
Research Article | DOI: https://doi.org/10.31579/2690-1919/433
1MRCS, Nuffield Orthopaedic Centre, Oxford, Oxford, UK
2Medical Student, University of Oxford, Oxford, UK
3FRCS, Nuffield Orthopaedic Centre, Oxford, Oxford, UK
4. FRCS, Nuffield Orthopaedic Centre, Oxford, Oxford, UK
5. FRCS, Nuffield Orthopaedic Centre, Oxford, Oxford, UK
*Corresponding Author: Joe Dixon. MRCS, Nuffield Orthopaedic Centre, Oxford, Oxford, UK.
Citation: Joe Dixon, Thirushan Wignakumar, Benjamin Kendrick, Abtin Alvand, Antony Palmer, (2024), Acute Kidney Injury Following Primary Knee Replacement; Systematic Review, J Clinical Research and Reports, 17(2); DOI:10.31579/2690-1919/433
Copyright: © 2024, Joe Dixon. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 06 November 2024 | Accepted: 23 November 2024 | Published: 28 November 2024
Keywords: acute kidney injury; knee; arthroplasty
Objectives
Knee Replacement (KR) is a highly-effective procedure for improving pain and function in patients. Acute Kidney Injury (AKI) is a potential complication that is associated with increased length of stay, morbidity and mortality. The aims of this systematic review were to establish the incidence of AKI following primary KR and to characterize risk factors for AKI and the incidence of Renal Replacement Therapy (RRT).
Methods
A systematic review of the literature was undertaken with a search of Medline, Embase, Scopus, Cochrane Library. The review included clinical trials or observational studies (cohort, case-control or cross-sectional studies) reporting the incidence of AKI following primary KR.
Results
1,523 studies were identified in the initial search, with eight meeting the inclusion criteria. A total of 13,574 episodes of patients undergoing primary knee replacement were included. The mean age of patients was 68.91 years (SD 2.68). 11,346 (83.02%) of patients were female. The weighted pooled incidence of AKI in the included studies was 8.85 (95% CI 8.35% to 9.35%). Risk factors highlighted for AKI following primary KR frequently identified were Age >65, Diabetes Mellitus and pre-existing chronic kidney disease. There was limited data on the requirement for RRT.
Conclusion
AKI is one of the most common complications following KR. There is a need for research into interventions that may reduce the risk of AKI.
Knee Replacement (KR) is a highly-effective procedure for improving pain and function in patients [1]. Approximately 80,000 knee replacements are undertaken in the United Kingdom each year with this number anticipated to increase [2-4]. Primary KR has demonstrated excellent long-term implant survival and patient-reported outcome scores however minimising post-operative complications continue to remain a priority [1,2]. Acute kidney injury (AKI) is one such complication that can have implications for, length of stay, patient morbidity and mortality [5-9].
AKI is a complex clinical condition, characterized by a sudden deterioration in kidney function, characterised by increased serum creatinine levels and/or reduced urine output [10-13]. The cause of AKI is commonly multifactorial in origin, with factors including hypovolemia, nephrotoxic medications and systemic inflammation [14,15]. Globally, AKI is a very common condition affecting over 13 million patients per year [5,7,14]. There is increasing evidence that even a transient AKI can cause subsequent increases in short and long-term mortality, as well as increased hospital costs and length of stay following surgery [6,16,17].
There are three commonly used classification systems for the diagnosis of AKI [10,12,18]. The first proposed was the Risk, Injury, Failure, Loss and End-stage disease (RIFLE) classification [11]. Subsequently, the Kidney Disease Improving Global Outcomes (KDIGO) [18] and the Acute Kidney Injury Network (AKIN) [12] have been developed. The individual diagnostic and staging criteria of each classification system can in found in Table 1.
| Criteria | RIFLE (11) | AKIN (13) | KDIGO (17) |
| Stages | Risk, Injury, Failure, Loss, End-stage kidney disease | Stages 1, 2, 3 | Stages 1, 2, 3 |
| Time period | Within 7 days | Within 48 hours | Within 7 days |
| Stage 1 | Risk (≥ 1.5 times baseline or Glomerular Filtration Rate (GFR) decrease ≥ 25%), | Creatinine increase≥ 0.3 mg/dL or GFR decrease ≥ 25% or urine output < 0> | Serum creatinine≥ 0.3 mg/dL increase or GFR decrease ≥ 25% or urine output < 0> 6-12 hours), |
| Stage 2 | Injury (≥ 2 times baseline or GFR decrease ≥ 50%), | GFR decrease ≥ 50% or urine output < 0> | GFR decrease ≥ 50% or urine output < 0> |
| Stage 3 | Failure ≥ 3 times baseline or GFR decrease ≥ 75% or serum creatinine ≥ 4 mg/dL with an acute rise ≥ 0.5 mg/dL | GFR decrease ≥ 75% or GFR < 3> | GFR decrease ≥ 75% or GFR < 35> |
| Stage 4 | Loss (complete loss of kidney function > 4 weeks), | ||
| Stage 5 | End-stage kidney disease (complete loss of kidney function > 3 months) |
Table 1: Summary of commonly used classification systems for AKI
The KDIGO classification is the most widely used by peri-operative clinicians [18].
The reported incidence of AKI following primary KR varies greatly and many of the studies combine data from knee and hip replacements to provide incidence estimates [19-23]. The incidence of AKI following hip or knee joint replacement surgery reported in the literature range from 0.05% to 21.9% [5,6,20,24,25]. The cause for the variability of incidence reported in the literature is not known. (Table 1).
Appendix 1: Search Strategy and Results
Medline
Database:
Medline (Ovid MEDLINE® Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE® Daily and Ovid MEDLINE®) 1946 to present
| # | Query | Results from 9 Mar 2023 |
| 1 | exp Acute Kidney Injury/ | 55,189 |
| 2 | (acute kidney injur* or acute kidney insufficienc* or acute kidney failure* or acute renal injur* or acute renal insufficienc* or acute renal failure*).ti,ab,kw. | 62,995 |
| 3 | 1 or 2 | 81,697 |
| 4 | arthroplasty, replacement, knee/ | 30,850 |
| 5 | (knee arthroplast* or knee replacement* or knee prosthe*).ti,ab,kw. | 40,398 |
| 6 | (joint arthroplast* or joint replacement* or joint prosthe*).ti,ab,kw. | 16,746 |
| 7 | 4 or 5 or 6 | 56,665 |
| 8 | 3 and 7 | 205 |
exp Acute Kidney Injury/
(acute kidney injur* or acute kidney insufficienc* or acute kidney failure* or acute renal injur* or acute renal insufficienc* or acute renal failure*).ti,ab,kw.
1 or 2 arthroplasty, replacement, knee/
(knee arthroplast* or knee replacement* or knee prosthe*).ti,ab,kw.
(joint arthroplast* or joint replacement* or joint prosthe*).ti,ab,kw.
4 or 5 or 6
3 and 7
Scopus Searched:31/3/2023
| # | Query | |
| Knee AND replacement | ||
| OR | Knee AND arthroplasty | |
| And | Acute AND renal AND injury | |
| OR | Acute AND renal AND failure | |
| OR | Acute AND kidney AND injury |
Total results 882
Embase
Database:
Embase 1974 to present
| # | Query | Results from 9 Mar 2023 |
| 1 | total knee replacement/ or knee replacement/ or knee arthroplasty/ | 53,138 |
| 2 | acute kidney injury.mp. and acute kidney failure/ | 51,811 |
| 3 | acute kidney failure.mp. or acute kidney failure/ | 117,896 |
| 4 | acute renal failure.mp. or acute kidney failure/ | 125,956 |
| 5 | 2 or 3 or 4 | 126,258 |
| 6 | 1 and 5 | 382 |
total knee replacement/ or knee replacement/ or knee arthroplasty/ acute kidney injury.mp. and acute kidney failure/ acute kidney failure.mp. or acute kidney failure/ acute renal failure.mp. or acute kidney failure/
2 or 3 or 4
1 and 5
Cochrane Clinical reviews Searched on 9/3/2023
Results: 53 (acute kidney injury):ti,ab,kw OR (Acute renal injury):ti,ab,kw AND (Knee arthroplasty):ti,ab,kw OR ("total knee replacement"):ti,ab,kw OR ("knee
The search was performed on 31/3/2023. Duplicates were removed using Rayyan.AI software deduplication function, any excluded duplicates were re-checked manually to prevent any articles from being excluded by error. References of included articles were assessed to identify if any potential studies for inclusion had been missed by the search.
Eligibility criteria
Clinical Trials and observational studies (cohort, case-control or cross-sectional studies) reporting the incidence of AKI following primary KR were included. Studies must have documented the classification criteria used for AKI diagnosis. No time or geographical restrictions were placed on the inclusion criteria. The exclusion criteria were as follows; if the study provided only pooled data on hip and knee replacements or did not provide the required demographic or outcome data, and studies published in languages other than English.
| Inclusion Criteria |
| 1.Studies reporting the incidence of AKI following primary KR |
| 2.Clinical Trials and Observational Studies (Cohort, Case-Control, Cross-sectional) |
| 3.All indications for primary KR |
| 4. Clear classification criteria used for diagnosis of AKI (KDIGO, AKIN, RIFLE) |
| Exclusion Criteria |
| 1.Studies providing pooled data for hip and knee replacement |
| 2.Review articles, case series and reports |
| 3. Studies published in languages other than English |
Table 2: Summary of Inclusion and Exclusion criteria
Data Extraction:
Screening was performed by two authors (JD, TW). This initially consisted of title and abstract screening using the Rayyan.AI software, followed by a full-text review of potential studies to ensure they met the selection criteria. Included studies were extracted for the following data: last name of the first author, year of publication, journal, study design, total number of patients, demographic data (age and sex), criteria used for diagnosis of AKI, length of follow-up, inclusion/exclusion criteria for the study, the incidence of AKI, risk factors for AKI, RRT and subgroup data from each study. Data was inputted into a Microsoft Excel spreadsheet. The duration of the peri-operative period for which AKI diagnosis was recorded was documented for each study. This was to ensure we had comparable data between studies to enable data synthesis. For studies reporting patients who required RRT, we recorded the diagnostic criteria and time from surgery that this diagnosis was made.
All studies reporting the rate of AKI following KR were included for data synthesis. All criteria used for AKI diagnosis (AKIN, RIFLE, KDIGO) were included in weighted pooled incidence calculations. Subgroup analysis was performed for different diagnostic criteria (AKI; KDIGO, AKIN and RIFLE).
Risk of bias:
Risk of bias was calculated using the Risk of Bias in Non-randomised Studies - of Interventions (ROBINS-I) I criteria [29] and Methodological Index for Non-Randomised Studies (MINORS) criteria [30]. All studies were assessed against the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence criteria (OCEBM) [31].
The search identified 1,523 studies with 487 duplicate records excluded via the Rayyan.AI software, which were then manually checked for accuracy. 1,036 records were screened, and 32 full texts were assessed against inclusion and exclusion criteria
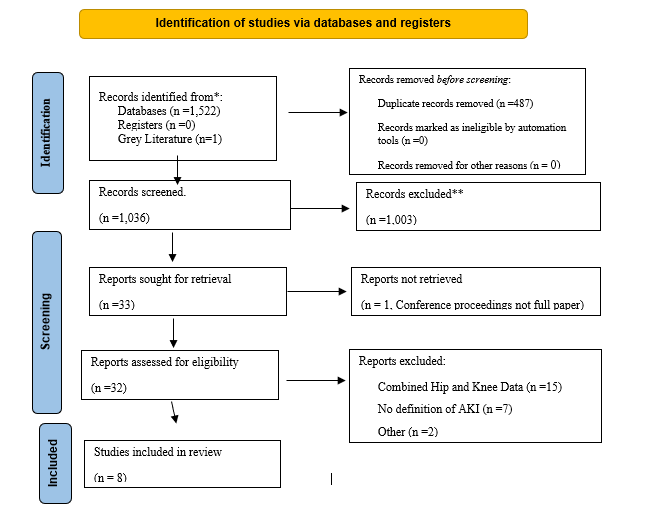
Figure 1: Prisma Search strategy flow diagram
Prisma Search strategy flow diagram
Eight manuscripts met the inclusion criteria
| Author | Year | Country | Study design | Number of patients | OCEBM Rating | Inclusion criteria | AKI diagnosis | AKI incidence Overall % | Renal replacement therapy incidence % | Risk Factors for AKI |
| Klasan et al 38 | 2021 | New Zealand | Retrospective cohort | 631 | 3 | Intraoperative vancomycin and cefazolin in KR patients | KDIGO | 3.9 | Not reported | Chronic Kidney Disease |
| Koh et al 35 | 2018 | South Korea | Retrospective cohort | 1453 | 3 | Bilateral KR patients | KDIGO | 8.1 | Not Reported | Simultaneous and staged (within 7 days) bilateral Knee replacements are high risk for AKI |
| Kim et al 36 | 2016 | South Korea | Retrospective cohort | 1309 | 3 | All patients undergoing KR | KDIGO | 4.4 | Not reported | Age, Diabetes Mellitus, preoperative beta blocker use, high uric acid, intraoperative diuretic use and post operative albumin level < 3.0g/dL |
| Sehgal et al 37 | 2014 | USA | Retrospective cohort | 627 | 3 | All patients undergoing KR | AKIN | 21.9 | Not reported | Age over 65, Diabetes Mellitus and Angiotensin converting Enzyme inhibitor use |
| Halawi et al i33 | 2020 | USA | Retrospective cohort | 319 | 3 | All patients undergoing KR | AKIN | 3.3 | Not reported | Chronic Kidney Disease, or having at least two of the following: age >65 years, BMI> 35, ASA score >3, Diabetes, heart disease, and/or anaemia |
Womble et al 32
| 2019 | USA | Retrospective cohort | 1035 | 3 | All patients undergoing KR | KDIGO | 5.6 | Not Reported | African Americans |
| Kim et al 34 | 2019 | South Korea | Retrospective cohort | 2987 | 3 | All patients undergoing KR | KDIGO | 5.4 | 0.0003 | General anaesthesia increased risk but not statistically significant |
| Ko et al8 | 2022 | South Korea | Retrospective cohort | 5302 | 3 | All patients undergoing KR | KDIGO | 10.20 | 0.004 | Pre-operative serum creatinine levels, Use of tranexamic acid, General anaesthesia, Use of Renin angiotensin antagonists, ASA class and sex |
Table 3: Included Studies in the review
All the studies included were retrospective in design. Four of the studies originated in South Korea, three in USA and one in New Zealand. All the studies reported undertaking primary KR; however, no information was provided on the spilt between partial and total KR surgery. Six studies used the KDIGO classification to diagnose AKI and two studies used the AKIN classification. The RIFLE classification was not used in any of the included studies.
A risk of bias assessment was undertaken for all included studies using the ROBINS-I tool (Figure 2) [29].
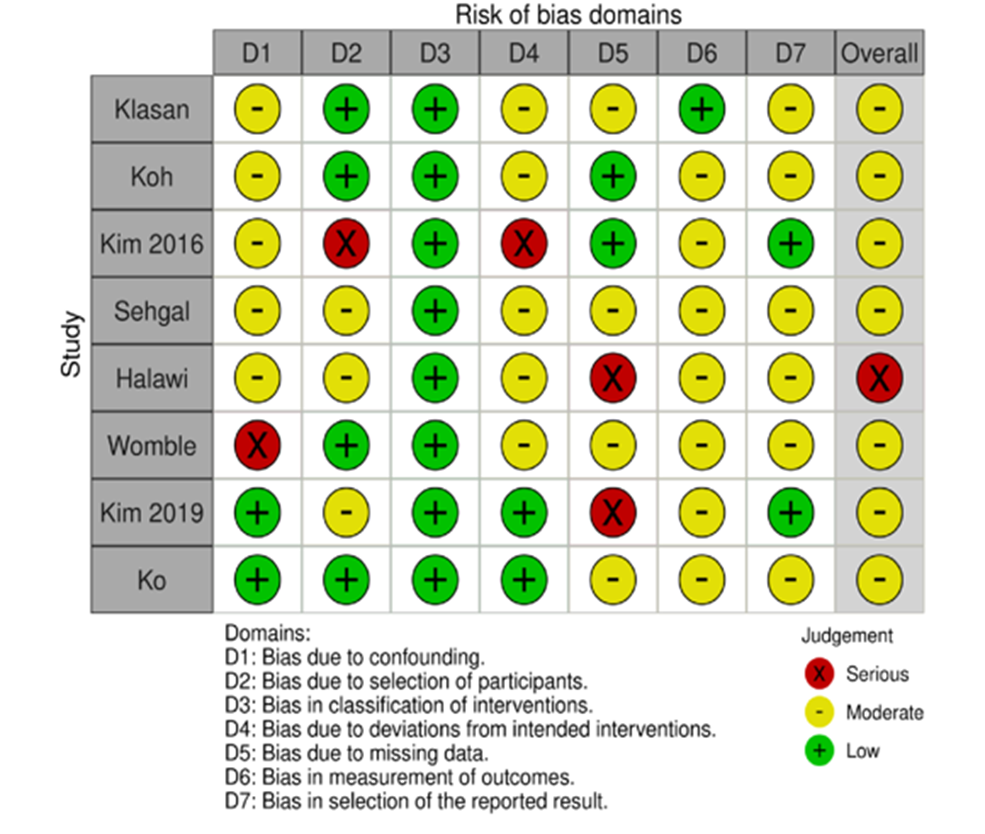
ROBINS-I, visual representation showing domain and overall level data
All studies were listed as low risk of bias in the classification of interventions. Regarding cofounders, there was a moderate risk of bias highlighted in five studies [34-38] and a serious risk of bias in one study [32]. The studies by Halawi [33] and Kim [34] were at high risk of bias for missing data. On overall rating with the ROBINS-I tool, seven of the studies included in this review were at moderate risk of bias, with one study at serious risk of bias [33]. (Figure 2)
The MINORS score across all papers is demonstrated in Appendix 2
Appendix 2: MINORS criteria scoring for each study
| Klasan 2021 | Kim 2016 | Koh 2018 | Sehgal 2014 | Halawi 2020 | Womble 2019 | Kim 2019 | Ko 2022 | |
| 1.Clearly stated aim | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 |
| 2.Inclusion of Consecutive patients | 1 | 1 | 2 | 1 | 0 | 1 | 2 | 1 |
| 3.Prospective data collection | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 4.Endpoints appropriate to aim of study | 2 | 1 | 1 | 0 | 2 | 0 | 1 | 2 |
| 5.Unbiased assessment of study endpoint | 2 | 2 | 2 | 2 | 1 | 0 | 2 | 2 |
| 6.Follow up period appropriate to aim of the study | 2 | 1 | 1 | 0 | 2 | 1 | 1 | 2 |
| 7.Loss to follow up less than 5% | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 2 |
| 8.Prospective calculation of study size | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| 9.Adequate control group | 2 | 2 | 2 | 2 | 2 | |||
| 10.Contemporay groups | 1 | 2 | 2 | 2 | 2 | |||
| 11.Baseline equivalence of groups | 1 | 2 | 1 | 1 | 2 | |||
| 12.Adequate statistical analysis | 2 | 2 | 2 | 0 | 2 | |||
| Total score | 18 | 18 | 17 | 7 | 9 | 12 | 17 | 13 |
[30]. The mean score across all papers was 14, with a breakdown of a mean score of eight for non-comparative studies and 15.8 for comparative studies. All studies scored three on the OCEBM Rating.
Incidence of AKI
The eight included studies had a total of 13,574 episodes of patients undergoing primary KR. The weighted pooled mean age of patients was 68.91 years (SD 2.68). 9,046 (73.67%) of the patients were female. The weighted pooled incidence of AKI in the included studies was 8.85 (95% CI 8.35%-9.35%).
On subgroup analysis of the classification system used to diagnose AKI. The KDIGO and AKIN groups had a weighted pooled AKI rate of 7.56% (95% CI 7.01%-8.05%) and 15.80% (95% CI 13.32 to 18.50%) respectively.
The pooled incidence was 7.93 (95% CI 7.36% to 8.34%) for South Korea and 11.73 (95% CI 11.43% to 12.04%) for the USA.
Renal Replacement Therapy
Two studies identified in this review reported the overall incidence of RRT following KR surgery, this was reported as 0.004% [35] and 0.003% [34].
The paper by Ko et al demonstrated that 2.2% of the patients that developed AKI following KR progressed to requiring RRT in comparison to 0.2% of the non-AKI patients. The odds ratio for requiring RRT for the AKI group in comparison to the non-AKI group was 9.8 (95% CI 4.3–22.4) [35].
Risk factors
Age [33,35–37], diabetes mellitus [33,35,37] and a preoperative diagnosis of chronic kidney disease (CKD) [33,35,38] were identified as independent risk factors for AKI.
Two papers reported a reduced risk of AKI with spinal anaesthesia over a general anaesthetic, although the results were not statistically significant [34,35]. The paper by Womble et al, demonstrated that African Americans were at higher risk of AKI than Caucasians [32]. No other ethnic groups were included in this analysis due to low patient numbers.
Koh et al, [35] demonstrated a significantly reduced risk of AKI in staged bilateral KR when the second surgery was within 7 days) (2.4%) (p>0.001); compared with staged KR when the second surgery was performed between 8 days and one year later (6%), or simultaneous groups (on the same day) (11.2%).
American Society of Anaesthesiologists (ASA) score was found to be a risk factor for AKI in two studies [33,35], with an ASA score of 3 or greater associated with a higher risk of developing post-operative AKI. The study by Kim et al, demonstrated that serum albumin less <3>
This review of eight studies and 13,574 surgical procedures has shown a weighted pooled incidence of AKI following KR of 8.85% (95% CI 8.35- 9.35). The pooled rate of AKI following KR reported in this study is similar to rates that have previously been reported in a systematic review and meta-analysis of the incidence of AKI following total hip replacement (6.3%) [15]. The incidence of AKI is, however, lower than that following other major operations, including heart valve replacement (AKI incidence 35% to 47%) [39], vascular surgery [40,41] (AKI incidence approximately 25%) or coronary artery bypass grafting (AKI incidence approximately 25%) [42].
Patients who develop AKI carry significant risks of prolonged hospital stay, with an increased likelihood of re-admission and mortality [43-46]. Only two studies reported data on the requirement for RRT. The incidence is RRT is low, but may be required in patients who develop AKI following KR [8,34]. The RRT odds ratio for patients with AKI compared to non-AKI was 9.8 (95% CI 4.3-22.4) [8]. Even mild AKI is associated with poor long-term outcomes including the progression to CKD and the development of cardiovascular disease [45]. This association highlights the importance of preventative measures to reduce the overall incidence of AKI, and to diagnose AKI postoperatively to permit early intervention.
The Incidence of AKI reported in the study by Sehgal et al. 21.9% [37], is significantly higher than that reported in the other studies included in this review. The reason may be the classification system used to diagnose AKI. The study diagnosed AKI with the AKIN classification and the majority of the patients had stage 1 AKI, 87.9% (120/137). However, another study that used the AKIN classification criteria had an AKI rate of 3.3% [33]. The AKI rate in the Sehgal study was significantly higher in the cohort of patients from 2008 than 2009 (odds ratio 0.55, 95% CI 0.37 to 0.82) for which the authors were unable to explain. The mean age of patients in the Sehgal paper (67.90 years) [37] was lower than the weighted pooled mean for this review (68.91 years), but there was a higher prevalence of diabetes (24.45%)[37] compared with other studies [9,34-36,39,40] (18.86%).
There was a significant heterogeneity in how studies collected and analysed risk factors for AKI. The risk factors for AKI highlighted in this study are similar to those published for other surgical procedures [47]. Of the risk factors identified, pre-operative CKD was highlighted as the strongest risk factor in predicting AKI by Ko et al [8]. Clinicians should consider peri-operative interventions for patients with commonly identified risk factors (Age>65, diabetes and CKD). Ko et al. have published a risk assessment and prediction tool based on their study [8].
The pooled incidence of AKI reported in this review is higher than that reported in some large cohort studies that use coding data for the identification of AKI [11,19,20]. These studies were excluded from this review as the clinical criteria used to diagnose AKI was unclear [11,19,20]. Previously studies demonstrated that the sensitivity and positive predictive value for ICD-10 and billing code data to identify AKI is poor [48,49]. The sensitivity of ICD-10 codes has been reported for all AKI as 25.7% and 35.8% [48]. The sensitivity of billing code data for the correct identification of AKI has been reported at 17.2% [49]. The rates of AKI recorded in the big data studies [11,20,50,51] 0.05%, 0.5%, 0.33% and 1.3%. respectively, were significantly lower than the results of all studies included in this review. This finding is consistent with the underreporting of AKI in large datasets.
The results of this review are valuable for clinical practice. Knowing the incidence of AKI following KR surgery allows clinicians to provide more accurate information to their patients preoperatively. A post-operative incidence of 8.85% makes AKI one of the most common medical complications following KR surgery [52-54]. Patient with risk factors for AKI should receive preoperative optimisation and postoperative measurement of their renal function.
The limitations of this study include the retrospective and non-randomised design of studies included in this review, which may be a source of bias. All the included studies were felt to be at moderate to serious risk of bias.
A further limitation is this review has only included studies from the USA, South Korea and New Zealand. Ethnicity has been highlighted as a risk factor for AKI and therefore it is unclear if the results of this review would be generalisable to all healthcare institutions [32].
Further high-quality population-based studies evaluating the incidence of AKI following primary KR are required to provide a more accurate representation of the incidence.
The weighted pooled incidence for AKI following KR is 8.85% (95% CI 8.35- 9.35). There is limited data on the incidence of progression to the requirement for RRT following primary KR. Risk factors for AKI include age over 65, CKD and diabetes mellitus.
AKI is one of the most common complications following KR surgery. Clinicians should therefore acknowledge this potential complication in their pre-operative consenting of patients prior to KR surgery. Further research should be undertaken into perioperative interventions that reduced the risk of AKI. Patients at high risk of AKI should have their renal function monitored postoperatively.
JD- Proposition idea for paper, search design and carrying out, preparation of manuscript, writing of manuscript
TW- Search, Reviewing manuscript
AA- Reviewing manuscriot , Wirting of manuscript
AP- Proposition idea for paper, search design, preparation of manuscript, writing of manuscript
BK- Reviewing manuscriot , Wirting of manuscript
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
