG= 34.143 (Table 3).

Association between sleep hours and Acylated ghrelin plasma levels
To determine the relationship between sleep hours and acylated ghrelin levels, the Spearman correlation test was applied, showing a negative correlation Rho= -0.293 and p= 0.028, indicating a moderate correlation, implying that at a lower correlation hour of sleep there are higher levels of acylated ghrelin.
The results obtained in this research we can propose the existence of an inverse relationship between lack of sleep and plasma levels of acylated ghrelin in young people with obesity, which implies that shorth-term sleep or lack of sleep may be a factor that alters hormonal regulation and is associated with a greater probability of promoting obesity and increased adiposity [43, 44].
This lack of sleep permeates a dysregulation of the neuroendocrine system, allows the elevation of orexigenic hormones such as ghrelin; that, together with ghrelin, leptin and dopamine; they are involved in the increase in the need for energy consumption and the maintenance of food reward systems, so they are perceived as appetite regulators [42, 45, 46]. As ghrelin is one of the main hormones related to preference of high palatability and high calorie food regardless of metabolic requirements [47, 48]; high concentrations of this could be a cause in the increase and /or difficulty for weight loss [49]. Therefore, its regulation should be proposed in the diagnosis and comprehensive treatment plans of the patient with obesity.
Important coincidence of the results of this study with those obtained by DelParigi et al., where it reports an increase in ghrelin hormone in patients with Prader Willi syndrome, points to ghrelin as the main factor of hyperphagia [50]. In addition, Kweh et al., propose that the increase in ghrelin during childhood is a predictor of obesity [51].
Another study conducted through functional magnetic resonance imaging in obese and non- obese subjects, showed that the activation of various brain areas such as the ventral striatum, the ventromedial prefrontal cortex, and the extra striated visual cortex, related to reward phenomenon. On the other hand, greater activations related to reward in the dorsolateral prefrontal cortex and posterior precuneus cluster of obese subjects were observed; compared to non-obese [52]. Consistent with this, obese subjects exhibited longer election times after repeated rewards and circulating ghrelin levels lower than lean controls. Reduced ghrelin levels significantly predicted slower post- rewards and circulating ghrelin levels lower than lean controls. Reduced ghrelin levels significantly predicted slower post- reward choices and reward- related hyperactivity in the dorsolateral prefrontal cortices in obese subjects [52].
Perhaps ghrelin signaling on the posterior hippocampus- hypothalamus- brain pathway is affects, by counteracting satiety signals at the intestinal level, allowing the increase in the amount of food ingested. Ghrelin and orexin interact to increase the need for energy consumption through a downward signaling pathway from the hippocampus to the hindbrain [53]. On the other hand, Andarini et, al., relate the subtype of acylated ghrelin with the qualification of self- reported appetite in obese subjects with normal body index, when determining acylated ghrelin before food consumption and 30, 60 and 120 minutes after food consumption showed that acylated ghrelin levels remained increased in obese subjects compared to the control group [42]. Thus, ours results of the correlation between obesity and plasma ghrelin levels support the results of this study.
Contrary to the data shown by Quian et. al., point out that circadian misalignment increases appetite for calorie- rich foods, in addition to raising postprandial levels of acylated ghrelin [54]. Likewise, Aly et. al., reported that ghrelin levels are lower in children with obesity [55]. Another study in laboratory animals showed that increase in ghrelin does not favor the reward system and orexigenic effects, proposed a mechanism that favors resistance to ghrelin, whose function is to prevent starvation and not promote obesity [56]. So, so far, the data referring to this relationship remain controversial.
The present study yielded results that allow us to support the obesity approach from the neuroendocrine point of view and the factors involved in it through new mechanisms. Because lack of sleep is a new health problem that leads to appearance of chronic diseases, it is a suggested to intervene early in the diagnosis and treatment of sleep disorders and obesity.
It is recommended to carry out new studies that support this relationship, which will determine a causal relationship (Randomized Controlled Studies, RTC) and double blind, to achieve control of the intervening variables; it is also suggested to contrast the studies found with subjects of normal weight, to enrich the results found in this research.
The authors REEI and BCV, worked equally in the experimental development and in the writing of the article, these authors have contributed equally to this work and share first authorship. The author TFMR participated in the data collection, CGML and JGSN participated in the review of the article and the experimental design, RGXS and BFE in the search for references, all authors reviewed the final version of the article.
The University of Guanajuato supports the financing of laboratory reagents and the publication of this article.
The authors thanks Francisco Corona Palmerin and Miriam Cervantes Tolentino, students of the Degree in Nutrition, María Guadalupe Botello Jacuinde student of the Master´s degree in Nursing Sciences of the University of Guanajuato Campus Celaya- Salvatierra.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
