
Case Report | DOI: https://doi.org/10.31579/2690-4861/722
Servicio de Medicina Interna del Hospital Universitario Infanta Leonor, Madrid, España.
*Corresponding Author: Mariano Ulla-Anes, Servicio de Medicina Interna del Hospital Universitario Infanta Leonor, Madrid, España.
Citation: Mariano Ulla-Anes, Elisa Fernández-Vidal, Ana Isabel Franco-Moreno, Juan Torres-Macho, Eva María Moya-Mateo, (2025), Acute Diverticulitis as A form of Presentation of Follicular Lymphoma of the Colon, International Journal of Clinical Case Reports and Reviews, 24(2); DOI:10.31579/2690-4861/722
Copyright: © 2025, Mariano Ulla-Anes. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 February 2025 | Accepted: 07 March 2025 | Published: 14 March 2025
Keywords: lymphoma; follicular; diverticulitis; lymphadenopathy; colon
Follicular lymphoma is the second most-common subtype of non-Hodgkin lymphoma, after Diffuse large B-cell lymphoma. Primary lymphomas of the gastrointestinal tract are rare, with secondary intestinal involvement being more common. We present the case of a 68-year-old male patient who was diagnosed with colonic follicular lymphoma during the study for recurrent acute diverticulitis.
Follicular lymphoma (FL) is the second most prevalent non-Hodgkin lymphoma, although colonic involvement is rare. The usual clinical presentation is diarrhea, abdominal pain, constipation and micro or macroscopic bleeding [1].
Below, we present the case of a patient who was diagnosed with colonic follicular lymphoma during the study of recurrent acute diverticulitis.
History and current illness:
A 68-year-old man with no relevant history except for an episode of acute diverticulitis in April 2021, with involvement of the mesosigma and Hinchey type I B intramural collection, which was managed conservatively. In the outpatient follow-up of this process, after several weeks of antibiotic therapy, an abdominopelvic CT scan was performed, which showed a practical resolution of the intramural collection but with persistence of retroperitoneal lymphadenopathy of significant size, as well as abundant mesenteric, mesosigma, and iliac lymph nodes. A colonoscopy was performed that showed an edematous and stenotic area about 20 cm from the anal sphincter that appeared to be post-inflammatory. Proximal to this, a mucosa with spontaneous bleeding was observed that was biopsied. No malignant lesions were detected. In the meantime, while waiting for the anatomopathological results, the patient presents with acute abdominal symptoms (pain, distension and absence of bowel movements) for which he goes to the emergency room and is admitted.
Physical exploration:
Cardiorespiratory examination without relevant findings, the abdomen was soft, painful on deep palpation in the hypogastrium and left iliac fossa, although without signs of peritonism, rectal examination without alterations.
Supplementary tests:
The initial blood analysis revealed a leukocytosis of 15,000/µL (4,000-11,000/µL) with neutrophilia and C-reactive protein (CRP) of 245 mg/L (0-0.5 mg/L), as well as anemia with a profile of chronic disorders. The abdominal x-ray showed abundant gas without signs of intestinal obstruction. An abdominopelvic CT with intravenous contrast was performed (Figure. 1, 2 and 3) in which radiological data compatible with a new episode of diverticulitis were observed, as well as an abscess on the lower surface of the sigmoid.
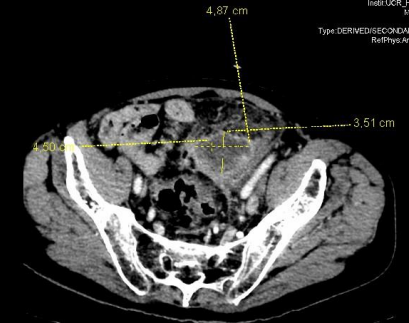
Figure 1: Transverse section of abdominopelvic CT, with abscess measuring 4'87x3'51cm
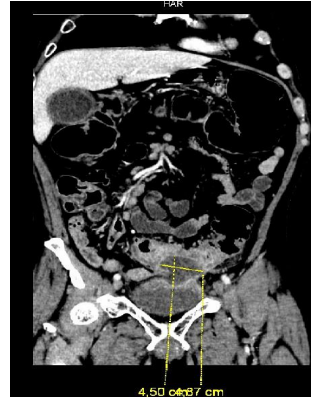
Figure 2: Coronal section of abdominopelvic CT, with abscess measuring 4.5 x 4.87 cm
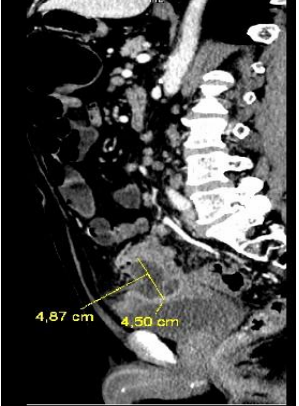
Figure 3: Sagittal section of abdominopelvic CT, with abscess measuring 4.87 x 4.5 cm
In addition, multiple pathologically sized lymphadenopathy, already present in the previous study, was observed on CT. Pathology results from outpatient colonoscopy showed CD10-positive tumor cells.
Evolution:
Despite parenteral antibiotic therapy (piperacillin/tazobactam), a poor clinical, analytical and radiological evolution was observed, with growth of the abdominal abscess, for which surgical treatment by open sigmoidectomy with terminal colostomy was indicated. The study of the surgical specimen confirmed the presence of numerous diverticula with acute leukocyte and histiocytic infiltrate, leukocyte accumulations in the intestinal wall with abscessed areas. In addition, an extensive neoplastic proliferation of lymphoid habit was observed that formed nodules with a focal tendency to fusion, and that appeared transmurally in the intestinal wall and in the subserous adipose tissue, as well as in the 19 isolated lymph nodes. These neoplastic follicles were formed by a mixture of small and intermediate sized lymphocytes (centrocyte type) with others of larger size and centroblast morphology, accounting for <15>
The extension study (cervico-thoracic CT) revealed subcentimeter lymph nodes in the right supraclavicular region, upper abdomen, lower mesenteric chain, ileocolic and in the retroperitoneum. The bone marrow aspirate and biopsy detected a minority clonal B population compatible with follicular lymphoma.
The first cycle of chemotherapy with Rituximab-Bendamustine was started. In the second cycle, the patient presented fever, diarrhea and elevated reactants that resolved with parenteral antibiotic therapy, as well as a red eye compatible with CMV chorioretinitis (bendamustine was suspended) that responded to treatment with ganciclovir and prednisone. Subsequently, rituximab was administered bimonthly for two years, with complete metabolic remission persisting on Positron Emission Tomography (PET-CT).
PARAMETER Age Stadium Hb level DHL level No. affected lymph node area | ADVERSE FACTOR >60 years III or IV* <12> >AI upper normal limit >4
| ||
Risk Category
Low Intermediate high | Nº. Prognostic Factors
0-1 2-3 4-5 | Survival % 5 years 10 years 91 71 78 51 52 36 | |
Table 1: FLIPI scale. International Index for Follicular Lymphomas.
In patients in stage I, the curative treatment is radiotherapy. In asymptomatic patients with low tumor burden, regardless of stage (II, III, IV), close observation (watchful waiting) can be performed, postponing active treatment at the onset of symptoms or if the disease progresses (3,4).
In our patient, disease progression was observed, with greater lymph node and colonic involvement in the second abdominal CT. Furthermore, he had a FLIPI 4 (high risk category) so treatment with rituximab and bendamustine was started (5).
Other treatment options are:
1.- Rituximab as monotherapy, used in our patient after the first two cycles of combined therapy due to the appearance of relevant infectious complications.
2.- R-CHOP (cyclophosphamide, doxirubicin, vincristine, prednisone and rituximab), which becomes the second choice due to a greater number of adverse reactions (6).
3.- Targeted therapy with a kinase inhibitor, monoclonal antibody or lenalidomide. 4.- Immunotherapy with CAR T Cells, is an option for patients with multiple falls. Because most patients with relapsed FL have favorable outcomes with other, less toxic treatment options, CAR-T therapy is generally reserved for patients with multiple relapses with short durations of prior remission (e.g., <24>
5.- Bone marrow/stem cell transplant.
Highlights:
Colon follicular lymphoma is a very low prevalence process and can simulate or be associated with inflammatory/infectious intestinal pathology. However, the presence of multiple intra-abdominal lymphadenopathy strongly supports its diagnosis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
