
Case report | DOI: https://doi.org/10.31579/2578-8949/145
1 Postgraduate doctor of second year of dermatology UTE university – Ecuador
2 Attending physician in dermatology, Eugenio Espejo Specialty Hospital - Ecuador.
3 Rural doctor at La Huaca Health Subcenter – Ecuador.
4 Attending physician in dermatology, Eugenio Espejo Specialty Hospital – Ecuador
*Corresponding Author: Carla Verdugo M, Postgraduate doctor of second year of dermatology UTE university – Ecuador.
Citation: Carla Verdugo M, Yadira Aguilar B, Gladys Castillo S, Francisco Mejía, Maria Victoria Santofimio D (2024), Actinic Reticuloid: A Literature Review of a Case, Dermatology and Dermatitis, 10(2); DOI:10.31579/2578-8949/145
Copyright: © 2024, Carla Verdugo M. This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 January 2024 | Accepted: 31 January 2024 | Published: 08 February 2024
Keywords: actinic reticuloid; inflammatory; corticosteroids; posterior thorax
Actinic reticuloid is a chronic inflammatory skin condition that primarily affects elderly individuals and is associated with chronic sun exposure. It is characterized by the presence of papules, plaques, and fine lines that form a reticular pattern on sun-exposed areas, such as the face, neck, and extremities. Histologically, lichenification and dermal alterations are observed, suggesting a chronic response to sun exposure.
Actinic reticuloid is often diagnosed clinically, but confirmation may require a skin biopsy. Managing this condition involves measures to protect the skin from the sun, such as the use of sunscreens and protective clothing. Topical and systemic treatments, such as corticosteroids and ultraviolet light therapy, may also be beneficial in some cases.
Although the actinic reticuloid is not malignant, its chronic course and the aesthetic changes it produces can have a significant impact on patients' quality of life. Therefore, it is important for doctors to properly recognize and manage this condition in order to provide effective relief to affected patients.
Actinic reticulium was first described in 1969 as an entity caused by a strong sensitivity to a broad spectrum of radiation. It is classified as pseudo-T-cell lymphomas due to its clinical and histological similarity, however, it is a chronic photodermatosis, which mainly affects older adults, men. Clinically, it is characterized by eczematous lesions located in photoexposed areas, which can extend to covered areas and evolve into infiltrated and lichenified plaques. It is a rare and described entity [1,2].
A 69-year-old male patient, born and residing in La Paz, province of Carchi, divorced, farmer, with a history of epilepsy under management with valproic acid and hypothyroidism under treatment with levothyroxine, denies allergies. She went to the dermatology service for presenting intensely itchy erythematous lesions on the face and neck of several years of evolution, which had previously been treated with topical medication which she did not remember, without improvement and have progressively expanded.
Physical examination revealed dermatosis located in photoexposed areas: face, ears, neck, V of the décolleté and upper third of the anterior and posterior thorax, characterized by erythematous plaques with thick desquamation, infiltrated and lichenified, superficial abrasions and some with crusts. (Figure 1Y2)

Figures 1 and 2
In the review of devices and systems, no other significant alterations were evidenced.
Complementary examinations showed 6.22 leukocytes, 60.8% neutrophils, 26.4% lymphocytes, 10.10% and 0.80% eosinophils; hemoglobin 16.3, hematocrit 47.8, platelets 282,000, glucose 78.6, urea 19.5, creatinine 0.70, total bilirubin 0.44, cholesterol 146, triglycerides 86.70, TGO 12.20, TGP 16.30, GGT 12, EMO: negative.
In view of the clinical suspicion, two skin biopsies were performed, the first in the right frontal region (Figure 3) and the other in the anterior thorax (Figure 4), which reported acanthosis, parakeratosis, spongiosis and vacuolization of the basal artery; In the papillary and middle dermis, moderate perivascular lymphocyte inflammatory infiltrate, some atypical with mild epidertrophism, is accompanied by eosinophils, plasma cells and hemosiderophages, presence of collagen bands parallel to the epidermis.
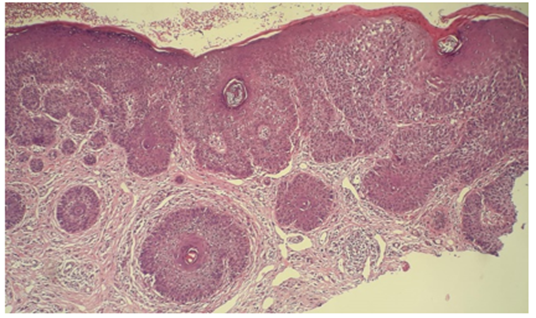
Figure 3
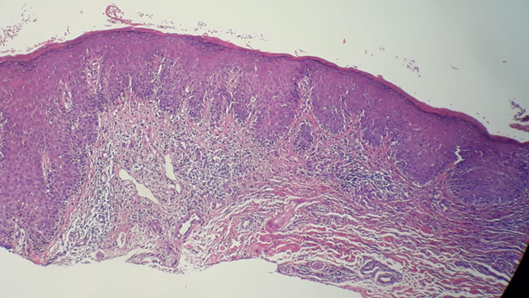
Figure 4
Immunohistochemistry: CD8: Positive for T lymphocytes (Figure 5). CD4: Negative (Figure 6)
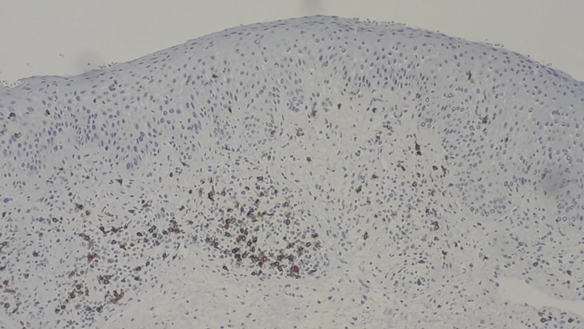
Figure 5
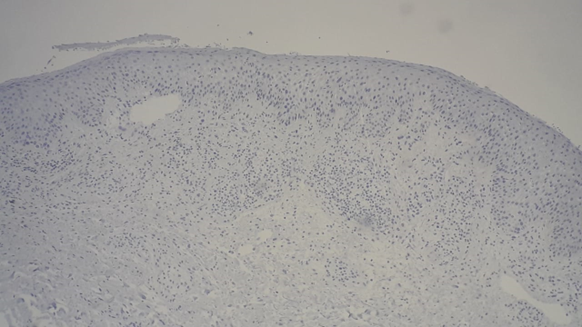
Figure 6
The patient was initially treated with systemic corticosteroids, prednisone at a dose of 60 milligrams/day with a progressive decrease in the dose with an adequate response, in addition, topicals, emollients and antihistamines were used to control pruritus, in the first control at 15 days there was evidence of a decrease in lesions, erythema and desquamation (Figures 7 and 8), in addition, the patient reported control of pruritus. however, the patient showed poor adherence to treatment and did not comply with subsequent appointments.

Figures 7 and 8</>< class>
| TABLE 1. Acquired idiopathic photodermatoses |
|
Its pathophysiology is not entirely clear and is not well defined, however, different factors are suggested. In 75% of patients who develop this pathology, a history of contact dermatitis or other photoallergic dermatitis was identified due to multiple allergens involved, such as histidine, plant resins and fragrances. An increased susceptibility to mainly UVB rays is also identified, demonstrated in a decrease in the dose of minimal erythema (MED).(3)
Another accepted hypothesis is that it is a type IV delayed hypersensitivity response that responds to a photo-induced antigen. The allergen is covalently bound to an endogenous protein by a covalent bond and requires the involvement of UV radiation. The changes produced mean that the presence of hapten is not necessary and only requires the action of UV rays to trigger a response. (4)
Clinic
A medical history is essential as there is often a history of intense photoexposure during the last few years. Clinical findings usually follow an evolutionary course. In the early stage it is common to observe eczematous lesions and erythroderma in areas exposed to the sun, the sign of "clothed erythroderma" is observed since when the clothing is removed it is observed that in covered areas there is no affectation. With the passage of time, lichenified and infiltrated plaques appear with papules and nodules that can extend to covered areas and also give the face a leonine facie and in the last stage generalized erythroderma may exist. (3)(5)
They may be accompanied by other signs, mainly intense itching, generalized lymphadenopathy, onychodystrophy, and diffuse alopecia.
Histology
It will depend on when the biopsy is done.
In the first or acute stage, a pattern of eczematous dermatitis is observed: spongiosis, acanthosis, for focal keratoses and perivascular lymphocyte infiltrates in the papillary dermis
In an advanced stage, it is more similar to a cutaneous T-cell lymphoma, with a dense band infiltrate in the papillary and middle dermis, there is also a perivascular and periadnexal infiltrate, which can be made up of normal or atypical lymphocytes, with convoluted nuclei and epidermopism that form, in some cases, Pautrier's microabscesses. (6)
There are other supporting techniques such as immunohistochemistry where a predominance of CD8 positive is distinguished in relation to mycosis fungoides that predominate C4, the genotype with PCR, are necessary to differentiate this picture from cutaneous T-cell lymphomas. (5)
Diagnosis
In 1991, Toonstra proposed 3 criteria for its diagnosis (7)
Although it is not within the diagnostic criteria, the patch test should be considered given its close relationship with allergic contact dermatitis and laboratory tests that include blood count, erythrocyte sedimentation rate and porphyrin dosage given its similarity if it is to be ruled out.
Treatment
The first and most important measure is to avoid triggers: light and photoallergens, during the acute phases these measures should be strict. Sunscreens are useful, but they should be monitored for their photosensitizing potential.
The use of corticosteroids is effective, they will be used depending on the clinic, they can be topical or systemic (prednisone 15 to 30 mg/day) which can be used in short periods or in periods of exacerbation. Another good topical alternative is tacrolimus 0.1% with good response and few adverse effects. (8)(9)
Sometimes the oral use of immunosuppressants is required, as a first alternative is azathioprine at doses of 1-2.5 mg/kg/day, evidencing an improvement one month after administration, however, its side effects such as myelosuppression limit its use. (10)
Cyclosporine at doses of 3-5 mg/kg/day induces a relatively rapid improvement, however, it has been seen that when treatment is discontinued there is recurrence of the lesions, so it is not possible to (11)There is sufficient evidence to support its use as well as that of mycophenolate mofetil, hydroxyurea and interferon alfa.
Finally, ultraviolet (UVB) treatments increase light tolerance.
Actinic reticulium is a chronic photodermatosis framed within the T-cell pseudolymphomas, mainly affecting men, in the fifth and sixth decade of life its clinical picture is variable depending on the stage in which it is, it begins with eczematous lesions in photoexposed areas and progresses to plaques in covered areas can cause generalized erythroderma, its pathophysiology is not well defined, however, UVB radiation is the main culprit. The fundamental pillar in its management is sun protection, frequently requiring the use of systemic medication with an adequate response to corticosteroids, sometimes it may require other therapies. Although it is not life-threatening and there are no reports of malignancy, it does affect the quality of life and daily activities, so it is essential to diagnose and treat it in a timely manner.
The authors declare no conflict of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
