
Research Article | DOI: https://doi.org/10.31579/2694-0248/073
Advisor doctor and expert trainer, The National Center of Training and Development and Baghdad Medical City, Baghdad, Iraq.
*Corresponding Author: : Aamir Al-Mosawi, Advisor doctor and expert trainer, The National Center of Training and Development and Baghdad Medical City, Baghdad, Iraq.
Citation: Aamir Al-Mosawi, (2023), Acute Rheumatic Fever: The Rare Association with Vitamin B12 Deficiency Induced Neutropenia, J Clinical Orthopaedics and Trauma Care, 5(5); DOI: 10.31579/2694-0248/073
Copyright: © 2023, Aamir Al-Mosawi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 November 2023 | Accepted: 20 November 2023 | Published: 30 November 2023
Keywords: acute rheumatic fever; vitamin B12 deficiency; induced neutropenia; acute febrile illness
Background: Acute rheumatic fever is an autoimmune disorder that develops commonly few weeks following a group A beta hemolytic Streptococcal tonsillopharyngitis. The autoimmune response can affect joints, skin, heart, and the brain. One of the important serious consequences of acute rheumatic fever that have to be prevented is the the long-term heart disease resulting from valves damage which may occur after one severe illness or following multiple recurrence of the illness. The diagnosis of acute rheumatic fever is generally based on the presence of either two Major diagnostic criteria (multiple joint arthritis, carditis, erythema marginatum, chorea, and subcutaneous nodules) or one Major diagnostic criteria and two Minor criteria (Fever, arthralgia, first degree heart block, elevated inflammatory markers [ESR and C-reactive protein]) plus appropriate evidence of preceding streptococcal infection.
The association of acute rheumatic fever with vitamin B12 deficiency-induced neutropenia has not been reported previously in the medical literature.
Patients and methods:The case of a ten-year old girl who developed acute febrile illness associated with arthralgia, arthritis, skin rash and neutropenia is described.
Results: The patient developed fever and arthritis of one elbow (Painful and swollen) followed shortly by the development of macular rash consisting of pink rings mostly on the extensor surfaces and arthritis of the second elbow. The patient had a previous febrile illness associated with sore throat which occurred during the previous 2 to 3 weeks. ASO titer was 150 iu/ml and CRP was positive 300 mg/dL. The patient had a high ESR, leukopenia, and blood film showed severe neutropenia, poikilocytosis and, frequent eliptocytosis. Serum vitamin B12 level was low, 152 pg/mL. Echocardiography showed low mitral valve prolapse.
Conclusion: The novel association of acute rheumatic fever with vitamin B12 deficiency-induced neutropenia is reported.
Acute rheumatic fever is an autoimmune disorder that develops commonly few weeks following a group A beta hemolytic Streptococcal tonsillopharyngitis. The autoimmune response can affect joints, skin, heart, and the brain. One of the important serious consequences of acute rheumatic fever that have to be prevented is the the long-term heart disease resulting from valves damage which may occur after one severe illness or following multiple recurrence of the illness.
Some of the important features of acute rheumatic fever have been known as early as the 1700s.
In 1797, Matthew Baillie quoted David Pitcairn (Figure-1A) who suggested that rheumatism is one of the causes of a morbid growth of the heart.
Matthew Baillie (Figure-1B) reported the presence of a thickening of some valves of heart in autopsies of patients who had acute rheumatism [1].
Figure (1A): David Pitcairn (1749-1809), a Scottish physician; (1B): Matthew Baillie (1761-1823), a British physician and pathologist
In 1803, Wagstaffe of Southwark reported a fatal case of rheumatic pericarditis with enlargement of the heart [2], and Crowfoot of Beccles reported two cases of rheumatic carditis in 1809 [3].
In 1809, David Dundas reported nine cases of heart disease associated with rheumatism that had been observed since 1770. The cases reported by Dundas were considered typical cases of acute rheumatic carditis. The heart disease started after, or sometimes during the same time of rheumatism. The cases of Dundas were mostly young patients who developed chest pain cough, dyspnea, and palpitations. There was a high death rate with most patients died because of congestive cardiac failure [4].
In 1812, William Charles Wells was still thinking that the association of rheumatism with heart disease was a concurrence rather than a specific association as he quoted Morgagni and Ferriar who had regarded the association as apparently an interesting coincidence [5, 6].
Richard Bright (Figure-1C) was probably the first to recognize the association of neurological manifestations of rheumatic fever (Sydenham’s chorea) with joint manifestations (Rheumatism) in 1831 [7].
Walter Butler Cheadle (Figure-1D) was most probably the first to link rheumatism and heart disease with tonsillitis in 1889. He reported his observations during twenty years on rheumatic fever at the Hospital for Sick Children, Great Ormond Street [8].

Figure (1C): Richard Bright (1789-1858), an English physician; (1D): Walter Butler Cheadle (October 1836-March 1910), an English pediatrician.
Freeric John Poynton (Figure-1E) and his colleague Paine were most probably the first to identify the diplococcus which they isolated from patients with acute rheumatic fever as the causative bacteria for the disease [9]. In 1944, Thomas Duckett Jones (Figure-1F) suggested diagnostic criteria for its diagnosis [10].
Figure (1E): Frederic John Poynton (June 26, 1869-October, 29 1943), an English physician; (1F): Thomas Duckett Jones (February 2, 1899-November 22, 1954) was an American physician, cardiologist.
Jones diagnostic criteria have been revised and modified in 1965, 1984, 1992, and 2002. The diagnosis of acute rheumatic fever is generally based on the presence of either two Major criteria (multiple joint arthritis, carditis, erythema marginatum, chorea, and subcutaneous nodules) or one Major criteria and two Minor criteria (Fever, arthralgia, first degree heart block, elevated inflammatory markers [ESR and C-reactive protein]) plus appropriate evidence of preceding streptococcal infection [11-14].
The association of acute rheumatic fever with vitamin B12 deficiency-induced neutropenia has not been reported previously in the medical literature.
The case of a ten-year old girl who developed acute febrile illness associated with arthralgia, arthritis, skin rash and neutropenia is described.
The patient developed fever and arthritis of one elbow (Painful and swollen) on the 22nd of August, 2023 followed shortly by the development of macular rash consisting of pink rings mostly on the extensor surfaces and arthritis of the second elbow. The face was not involved by the rash. She was treated with oral antibiotics and analgesics without obvious improvement. The patient was brought to us on the 26th of August, and she still had painful swollen elbows and rash (Figure-2). The patient had a previous febrile illness associated with sore throat which occurred during the previous 2 to 3 weeks.

Figure (2A): Macular rash consisting of pink rings mostly on the extensor surfaces.

Figure (2B): Macular rash consisting of pink rings mostly on the extensor surfaces.

Figure (2C): Macular rash consisting of pink rings mostly on the extensor surfaces.
ASO titer was 150 iu/ml and CRP was positive 300 mg/dL.
Erythrocyte Sedimentation Rate (ESR) was 100 cubic mm/hour.
Hemoglobin was 8.9 g/dL.
White blood cell count was 1.58 × 109/L (Normal: 4.0 to 11.0 × 109/L).
Granulocyte (Including neutrophils) count was 0.9 × 109/L (Normal: 2.0 to 7.0 × 109/L).
Blood film showed:
White blood cells: Severe neutropenia, no immature or abnormal cells.
Red blood cells: Poikilocytosis (10% or more of blood cells have abnormal shape), frequent eliptocytosis, occasional polychromasia (Excessive immature blood cells).
Platelets: Normal.
Serum folic acid was within normal range.
Serum vitamin B12 level was 152 pg/mL (Normal: 200-900 pg/mL).
Radiographs of the left elbow showed no significant abnormalities (Figure-3).
Ultrasound of the elbows showed fluid collection suggesting joint effusion (Figure-4).
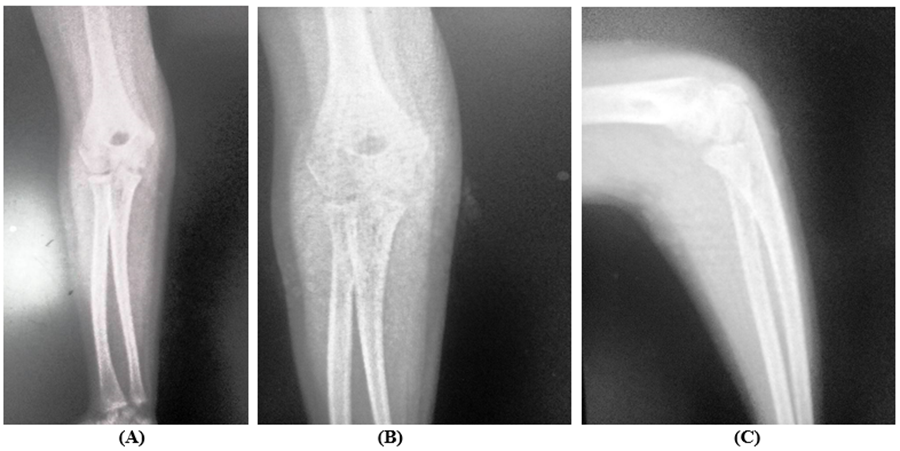
Figure 3 (A): Radiographs of the left elbow; (B): Radiographs of the left elbow; (C): Radiographs of the left elbow.

Figure 4: Ultrasound of the elbows showed fluid collection suggesting joint effusion.
Erythrocyte Sedimentation Rate (ESR) was 19 cubic mm/hour.
Hemoglobin was 10.1 g/dL.
White blood cell count was 2.7 × 109/L (Normal: 4.0 to 11.0 × 109/L).
Granulocyte (Including neutrophils) was 29.6 %.
Serum vitamin B12 level was 210 pg/mL (Normal: 200-900 pg/mL).
Zeynep Canan Ozdemir from Turkey and her research group reported the etiological causes of neutropenia in 94 children. 55 children (58.5%) had post-infectious neutropenia with 38.4% occurring following upper respiratory airway. 23 (24.6%) children had idiopathic neutropenia. Six children (6.3%) had drug-induced neutropenia. Five children (5.3%) had vitamin B12 deficiency-induced. Two children (2%) had chronic benign neutropenia. One child (1.1%) had immune deficiency, one child (1.1%) had autoimmune lymphoproliferative syndrome, and one child (1.1%) had post-infection hemophagocytic lymphohistiocytosis.
Neutropenia improved in ninety-one children (96.8%).
Neutropenia persisted in 3 children (3.2%).
One died because of infection [24].
Although, the patient in this report had lab-confirmed vitamin B12 deficiency, the blood film showed no macrocytosis, but showed poikilocytosis and frequent eliptocytosis.
As early as 1982, Spivak emphasized that megaloblastic anemia can be masked by the absence of macrocytosis. Spivak also emphasized that poikilocytosis may indicates a vitamin deficiency [25].
As early as 1982, Schoomaker and colleagues, emphasized that vitamin B deficiency may result in an abnormal red blood cells’ membrane causing elliptocytosis [26].
In this patient, echocardiography showed low mitral valve prolapse.
As early as 1980, Storozhakov et al suggested the potential of echocardiographic diagnosis of rheumatic valvulitis and mitral valve prolapse in children [27].
In 1988, Lembo et al emphasized that acute rheumatic fever commonly results in mitral regurgitation without associated mitral valve stenosis. They reported that the surgical findings have showed a high frequency of mitral prolapse in rheumatic valvular heart disease suggesting that acute rheumatic fever can cause mitral valve prolapse.
Lembo et al reported thirty patients who had previously acute rheumatic fever. 25 patients (84%) were found to have mitral regurgitation on doppler examination. Echocardiography showed mitral prolapse in 24 patients (80%). Only one patient had mitral stenosis when examined by echocardiography.
Therefore, Lembo et al suggested that acute rheumatic fever can cause mitral valve prolapse [28].
The use of ibuprofen in acute rheumatic fever was reported as early as the 1970s [15].
In 2021, Derya Altay from Turkey and her research team reported 286 patients with acute rheumatic fever. 53 patients (18.5%) [Mean age: 10.7 ± 2.5 years] were treated initially with aspirin for arthritis.
Aspirin-associated hepatotoxicity occurred in 9 (17%) of the 53 patients, and therefore ibuprofen or naproxen was given as an alternative to aspirin. Both ibuprofen and naproxen were not associated with side effects.
30% of 53 patients had anemia, and aspirin was used for longer period in the hepatotoxic anemic patients than non-anemic patients (p=0.02) [16].
Münevver Yılmaz and her colleagues emphasized that the use of Aspirin (Acetylsalicylic acid) in acute rheumatic fever can be associated with severe side effects [17].
The use of single injections of benzathine penicillin given every month in the treatment of acute rheumatic fever was reported as early as the 1950s [18-21].
In 2013, Nigel Wilson from New Zealand reviewed the literature and emphasized that randomized controlled studied showed four weekly intramuscular long-acting benzathine penicillin G was found to be more effective than penicillin given orally to prevent recurrence of rheumatic fever [22].
In 2022, Anna P Ralph and Bart J Currie from Australia emphasized that the aims of the treatment of acute rheumatic fever include relieving symptoms, lessening heart valve damage and eliminating streptococcal infection. They recommended the use of monthly intramuscular injections benzathine benzyl penicillin G for the prevention of recurrences [23].
The novel association of acute rheumatic fever with vitamin B12 deficiency-induced neutropenia is reported.
The author has the copy right of all figures and sketches included in this paper.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
