
Research Article | DOI: https://doi.org/10.31579/2641-0419/478
Cardiology Department, CHU Ignace Deen, Conakry.
*Corresponding Author: Baldé E.Y, Cardiology Department, CHU Ignace Deen, Conakry.
Citation: Baldé E.Y, Barry I.S, Bah M.B.M, Bah A.M, Camara O.M, et al.,(2025), Acute Coronary Syndromes in Subjects Under 40 Years of Age at the Chu Ignace Deen in Conakry, J Clinical Cardiology and Cardiovascular Interventions, 8(8); DOI: 10.31579/2641-0419/478
Copyright: © 2025, Baldé E.Y. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 12 May 2025 | Accepted: 28 May 2025 | Published: 04 June 2025
Keywords: acs; young subject under 40; chu ignace deen
Introduction: Acute coronary syndromes (ACS) are more common patients over 50. Nowadays, however, it is not uncommon to see them in younger patients.
Patients and Methods: This was a descriptive, retrospective study lasting one year (from January 1, 2023 to December 31, 2023) and concerned subjects aged under 40 years hospitalized in cardiology at Ignace Deen University Hospital. The aim of the study was to describe the epidemiological, clinical and therapeutic aspects of ACS in young subjects under 40.
Results: Of a total of 608 patients, 170 (28%) were ACS patients, of whom 23 (13.5%) were under 40 years of age. The mean age of our patients was 31± 6.8 years, with extremes of 19 and 39 years. The male/female sex ratio was 4.75. The majority had no insurance (78.26%). Dyslipidemia, hypertension and smoking were the main modifiable risk factors, with 56.52%, 17.39% and 8.69% respectively.
Chest pain was the main symptom in all patients (100%). ST+ accounted for 73.91% and non-ST+ for 26.09%. Seven (7) patients were within the time limit for thrombolysis (30.43%). Coronary angiography was performed in 3 patients (13.04%). Heart failure was noted in 4 patients (17.39%), with a mortality of 4.34%.
Conclusion: ACS in young patients is common at Ignace Deen University Hospital. Coronary angioplasty is not accessible to all, resulting in high in-hospital mortality.
Coronary syndromes were considered rare before the age of 40, but in recent years their incidence has risen sharply, constituting a remarkable economic challenge (1). Cardiovascular disease, and more particularly ischemic heart disease, is constantly on the increase in both developed and developing countries (2). According to Diop C et al., 17.9 million deaths worldwide are due to cardiovascular pathologies. Of these, 7.4 million are due to heart disease.
Ischemic events (3). Acute coronary syndrome (ACS) is defined as de novo, prolonged or recently worsening angina-like chest pain in a patient with or without a history of coronary artery disease. As such, MI is an absolute cardiological emergency, the incidence of which remains high at 120,000 cases per year in France (4). Myocardial infarction (MI) in young people is rare, accounting for 4-10% of MI cases of all ages, but its incidence is rising and represents an indisputable economic challenge. It represents the most frequent manifestation of atheromatous disease at this age, and can also be linked to other causes such as haemostasis anomalies or coronary spasm (5). In Senegal, one study reported a hospital prevalence of 21.31% (6).
In Guinea, the hospital prevalence of myocardial infarction in young people under 50 is 23% (8).
This was a descriptive, retrospective one-year study (January 1, 2023 to December 31, 2023) conducted in the cardiology department of the Ignace Deen University Hospital. All patients under 40 years of age admitted for acute coronary syndrome on the basis of angina syndrome, rest pain, suggestive electrocardiographic changes and elevated troponin levels were included. Patients with less than 40 years of age, those stable syndrome, pain at rest, suggestive electrocardiographic changes and elevated troponin levels were included. Patients over 40, those stable angina and those semi-sequential or sequential coronary syndrome were excluded from the study.
We studied data on age, sex, history, including history of diabetes, hypertension, smoking, alcoholism, sedentary lifestyle (less than 30 minutes or more of moderate-intensity physical activity most days of the week), obesity; family history of coronary heart disease at an early age under 40, use of estrogen-progestogen contraceptives, stable angina pectoris and stress. We also noted the time admission, the management given and vital parameters (blood pressure, heart rate, body mass index).
Other tests included blood glucose levels on admission, total cholesterol, HDL, LDL and triglycerides. On ECG, we looked for subepicardial or subendocardial lesions. Cardiac echodoppler assessed LV systolic function, segmental and global kinetics, and looked for left intra-cavity thrombi. Coronary angiography looked for coronary stenosis. Data analysis and entry were performed using Épi infos software version 7.2.0 and Office Word, Excel 2016. The anonymity and confidentiality of all patients were respected
Of a total of 608 patients, 170 (28%) (Figure 1) were ACS patients, of whom 23 (13.5%) were under 40 years of age (figure 2). The mean age of our patients was 31± 6.8 years, with extremes of 19 and 39 years (table I). The male/female sex ratio was 4.75 (table I). The majority had no insurance (78.26%) (table II). Dyslipidemia, hypertension and smoking were the main modifiable risk factors, with 56.52%, 17.39% and 8.69% respectively. Chest pain was the main symptom in all patients (100%) (table III).
ST+ accounted for 73.91% and non-ST+ for 26.09% (Figure 3). Seven (7) patients were within the time limit for thrombolysis (30.43%) (table V). Coronary angiography was performed in 3 patients (13.04%) (table VI). Heart failure was noted in 4 patients (17.39%), with a mortality of 4.34% (tableVII).

Figure1: Flow chart for inclusions.

Figure2: Prevalence of ACS in young people under 40.
| Features | Workforce | Percentage |
| Age (years) | ||
| 19-24 | 4 | 17,39 |
| 24-29 | 4 | 17,39 |
| 29-34 | 4 | 17,79 |
| 34-39 | 8 | 34,78 |
| ≤ 39 | 3 | 13,04 |
| Average And [extremes] | 31.8± 6.8 | [19 - 39] |
Gender Male |
19 |
83 |
| Female | 4 | 17 |
| Ratio(M/F) | 4,75 |
Table I: Distribution of patients by socio-demographic characteristics
| Care method | Frequency | Percentage |
| Personal resources | 18 | 78,26 |
| Health insurance | 3 | 13,04 |
| No | 2 | 8,70 |
| TOTAL | 23 | 100 |
Table II: Distribution of patients by mode of care
| Clinics | Workforce | Percentage |
Reasons for consultation Chest pain |
23 |
100 |
| Dyspnea | 4 | 17,39 |
FDRCV Dyslipidemia |
13 |
56,52 |
| HTA | 4 | 17,39 |
| Tobacco | 2 | 8,69 |
Table III: Distribution of patientsby clinical characteristics and modifiable risk factors
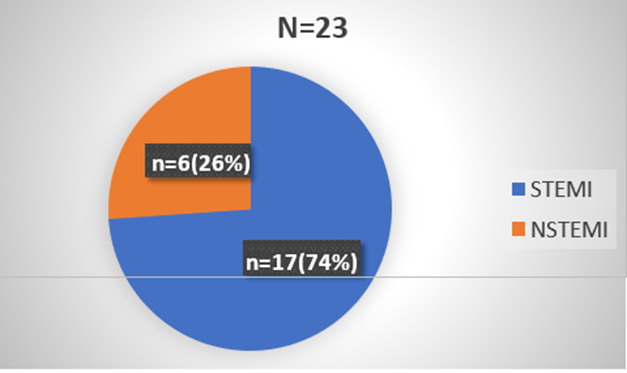
Figure 3: Patient distribution by ECG
| Onset of pain | Workforce | Percentage |
| ≤ 6H | 3 | 13,04 |
| 6-12H | 4 | 17,39 |
| ≥ 12H | 16 | 69,57 |
| Total | 23 | 100 |
Table V: Distribution of patients according to time to treatment.
| Treatment | Frequency | Percentage |
| Clopidogrel | 17 | 73,91 |
| Aspirin | 16 | 69,57 |
| IEC | 15 | 65,22 |
| Analgesic | 15 | 65,22 |
| B Blocking | 14 | 60,87 |
| Statins | 13 | 56,52 |
| Heparins | 13 | 56,52 |
| Anxiolytic | 2 | 8,69 |
| Nitro derivatives | 2 | 8,69 |
| Angioplasty | 3 | 13,04 |
| Thrombolysis | 7 | 30 ,43 |
Table VI: Distribution of patients accordingto treatment.
| Evolution | Workforce | Percentage |
| Favorable | 19 | 82,60 |
| Unfavorable | ||
| Heart failure | 3 | 13,04 |
| Deceased | 1 | 4,34 |
| Total | 23 | 100 |
Table VII: Distribution of patientsaccording to evolution
Over a 12-month period, only 23 cases were collected. Only patients presenting ACS were included in our study; patients hospitalized for ischemic heart disease and other pathologies were excluded.
When the files were analysed, the questioning data concerning FRCV were incomplete: only smoking, hypertension and dyslipidemia were listed, with no indication of how long they had been present. On physical examination, anthropometric parameters such as body mass index (BMI) and waist circumference were missing from most files.
Coronary angiography was not performed in all patients.
The doses of the drugs were not mentioned .
The evolution after hospitalization has not been studied in all patients.
The majority of published studies on young MI patients are single-center studies of different types of ACS patients, or populations from randomized trials. Very few studies have made gender comparisons (9).
The rising incidence of cardiovascular disease is expected to continue, not only because of the increasing prevalence of obesity, diabetes and metabolic syndrome, but also because of the aging of the population (10). Our study includes all patients under 40 years of age managed for ACS at the cardiology department of CHU Ignace Deen from January 1 to December 31, 2023. seventy (170) coronary patients, twenty-three (23) of whom met our inclusion criteria, representing a prevalence of 13.53%. Our result is lower than that found by MINGOU J et al (11), but higher than those of Juan A. Fournier et al; Coulibaly S et al; Sarr M et al who reported respectively 4.1%; 6.8% and 6.8% (11,12). HERMAN Y reported a prevalence of acute coronary syndrome of 76% (13).
The mean age of our patients was 31± 6.8 years, with extremes of 19 and 39 years. Our patients were relatively younger than those of Bâ Hamadou et al, with a mean age of 34.14±
2.96 years and extremes of 29 and 37 years (2). The age most affected was 34-39, at 34.78%.
According to sex, men were the most represented at 83%, our result corroborates that found by Coulibaly S et al in Mali, who found 90% of men (12).
The majority no insurance (78.26%). This can be explained by the fact that the population has a very low socio-economic level.
According to FDRCV, dyslipidemia was the most prevalent with a frequency of 56.52%. This result is contrary to those of Raiah M et al who found a predominance of hypertension (41.5%) (13). Fach A et al found 27.1% dyslipidemia, a much lower figure than ours(14).
All patients (100%) had chest pain. These results are similar to those of Sarr M et al who found 95.2% and 70% respectively in their series (11).
The electrocardiogram revealed acute coronary syndrome with persistent ST-segment elevation in 17 patients (73.91%) and acute coronary syndrome without ST-segment elevation in 6 patients (26.09%). Our results are lower for STEMI but higher for NSTEMI than those of Sarr M et al, who reported 85.7% and 14.3% respectively (11).
69.57% of our patients were admitted out of time (≥ 12H), our result is close to those found by Coulibaly S et al. (12) in Mali in 2018 and Pessinaba. et al. (17) in Togo in 2018 who reported respectively an average delay of 84.2 h and 82.1 h. These results can be explained by the lack information about ACS in the general population and among general practitioners and other specialties.
In contrast to the DAGNOGO et al study, 17.39% had been thrombolysed with Streptokinase. This may be explained by the fact that their patients were all admitted to the cardiac catheterization room within a short timeframe. 66.67% had been loaded on admission Aspirin and clopidogrel.
In line with recommendations (19), most of our patients were on dual anti-platelet aggregation therapy (clopidogrel and aspirin), i.e. 73.91% and 69.57% respectively.
Only 3 patients (13.04%) had undergone coronary angiography with a monotruncal lesion (diagonal occlusion). In several series, this predominance of monotruncular lesions was found Bâ H et al found monotruncular lesions in 34%. (2)
Killip stage II heart failure was the most common complication, accounting for 13.04%. It would appear to be the most frequent complication of ACS.
Progression was favourable in 82.60% of our patients. Our result was superior to that found by Mboup MC. et al (18).
CONCLUSION: Younger accounted for 13.5% of those consulted for ACS. Dyslipidemia was the main FDRCV. Most of our patients were received late (>12h).
Most of our patients had a favourable outcome. Management of ACS remains a major problem in Guinea. It should be improved through primary prevention, screening and management of FDRCV, awareness-raising and information for the general population and medical personnel.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
