
Case Report | DOI: https://doi.org/10.31579/2692-973X/056
1 Brain Mapping and EEG Laboratory UFRJ - IPUB and Professor UNIG, Brazil.
2 Department of Neurology – UNIFESP, Brazil.
3 Universidade Iguaçu – UNIG, Brazil.
4 Universidade Estácio de Sá - Medicine, Brazil.
5 Universidade do Rio de Janeiro - UERJ, Brazil.
6 Neurology Service - UFRJ, Brazil.
7 Medicine School - UFRJ, Brazil.
8 Neurosurgery- UFF, Brazil.
9 Radiology Institute Lara Brandão, Brazil.
*Corresponding Author: Marco Orsini, Brain Mapping and EEG Laboratory UFRJ - IPUB and Professor UNIG, Brazil.
Citation: Marco Orsini., Acary B. Oliveira., Jaqueline F.do Nascimento., Clara de A e Araújo Leite, Eduardo Jorge, et al., (2023), Acute traumatic encephalopathy in an MMA athlete: EEG findings Presentation of a case, J. Brain and Neurological Disorders. 6(3): DOI:10.31579/2692-973X/056
Copyright: © 2023, Marco Orsini. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 April 2023 | Accepted: 27 April 2023 | Published: 04 May 2023
Keywords: MMA; athletes; JMA; EEG; notorious, acute traumatic encephalopathy; chronic traumatic encephalopathy
Acute traumatic injuries in MMA (Multiple Martial Arts) athletes are frequent. The trauma mechanisms are caused by punches, elbows and kicks. In the acute phase, loss of consciousness, dizziness, headache, and other complaints are frequent. We present the case of an MMA athlete who, after being knocked out, lost consciousness and persisted for weeks with extreme irritability, headache, insomnia, slowed thinking, and incapacitating vertigo.
JMA, 26 years old, male, professional MMA fighter, reports that about 1 month ago (moments after trauma by knockout) he presented with loss of consciousness for a few seconds, visuospatial dysfunction, pounding headache, and five episodes of vomiting. He was evaluated by a doctor at the event and referred to hospital for complementary exams. Laboratory: Normal. Skull CT: No changes. EEG with Brain Mapping: discrete signs of cortical and subcortical dysfunction of nonspecific character with slowing of the dominant posterior rhythm and diffuse increase of the slow theta activity. About 15 days post-trauma he still presents headache, behavioral changes (emotional lability) and insomnia.
JMA, 26 years old, male, professional MMA fighter, reports that about 1 month ago (moments after trauma by knockout) he presented with loss of consciousness for a few seconds, visuospatial dysfunction, pounding headache, and five episodes of vomiting. He was evaluated by a doctor at the event and referred to hospital for complementary exams. Laboratory: Normal. Skull CT: No changes. EEG with Brain Mapping: discrete signs of cortical and subcortical dysfunction of nonspecific character with slowing of the dominant posterior rhythm and diffuse increase of the slow theta activity (figure 1-2). About 15 days post-trauma he still presents headache, behavioral changes (emotional lability) and insomnia. During the neurological examination, the reaction time between the tasks requested by the examiner and the conclusion, such as dyscalculia, dysnomia, and even slowness in answering questions related to daily life, drew attention. A "gap" of time between questions and answers is notorious. Medications used: betaistine 24mg 3x a day; dipyrone 500mg every 12 hours, quetiapine 25mg 2x a day; zolpidem 12.5mg at bedtime. Guided not to return to activities involving MMA until full recovery. Alerted to the risks of Chronic Traumatic Encephalopathy.
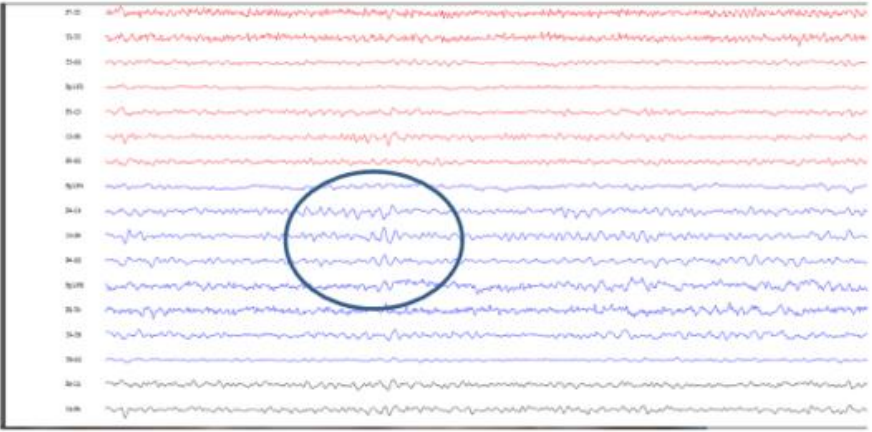
Figure 1: Ondas teta em F4-C4 e em C4-P4
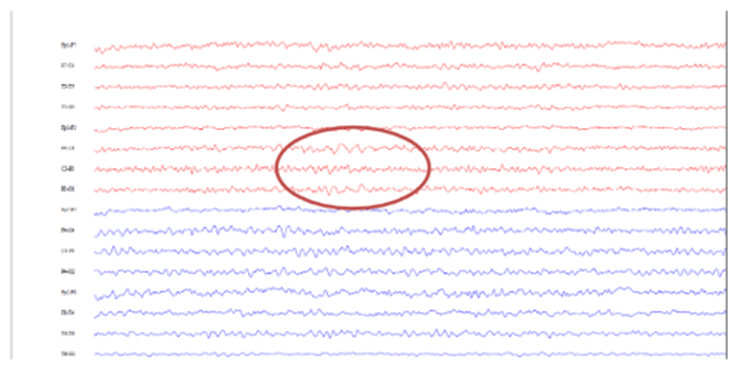
Figure 2: Ondas teta em C3-P3 e em F3-C3
In the detection of acute cerebral concussions, EEG may be more sensitive than neurological examination. After mild traumatic injuries, most patients with abnormal neurological examination have abnormal EEG findings (more than 80% of cases) - as in the present case.
In contrast, only 23% of abnormal EEGs were accompanied by an abnormal neurological examination. EEG changes are not uniform in all patients, probably because of differences in severity and type of trauma [1-2]. To date, EEG is considered the first clinical "neurodiagnostic" assessment that reveals abnormal brain function after traumatic brain injury. Although it has been described since the 1940s in patients the post-traumatic brain injury test is still an excellent tool for identifying the first "electrical" damage to the central nervous system [5].
One of the most common chronic problems that occur as a result of boxing is the chronic progressive encephalopathy of boxers or MMA fighters, which is also called dementia pugilistic or punch drunk syndrome. This syndrome, however, does not only affect boxers; several other sports can trigger it, such as American soccer, soccer, and rugby. Boxer dementia causes problems with attention, memory and concentration, parkinsonian symptoms, disorientation and headaches. As the disease progresses, you notice increased irritability, aggressiveness, mental confusion, poor coordination of speech muscles, and progressive dementia [6].
The patient in the present study presented some of these clinical manifestations after the acute presentation. There is a high probability that athletes who suffer cranial impacts several times and with disproportionate force will develop Chronic Traumatic Encephalopathy [7].
In view of the above, we elucidate the importance of this post-trauma test, as well as orient the patient of the present case and other MMA athletes about the risks of CTE and its consequences, such as behavioral and dementia symptoms.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
