
Case Report | DOI: https://doi.org/10.31579/2690-4861/211
1 Department of Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia.
2 King Khalid Hospital, Alkharj city, Riyadh Region, Ministry of Health, Saudi Arabia.
3 Ministry of Health, Riyadh, Saudi Arabia.
*Corresponding Author: Bandar Ali M.D, Department of Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia.
Citation: Ali B, Al-Hassan B, Alshihri A, Alanazi M, Sultan T Almatrafi, Bukhari K. (2022). Acute Acalculous Cholecystitis in a Patient with Systemic Lupus Erythematous Case Report. International Journal of Clinical Case Reports and Reviews. 11(1); DOI: 10.31579/2690-4861/211
Copyright: © 2022 Bandar Ali, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 08 March 2022 | Accepted: 22 March 2022 | Published: 26 March 2022
Keywords: acute acalculous cholecystitis; systemic lupus erythematous; abdominal pain; gallbladder; acute abdomen; cholecystectomy
Acute Acalculous Cholecystitis “AAC” is defined by inflammation of the gallbladder without the presence of gallstones. It is by far less common than acute calculous cholecystitis where it only counts 5-10% of all cases of acute cholecystitis. In a patient with the disease of systemic lupus erythematous (SLE) having a gallbladder disorder is not common. Herein, we present a 43-year- old lady who is known case of hypertension, SLE, and End-stage renal disease on hemodialysis due to lupus nephritis presented to the emergency department with a right upper abdominal pain, and abdominal ultrasound revealed acalcular cholecystitis. Further diagnostic tools supported the diagnosis, and she underwent after preparation uneventful laparoscopic cholecystectomy (LC).
Acute Acalculous Cholecystitis (AAC) is defined by inflammation of the gallbladder without the presence of gallstones. it's by far less common than acute calculous cholecystitis where it only counts 5-10% of all cases of acute cholecystitis [1].
AAC pathogenesis is complex and multifactorial, where patients who are diagnosed with AAC are usually critically ill, intubated, and intensive care unit (ICU) patients [1].
In systemic lupus erythematous (SLE) patients, gastrointestinal tract involvement is present in around 30% of SLE patients, but AAC is considered a very rare disease in those patients, where most of them are already known to have SLE and it is not their first presentation of SLE [2,3].
This is a 43-year-old lady known case of hypertension, SLE, and End-stage renal disease (ESRD) on hemodialysis due to lupus nephritis. She presented to the emergency department (ED) complaining of right upper quadrant pain radiating to the back. The pain started two days back, was persistent, colicky in nature, and associated with nausea and vomiting. No history of fever, change in bowel habits or change in stool or urine color. The patient has had no similar attacks previously.
The patient was diagnosed around 20 years back with SLE world health organization (WHO) class III based on positive anti-nuclear antibodies (ANA), double-strand deoxyribonucleic acid (dsDNA), low complement (C3), and low complement (C4). She was diagnosed with end-stage renal disease eight months back and started on hemodialysis (HD). The patient was not compliant with her medication.
On physical examination, the patient was conscious, alert, and oriented. Blood pressure (BP) 135/75 mmHg, heart rate is 95 beats per minute, respiratory rate is 20 per minute, the temperature is 36.8 Celsius and SPO2 98% on room air. The patient was not jaundiced, and her chest was clear and equal bilateral air entry.
The abdomen was soft and lax, with marked tenderness in the right upper quadrant with a positive Murphy’s sign.
Laboratory tests revealed white blood cells 3.37, hemoglobin 7.1 g/dl, sodium 136mmol/l, potassium 4mmol/l, creatinine 563mmol/l, urea 8.4, total bilirubin 5mmol/l, direct bilirubin 1.5, and Alkaline phosphatase 102.
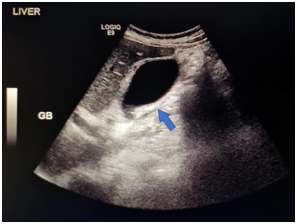
Ultrasound (U/S): Normally distended Gallbladder (GB) with mild diffuse wall thickening 0.38cm associated with hyperemia. There is a trace of pericholecystic fluids, no gallbladder stones. Positive radiological murphy sign Figure 1.
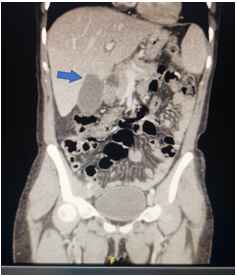
Computed tomography (CT) showed gallbladder distention with preserved mucosal delineation and enhancement associated with peri-cholecystic fluids suggestive of acute cholecystitis.
The common bile duct (CBD) was dilated 0.9 cm with no obvious obstructing stone Figure 2,3.

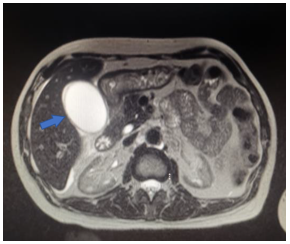
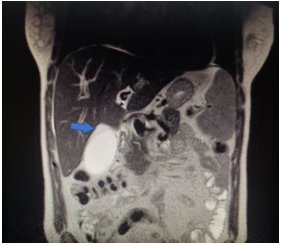
Magnetic resonance cholangiopancreatography (MRCP): Gallbladder is distended with a small amount of peri-cholecystic fluid, no gallbladder stones or wall thickening. CBD is dilated 0.7cm with no stones or strictures, minimal proximal intrahepatic biliary duct dilatation measuring 0.4cm there are few porta hepatis reactive lymph nodes. Findings are suggestive of resolving acute cholecystitis Figure 4,5.
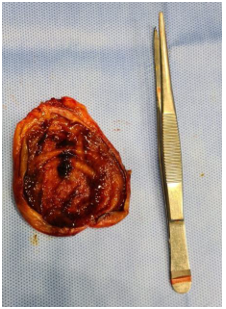
Initially, the patient was started on conservative management where she was kept nill per Os (NPO), with intravenous fluids and antibiotics “cefuroxime and metronidazole”, until all investigations were done then she underwent laparoscopic cholecystectomy. Inspecting the specimen showed no gallbladder stones Figure 6.
The patient post-operatively was doing fine and was discharged 1 day after the procedure.
AAC is a serious disease with a high mortality rate that needs to be diagnosed and treated early. There are many pathogeneses of AAC, such as gallbladder ischemia-reperfusion Injury, cholestasis, Bacterial Infections, Abnormal Anatomical Structure of the biliary tract system, and other risk factors as hypertension, atherosclerosis diabetes mellitus, vasculitis, and immunodeficiencies such as SLE [1,3].
SLE is an autoimmune disease that causes chronic inflammation virtually affecting any organ in the body, with many clinical manifestations mainly as vasculitis [4,7]. In SLE the gastrointestinal tract symptoms are very common, however, AAC associated with SLE is considered very rare, especially as an initial presentation of SLE with an incidence rate less than 0.05% [7].
As the pathogenesis of AAC in SLE patients, there are multiple suggested theories such as serositis, vasculitis, mesenteric inflammatory veno-occlusive disease, and antiphospholipid syndrome, being vasculitis is the most common cause of AAC in SLE patients [5,6].
Until now there is no full agreement regarding the treatment of AAC in SLE patients. Suggested treatment options are Cholecystectomy, cholecystostomy tube, and conservative medical treatment in the form of corticosteroids, Hydroxychloroquine, and antibiotics. It depends on the patient's general condition and the risk factors that the patient has, whether they can tolerate the surgical procedure or not [4,7].
As our patient was in a good state of health, not septic and young, she underwent laparoscopic cholecystectomy. Post-operatively she stayed one more day for observation then she was discharged in a good condition.
In many studies where the patient couldn't tolerate the surgical intervention conservative medical management was the choice where high doses of corticosteroid and antibiotics were given to the patients which showed successful modality of treatment [4,8].
AAC in SLE patients is a rare disease but it could be a life-threatening situation. Diagnosis and management should not be delayed. Surgical intervention for these patients who can tolerate the surgical procedure is a valid option, although in patients who can't tolerate surgery, they should be treated by other medical options. We recommend that those patients to be assessed and discussed with a multidisciplinary team to determine the best management can be offered for them.
Conflict of Interest
The authors declare no conflict of interest
Funding
Self-funded by the authors
Declare
Non
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
