
Review Article | DOI: https://doi.org/10.31579/2692-9759/080
1 Laboratory of Interventional Cardiology - Universidade Estadual de Campinas (UNICAMP), Campinas, Brazil.
2 Nephrology Department, BP - A Beneficência portuguesa de São Paulo, São Paulo, Brazil.
*Corresponding Author: Tania Leme da Rocha Martinez, Nephrology Department, BP - A Beneficência portuguesa de São Paulo, São Paulo, Brazil.
Citation: Gioppato S, Gascòn V, Anita L R Saldanha, Tania L R Martinez.(2022). Acute Kidney Injury After Exposure to Iodized Contrast Medium. Cardiology Research and Reports. 4(6); DOI:10.31579/2692-9759/080
Copyright: © 2022 Tania Leme da Rocha Martinez, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 September 2022 | Accepted: 21 October 2022 | Published: 17 November 2022
Keywords: acute kidney injury; iodized contrast; kidney protection; creatinine
Acute Kidney Injury can be caused by a series of conditions. In this paper, the focus is the use of iodinated contrast and the conditions that may even diminish this risk. Precautions are indicated in admitted patients: isotonic saline solution seems to be better than more hypotonic fluids. It is proposed that the saline be used instead of bicarbonate, because it has no greater benefits than the saline and is more expensive. Generally, contrast nephropathy is defined as an increase of at least 0.5 mg/dL or 25% of baseline creatinine within 2 to 5 days of contrast exposure. A study group of Kidney Disease Improving Global Outcomes (KDIGO) suggested a definition of an increase of 1.5 times or more in basal creatinine within 7 days of contrast use, an increase of at least 0.3 mg per deciliter above baseline within 48 hours after exposure to contrast or a urinary volume of less than 0.5 ml/kg of body weight per hour persisting per hour, at least 6 hours after exposure. Risk factors for contrast-associated nephropathy: preexisting chronic kidney disease; use of high osmolarity contrast; high volume of contrast (>350 mL or >4 ml/kg); repeat contrast in less than 72 hours. Contrast-associated nephropathy impacts in clinical practice: many studies have shown that contrast-associated renal injury is related to increased mortality, in addition to being related to the progression of underlying chronic kidney disease.
AKI: Acute Kidney Injury
CIN: Contrast-Induced Nephropathy
ICM: Iodinated Contrast Medium
PC-AKI: Post-Contrast Acute Kidney Injury
Scr: Serum Creatinine
Acute kidney injury (AKI) after exposure to iodinated contrast medium (ICM), or simply post-contrast AKI (PC-AKI) is one of the forms of AKI, where ICM plays a prominent role in pathophysiology and represents a marker of poor prognosis, being associated with serious adverse events such as death, infarction, dialysis as well as longer hospital stay and cost. Because it is a form of renal deterioration with well-known and predictable risk factors, its prevention plays a prominent role. Thus, full knowledge of the disease, risk factors and evolution are fundamental elements for prevention, early diagnosis, reduction of incidence and optimization of treatment [1-5].
Contrast-Induced Nephropathy (CIN) is the most widely used terminology. However, evidence shows that many individuals who develop PC-AKI also exhibit other factors potentially capable of facilitating or inducing kidney injury. Thus, the contrast medium would not be the only causal agent as the term CIN may erroneously suggest.
Based on this evidence, the 2011 Guideline of the Contrast Media Safety Committee of the European Society of Urogenital Radiology (ESUR) proposed that the term PC-AKI should be preferred over the term CIN, thus placing the ICM as a potential causal agent and not the main responsible for renal injury [6].
PC-AKI is a constant concern for interventionists and radiologists, with an occurrence ranging from 3 Percentage to 19 Percentage of contrasted procedures. This wide variability in incidence is a reflection of differences in the study designs regarding the route of administration of the ICM, the type of population, the type of procedure and, finally and more importantly, the criteria that define PC-AKI. The criteria most frequently used to characterize PC-AKI are based on absolute elevation of basal serum creatinine (SCr) greater than0.5 mg/dL or relative increase greater than25 Percentage within 48h-72h after exposure [7-8]. However, there has never been a consensus on these values.
In order to standardize the nomenclature and refine diagnostic and prognostic sensitivities, two criteria of wide acceptance were developed. The first of these, the RIFLE criterion (Risk, Injury and Failure, Loss of kidney function, and End-stage kidney disease of 2004 prioritized the definition in three stages of renal damage (risk, injury and failure) and two stages of evolution (loss of function and end-stage) based on changes in SCr and urinary output in a time interval of seven days. Later in 2007, the Acute Kidney Injury (AKIN) criterion, based on the premise that even small changes in SCr can significantly impact mortality, sought to make the RIFLE criterion more rigorous and thus achieve better levels of sensitivity and reproducibility.
In the new proposal, the AKIN criterion proposed that minimum SCr changes, such as an increase ≥0.3 mg/dl within 48 hours or a relative increase ≥ 50 Percentage of baseline value within seven days already configure AKI [9]. Despite good sensitivity and reproducibility, the RIFLE and AKIN criteria reflect the reality of patients hospitalized in intensive care settings who accumulate multiple health problems, which makes it difficult to separate cases actually related to ICM from those in which AKI originates from other causes.
In 2012, the KDIGO (Kidney Disease Improving Global Outcome) working group sought to broaden the scope of the RIFLE and AKIN criteria to encompass both adults and children at risk of AKI, including for the first time in a kidney injury criterion, PC-AKI. The KDIGO criterion classifies AKI into stages 1, 2 and 3 (Table 1) by defining it as an elevation of SCr ≥0.3 mg/dl within 48 hours, or elevation of serum levels in at least 50 Percentage of the reference value in seven days, or urinary volume less than 0.5 mL/Kg/h for six consecutive hours [10].
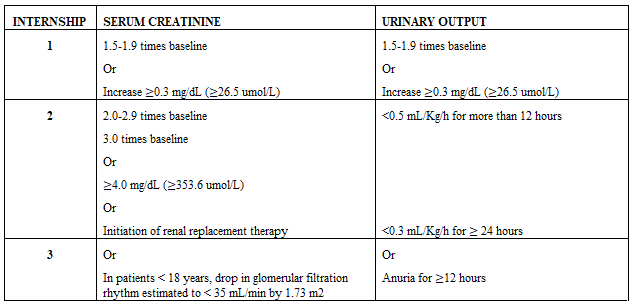
Table 1: Kidney Disease Improving Global Outcome (KDIGO) criteria for acute kidney injury.
AKI exhibits complex pathophysiology, with several pathways of aggression to the endothelium and tubular cell. The main risk factor is previous renal dysfunction accompanied by others such as diabetes, anemia, hyperglycemia, heart failure, volume depletion and hemodynamic instability [6]. Clinically, she is studying SCr elevation starting between the second and third days, peaking between the seventh and tenth days, and complete or almost complete resolution between the second and third weeks after exposure to ICM. However, in some cases (0.06 Percentage to 0.3 Percentage) it may progress to chronic kidney disease requiring dialysis [11].
Risk Prediction
Risk assessment has been a key element in the effort to define which factors impact the chance of developing a given outcome and thus identify new markers, identify and access potential targets and optimize the cost effectiveness of a given therapy or the implementation of interventions. These models gain greater relevance in contemporary medical practice, where the vision of a more cost-effective and patient-centered medicine requires an even greater concern for institutions and health professionals with the quality of care and patient safety [12-14].
The currently available research data is insufficient to state that contrast agents are not nephrotoxic. Then, a prudent approach to the care of patients undergoing contrast procedures involves the careful implementation of evidence-based preventive care for patients identified as being at higher risk of AKI.
Research on the prevention of contrast-associated AKI has focused mainly on the use of renal replacement therapies, pharmaceutical agents and intravenous crystalloids. The benefits of prophylactic renal replacement therapy and most pharmaceutical agents have not been proven, making the supply of epiprocedural intravenous crystalloids the main intervention to reduce risks.
There is still no defined protocol for the prevention of contrast-associated nephropathy with saline use. The uptodate suggests the following scheme:
Outpatients: administer 3 mL/kg in one hour before the procedure and 1 to 1.5 mL/kg/hour for four to six hours after the procedure, with administration of at least 6 mL/kg after the procedure.
Hospitalized patients: administer 1 mL/kg/hour for 6 to 12 hours pre-procedure, intraprocedure and for 6 to 12 hours after the procedure.
It is recognized that, collectively, these studies [15-34] and others similarly, increased awareness of AKI associated with contrast and stimulated research to identify preventive strategies. However, it points out that it is possible that AKI associated with contrast injury is actually a marker of increased risk of adverse outcomes rather than a mediator of such results.
Although small postoperative elevations in plasma creatinine levels are associated with increased mortality at 30 days, small decreases in creatinine plasma (≤ 0.5 mg per deciliter) were also associated with increased mortality. In addition, a meta-analysis by Coca et al [35]. showed that interventions that reduced the incidence of AKI by almost 50 Percentage failed to reduce the risk of long-term death or the development of chronic kidney disease. These observations raise doubts about the causal relationship between small increments in plasma creatinine levels after contrast administration and adverse side events.
Another important problem is that creatinine is not specific to contrast kidney injury, so using it as a definition parameter can lead to misinterpretations. To date, there have been no adequate clinical trials showing that prevention of AKI results associated with contrast in a survival benefit.
There are a number of precautions to be taken when there is use of iodinized contrast as to the risk of AKI, such as preexistence of kidney disease, contrast osmolarity, contrast volume, among many others that the clinician will point out depending on the peculiarities of each patient.
None
No conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
