
Case Report | DOI: https://doi.org/10.31579/2693-4779/088
1 The First College of Clinical Medical Science, China Three Gorges University, Yichang, China.
2 Institute of Digestive Disease, China Three Gorges University, Yichang, China.
3 Department of Gastroenterology, Yichang Central People’s Hospital, Yichang, China.
*Corresponding Author: Wei Liu, Ph.D., The First College of Clinical Medical Science, China Three Gorges University, Yichang, China.
Citation: Y Lu, S-H Zheng, W Liu. (2022) Acute Hepatitis E With Elevated Alpha Fetoprotein: A Case Report and Literature Review. Clinical Research and Clinical Trials. 5(4); DOI:10.31579/2693-4779/088
Copyright: © 2022 Wei Liu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 March 2022 | Accepted: 21 March 2022 | Published: 29 March 2022
Keywords: acute hepatitis e; jaundice; alpha fetoprotein; severe hepatitis
Acute Hepatitis E (AHE) is an acute self-limiting disease caused by Hepatitis E virus infection, which is mostly transmitted through the digestive tract. A few patients can lead to severe hepatitis and liver failure. Alpha fetoprotein is a sensitive serological marker of primary liver cancer. AFP may increase in different degrees in patients with gastrointestinal tumors, endodermal sinus tumors and germ cell carcinoma originating from endoderm. In addition, serum AFP can also be elevated in varying degrees in non-neoplastic acute and chronic liver diseases. We here report a case of Acute Hepatitis E with elevated serum AFP, and discuss the clinical characteristics and significance of elevated AFP in Acute Hepatitis E through literature review.
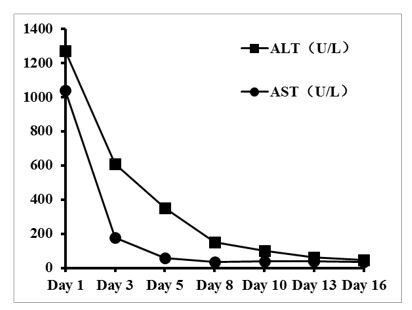
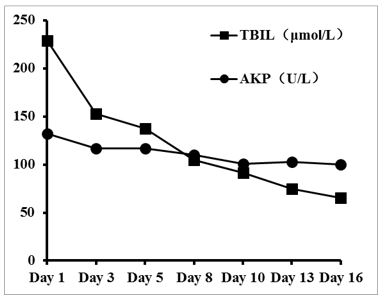
A 57-year-old female patient was admitted to our hospital on December 6, 2020 for “yellow skin staining for 2 weeks”. The patient presented with yellow sclera, yellow urine, and discolored stools without any obvious cause two weeks ago. The symptoms worsened gradually, accompanied by loss of appetite, nausea, and vomiting. Vomiting is worsened after eating greasy food. Symptom combined with exhaustion, poor appetite, and fever. There was no chill. The highest temperature was 37.8℃. The liver function test at the local hospital 1 day ago showed that total bile acids 251.7 μmol/L, total bilirubin 293 μmol/L, direct bilirubin 166.5 μmol/L, indirect bilirubin 126.5 μmol/L, alkaline phosphatase 183 U/L, glutamyl transferase 43.6 U/L, and glutamate transaminase 1518.8 U/L. Color ultrasound showed slightly strong echogenicity in the gallbladder cavity. CT suggested soft tissue density shadow in the gallbladder, fatty liver, gallbladder fossa fluid accumulation, and a diverticulum in the descending duodenum. The patient had no specific medical history and denied any history of allergy, herbal medicine, alcohol or tobacco use. Physical examination after admission suggested a temperature of 36.3°C, a pulse of 84 beats/min, and respiration of 20 breaths/min. Blood pressure was 127/89 mmHg. The patient had yellow skin, yellow sclera, and clear breath sounds in both lungs. No murmur was heard in each valve auscultation area. The abdomen was flat and soft with no obvious pressure pain and rebound pain. The liver, spleen, and rib were all in normal size. Murphy's sign was not detected. Bowel sound was normal. Laboratory tests suggested glutamate transaminase 1272 U/L, glutamic oxalacetic transaminase 1040 U/L, total bilirubin 228.80 μmol/L, direct bilirubin 134.63 μmol/L, alkaline phosphatase 132 U/L, and glutamyl transpeptidase 33 U/L. Blood routine examination, liver and kidney function, blood coagulation function, cardiac enzyme and amylase performed normally. Negative hepatitis B surface antigen, negative hepatitis B surface antibody, and positive hepatitis B core antibody were confirmed. Autoimmune liver disease antibodies were normal. ENA and ANCA were negative. Thyroid function and IgG4 were normal. Human immunodeficiency virus antibodies and syphilis antibodies were normal. Hepatitis E antibody IgM was positive. Hepatitis A antibody IgM was negative. Hepatitis C antibody IgG was negative. MR Cholangiopancreatography (MRCP) suggested gallbladder wall edema, pancreatic swelling with a little exudate, fatty liver, and bilateral renal cysts. CT examination of the whole abdomen suggested uneven thickening of the gallbladder wall, gallbladder fossa fluid accumulation, hepatic cysts, low-density foci in the spleen, and multiple small cysts in both kidneys. no significant abnormalities were shown in Cardiac ultrasound, gastroscopy, cranial, and chest CT.
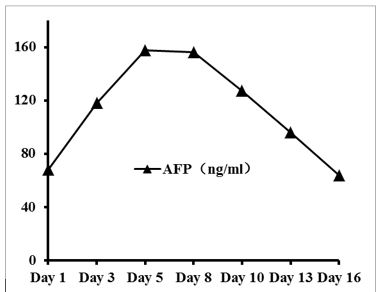
The patient had jaundice as the first symptom. Hemolytic jaundice has been excluded. MRCP did not show any obvious intra- and extra-hepatic bile duct obstruction. Obstructive jaundice was excluded. Serum IgG4 examination was normal. IgG4-related cholangitis and pancreatitis was excluded. Hepatitis E were considered due to hepatocellular jaundice and positive IgM antibodies to HEV. Finally, viral hepatitis E with acute severe jaundice was diagnosed. The patient denied unclean diet and aggregation of morbidity. Treatment included glutathione, compound glycyrrhizin, adenosylmethionine, ursodeoxycholic acid, and polyenylphosphatidylcholine. Transaminases, bilirubin, alkaline phosphatase, and AFP were monitored during hospitalization. About 1 week after admission, the patient's serum alanine transaminase, glutamic oxalacetic transaminase, total bilirubin, and alkaline phosphatase decreased significantly (Figure 1, Figure 2). In contrast, the patient's serum AFP rose rapidly after admission with a peak around 1 week, and thereafter showed a gradually decreasing trend (Figure 3). At the time of discharge, the patient's jaundice had subsided. The gastrointestinal symptoms had improved significantly. The cardiopulmonary and abdominal physical examinations did not show any abnormalities. The transaminases, total bilirubin, alkaline phosphatase, glutamyl transpeptidase, and AFP returned to normal level.
AHE is an acute self-limiting disease caused by Hepatitis E Virus (HEV) infection [1]. Although hepatitis B is the predominant cause of viral hepatitis in China overall, AHE has taken the lead in acute viral hepatitis in adults in most areas. The transmission routes of AHE include gastrointestinal transmission, blood transfusion transmission, vertical transmission, and close contact transmission, among which gastrointestinal transmission is the most important form of transmission. Most patients with disseminated form have a history of unclean diet [2]. Anti-HEV IgM antibodies first appear in 3-4 days after HEV infection, and anti-HEV IgG antibodies can be detected about 1 week later. Positive anti-HEV IgM is a reliable indicator of recent HEV infection [3]. The clinical presentation of patients with AHE lacks specificity. In most individuals, HEV infection is asymptomatic. In patients with symptomatic AHE, the main manifestation is acute jaundice with an incidence of 5-30%. The main manifestation is hepatocellular jaundice, which is currently thought to be caused by increased hepatocyte membrane permeability and dysfunctional uptake, binding and excretion of bilirubin, of which most patients have varying degrees of intrahepatic cholestasis. AHE is an acute self-limiting disease, but a small number of patients can progress to severe hepatic decompensation or even liver failure, mostly in the elderly, pregnant women, and patients with underlying liver disease [4]. Many cases of AHE complicated by acute liver failure resulting in death have also been reported [5, 6]. There are no specific antiviral drugs for AHE. The main treatment is symptomatic, such as routine bed rest, avoidance of exertion, nutritional support, increasing blood flow to the liver, dietary modification, liver function protection, and artificial liver blood purification techniques. It has been shown that adenosylmethionine combined with ursodeoxycholic acid in the treatment of acute hepatitis E complicated by jaundice has a synergistic effect in promoting the resolution of jaundice and improving liver function.
AFP is a serum glycoprotein that is synthesized by the liver. AFP rises significantly when hepatocellular carcinoma or germinal embryonal tumors associated with embryogenesis are present [7, 8]. Several studies have shown that AFP can also be used to reflect hepatocyte regeneration [9-11]. Therefore, AFP can be used as one of the important observational indicators to assess the severity and prognosis of acute hepatitis. Varshney [12] showed that the dynamics of AFP rather than the absolute value of AFP determines the prognosis of patients with liver failure by monitoring serum AFP in patients with liver failure during the course of the disease. Lin [13] studied the mechanism of AFP transcriptional activation by transgenic mice and found that AFP is elevated differently in early embryonic stages, during liver regeneration and malignant liver proliferation. The Hepatitis B virus X protein has been reported to activate and induce AFP expression in multiple ways [14-17]. The mechanism of AFP elevation in AHE needs to be further explored.
Cases of AHE with elevated AFP have been reported occasionally. Liver tissue damage is more severe in patients with AHE with elevated AFP. When AHE develops into acute severe hepatitis, there can be massive hepatocyte destruction. As the disease develops, AFP tends to increase and then decrease. As hepatocytes are actively regenerating, new hepatocytes can synthesize and secrete AFP corresponding to the number of new cells. The serum AFP concentration usually does not exceed 400 ng/ml. As the disease progresses and the regenerating hepatocytes differentiate and mature, the serum AFP concentration gradually returns to normal with the process usually taking less than 3 months. Therefore, monitoring AFP in patients with AHE-related severe hepatitis has significant prognostic significance. AFP level rising above 1000 ng/ml may result in misdiagnosis if hepatocellular carcinoma was easily diagnosed. However, if patients with severe hepatitis present with consistently high AFP levels, they should be alerted to the possibility of hepatocellular carcinoma.
Transaminases, bilirubin, and alkaline phosphatase were significantly elevated in this AHE patient, which suggested severe hepatocellular injury and cholestasis. The elevated AFP indicates a reflection of hepatocyte injury and post-necrosis hyperplasia. The prognosis of this patient may be influenced by the dynamic changes in the level of AFP. After active treatment, the liver function indicators and AFP gradually returned to normal level. The patient still needs to be monitored regularly for liver imaging and dynamic changes in AFP to alert deterioration or the possibility of hepatocellular carcinoma. In addition, hepatobiliary and pancreatic imaging showed uneven thickening and echogenicity of the gallbladder wall, edema of the gallbladder wall, fluid accumulation in the gallbladder fossa, and swelling of the pancreas with a little exudation. However, the patient had no significant abdominal pain but normal inflammatory parameters such as neutrophils, C-reactive protein, erythrocyte sedimentation and calcitoninogen. So cholecystitis and pancreatitis were not considered. It is presumed that the changes in hepatobiliary and pancreatic imaging may be related to the non-specific manifestations of AHE.
The authors have no conflicts of interest to declare.
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Written informed consent was obtained from the patient for publication of this “Case Report”.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
