
Case Report | DOI: https://doi.org/10.31579/2690-4861/028
*Corresponding Author: Varun Shah, Department of Neurology, University of Texas Medical Branch, Galveston Texas.
Citation: Varun S, Alok D. (2020) Acute Kidney Injury Complicating the Management of Fatal Cerebral Edema after Cannabinoid Use – Case Report and Literature Review. International Journal of Clinical Case Reports and Reviews. 2(5); DOI: 10.31579/2690-4861/028
Copyright: © 2020 Varun Shah, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 June 2020 | Accepted: 29 June 2020 | Published: 02 July 2020
Keywords: neurocritical care; cannabis; cannabinoid; acute kidney injury; cerebral edema
Case Description: 19-year-old man with history of marijuana and Synthetic Cannabinoids use presented with status epilepticus. Labs showed tetrahydrocannabinol in urine. Imaging showed diffuse cerebral edema with non-traumatic subarachnoid hemorrhage. Intracranial pressure (ICP) was elevated to 30 mmHg. This was complicated by severe refractory metabolic acidosis with persistently elevated ICP unresponsive to medical care and cerebrospinal fluid drainage. Five days later patient suffered cardiac arrest from severe acidosis and metabolic derangements. Patient could not be resuscitated, and family withdrew care.
Discussion: This case highlights the many challenges in managing a critically ill patient with cerebral edema and renal failure with medically refractory metabolic acidosis. Synthetic Cannabinoids are undetectable on routine drug screens and exposure is difficult to establish. Synthetic Cannabinoids can lead to multi-organ failure and death that may result from cardiovascular events, respiratory depression, pulmonary complications and acute kidney injury. A high clinical suspicion is warranted in at-risk patients.
Conclusion:Clinicians should always consider Synthetic Cannabinoids use in high-risk patient and anticipate multi-organ damage for early intervention. Further research is needed to establish causality, improve detection and devise appropriate therapeutic strategies in managing such patients
The prevalence of cannabis (marijuana) and synthetic cannabinoids (SCs) is increasing in recent times due to an international push towards its legalization. Admissions to the Neurocritical Care units from cannabis and/or cannabinoid related adverse health events are increasing. While acute neurological symptoms are common and well-documented in the literature [1], it’s important that Neurologists familiarize themselves with the entire spectrum of ill-effects of the cannabinoids as involvement of multiple organ systems can complicate the management of a primary neurological problem in a critically ill patient. Particularly, acute kidney injury is under-reported with synthetic cannabinoid use and can complicate the management of a critically ill neurology patient.
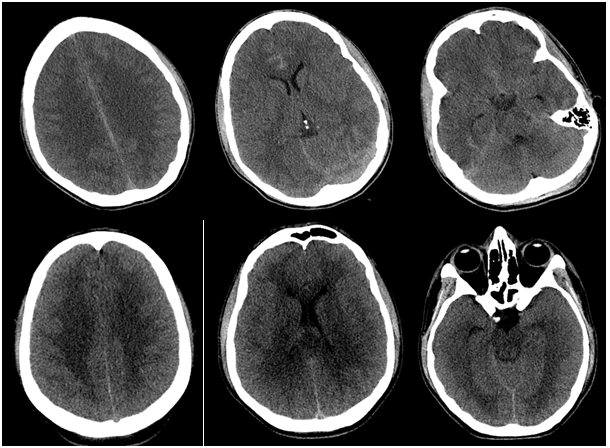
A 19-year-old Caucasian male with known cannabis and SCs abuse was admitted to our institution after new-onset seizures. History was positive for headaches, sleep deprivation and recent marijuana use. He was intubated emergently followed by intravenous levetiracetam and naloxone administration. However, clinical exam remained unchanged and was noted to have restlessness, inability to follow commands and preserved brainstem reflexes. Urine drug screen was positive for delta-9-tetrahydrocannabinol (THC). Non-contrast CT Head showed diffuse cerebral edema with cortical sulcal hyperdensities (Figure 1) suspicious for subarachnoid blood and CT angiogram of head and neck was unremarkable for aneurysm or other vascular malformations.
Neurosurgery was consulted and an external ventricular drain (EVD) placement revealed elevated intracranial pressure (ICP) around 30 mmHg. Hyperosmolar therapy was immediately initiated to maintain serum Sodium between 145 and 155 mEq/L. There was initial radiographic improvement in cerebral edema without clinical change. Patient developed acute kidney injury (AKI) with a steady deterioration in glomerular filtration rate, metabolic acidosis, hypocalcemia, and hyperkalemia. AKI made ICP management difficult as hyperosmolar therapy could not be titrated up given risk for electrolyte derangement and volume overload. Transient neuromuscular blockade was tried with transient drop in ICP. EVD was exchanged but showed consistent results with ICP more than 30 mmHg. Nephrology was consulted for continuous renal replacement therapy to stabilize him for a surgical decompression. However, the patient developed ventricular fibrillation. Return of spontaneous circulation was achieved after 15 minutes of resuscitation but then shortly after he had a second cardiac arrest with asystole. Family decided to abort resuscitative measures and he was declared dead subsequently.
Discussion
Out of the five-hundred compounds extracted from Cannabis, sixty-five are classified as cannabinoids. SCs abuse can be difficult to establish unless self-reported, as they are not detectable by standard lab tests. A high clinical suspicion is warranted in such at-risk patients. Their abuse can lead to multi-organ failure and even death that may result from cardiovascular events, respiratory depression, pulmonary complications or AKI.
There is a report of cerebral edema in three fatal cases from Germany with post-mortem drug analysis showing SCs from various body tissues [2]. However, there are no case reports of SCs related combination of cerebral edema, refractory renal failure with metabolic acidosis and new onset seizure as found in the case being reported by our team.
A rare but clinically significant adverse effect of Cannabis consumption that is under-reported in the literature includes acute kidney injury. Both CB1 and CB2 receptors are expressed in kidneys. In animal models of AKI, CB receptor activation is associated with increased production of reactive oxygen species, which can either activate NF-κβ-dependent transcription of downstream proinflammatory target genes, or alternatively activate p38 MAPK and JNK. In the end, both pathways activate programmed cell death by apoptosis [3].
As demonstrated above, in addition to direct nephrotoxicity, the severe refractory metabolic acidosis from AKI associated with synthetic cannabis abuse can prove to be fatal. This case highlights the many challenges in managing a critically ill patient with cerebral edema and renal failure with medically refractory metabolic acidosis. Having a low threshold for suspecting cerebral edema and renal failure may potentially help save other patients who may have a similar clinical presentation. Unfortunately, as the use and abuse of the Marijuana gets more socially acceptable, similar presentations are likely to become more common.
Conclusion:
The spectrum of physiological and pathological effects of Cannabis and synthetic cannabinoids is not yet fully understood. Due to the increasing acceptance of marijuana in society-at-large, use of Cannabis is likely to become more prevalent. The perceived benefits of medical marijuana need to be compared with the known and potential health risks, both short and long-term, before accepting it at a community level [4]. Synthetic marijuana detection and control of natural marijuana contamination by appropriate use of legal and judicial measures needs to be strictly placed to avoid serious health consequences, especially to the younger generation. Further large-scale studies are warranted to evaluate the impact of this upcoming health challenge to the physicians and the society.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
