
Research Article | DOI: https://doi.org/10.31579/2692-9759/002
Electrophysiologist Head of Electrophysiology Department at St. Sophia State HospitalManizales, CaldasColombia South America
*Corresponding Author: William-Fernando Bautista-Vargas, Electrophysiologist Head of Electrophysiology Department at St.Sophia State Hospital Manizales,CaldasColombia South America
Citation: William-Fernando Bautista-Vargas, (2020) A Wolff- Parkinson- White Surprise Case. J Cardiology Research and Reports, 2(1): Doi: 10.31579/2692-9759/002
Copyright: © 2020, William-Fernando Bautista-Vargas, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 November 2019 | Accepted: 18 December 2019 | Published: 10 January 2020
Keywords: syncope, wolff-parkinson-white syndrome, catheter ablation
37-year-old-gentleman, who was presented in three occasional times to emergency department for a fast, precordial, and rhythmic symptomatic palpitations, in which the last episode was with a duration that lasted more than an hour with instability vitally that ended in performing emergency electrical cardioversion. All these episodes were symptomatic and last hospitalization was associated with pre syncopal and syncopal attacks.
With evidence of Wolff-Parkinson-White syndrome the patient was brought to Electrophysiology Lab to EP study and ablation.
So often we found an ECG with Wolff- Parkinson- White pattern and some of them have an atypical delta wave morphology, and then there are not easy to figurate out the anatomical ubication of the accessory pathway, therefore even with the ECG patterns that are easily to predict where will become the accessory pathway, the real problem is: which ones of them are related with sudden cardiac death risk?. We have some probed clues of low risk: first of all the absence of atrial fibrillation on the ECG records, second the loss of preexisted conduction during the stress test, and the last but not less important the refractory period of AP during EP study specially when it is more than 300ms are signals of low cardiac risk. However the evidence is not clear when we have anatomical abnormalities related with WPW like CS aneurysm [1].
History of presentation
A 37- year-old gentleman, who is not known to have any medical illness, was presented with history of five years of precordial, fast, rapid, palpitations; some of these episodes needed to be admitted to emergency department. Last hospitalization patient had fast symptomatic palpitation with pre syncopal attack, with instability vitally that had to have an immediate successful electrical cardioversion, and admitted to ICU.
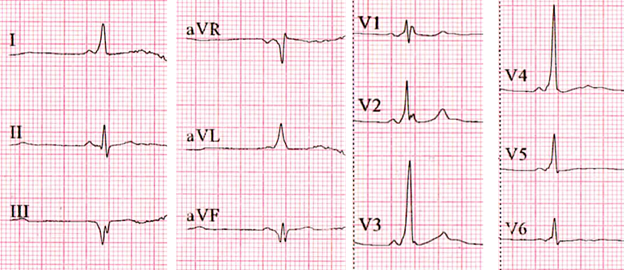
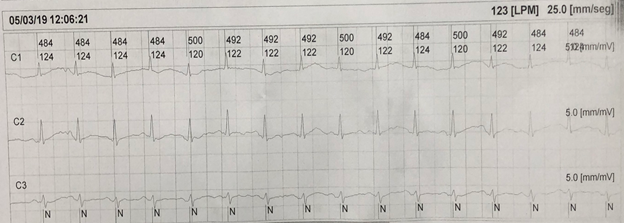
His ECG showed short PR interval with delta wave, this was positive at DI, negative at DIII, aVF and iso-biphasic DII (figure1).
He had a normal echocardiogram with no regional motion abnormalities and normal LVEF without any structural heart disease and normal blood work.
On the next day of admission, the patient was transferred to electrophysiology lab, to perform 3D mapping and radiofrequency ablation.
Under general anesthesia, the catheters were placed at CS, His, RV-apex, ICE and ablation catheter TactiCathTM was advanced over long sheath (SR0™), and used to do anatomical mapping.
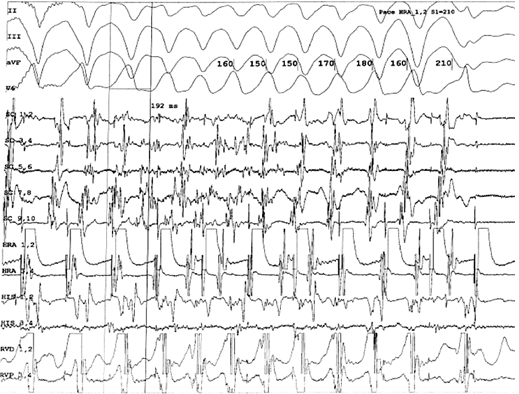
The EP study was performed, with basic intervals were: AH: 97ms, HV interval: 13ms, the antegrade refractory period of AP was less than: 600-220ms, the retrograde refractory period of AP was: 600-300ms, during AF the shortest RR was 192ms (figure2).
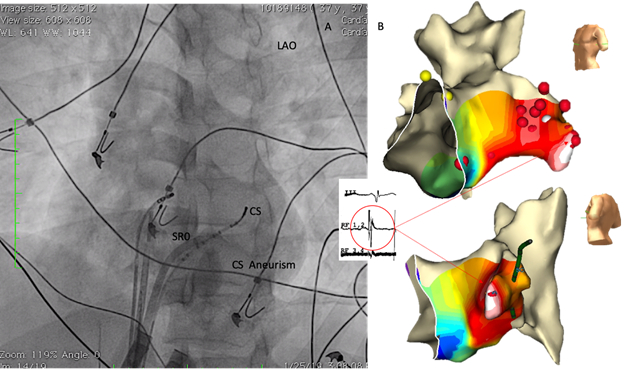
During difficult Kent potential mapping with 3d mapping system (EnSiteTM, St. Jude MedicalTM) we had discover a CS aneurism (Figure3).
And the ablation was performed with (20 Watts and 42c up to 60 seconds) at the apical area of CS aneurism where Kent potential was mapped, with immediate elimination of accessory pathway and normalization the ECG preexcitation pattern (Figure4).

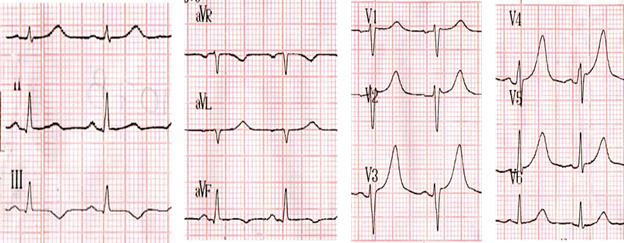
One day post RF. ablation an ECG showed no evidence of preexcitation pattern (Figure5).
The patient was seen and evaluated with 24 hours Holter in the electrophysiology clinic in three month period post RF. ablation with normal ECG and preexcitation pattern(Figure6).
Nowadays the Wolf Parkinson White syndrome (short PR interval, delta wave and tachycardia secondary an accessory pathway conduction) are less presented than before maybe because they were successfully ablated.
Always during the EP study the electrophysiologist has the tools to evaluate the sudden cardiac death related with the abnormal accessory pathway; not only is an electric congenital anomaly but also can be present with anatomical anomalies, the ablation therapy is curative option of treatment to this pathology [2].
Wolf Parkinson White syndrome, was related with sudden cardiac death, however there is no an ECG pattern to do a right prediction, none invasive test like stress test can be useful to evaluate arrhythmia induction and refractory period over AP conduction. The EP study is the invasive strategy to allow the right evaluation of AP risk to sudden cardiac death [2, 3]
The presence of atrial fibrillation is used to evaluate rapid conduction over AP. The shortest RR interval during AF illustrated how fast can be the conduction to the ventricle. The refractory periods were described by Dr. Josephson to evaluate sudden cardiac death risk when these are less than 300ms [4].
Therefore the accessory pathways are more common at left lateral location, the presence of AP at posteroseptal space are up to 8%; 31% of these AP could be found with CS aneurysm as a result the rapid recognition of this anomaly could be a useful information to ablation. There are other venous anomalies reported with posteroseptal AP like left superior vena cava, Ebstein disease [5, 7]
However there is a description of ECG pattern for some CS aneurysm related with posteroseptal AP(QS DIII, aVF and more negative DII ), which is not typically presented as this case. The recognition of CS aneurysm allowed to perform the mapping within the CS aneurysm, nevertheless the ablation site has been described at aneurysm neck, in this case the kent potential was found at the apex of aneurysm where the ablation was performed and with immediate achievement of successful elimination of the accessory pathway [8-12].
CS: coronary sinus
RV: Right ventricle
ICE: intra cardiac echo
EP: electrophysiology
HV: His-Ventricle
AH: Atrium- His
AP: Accessory pathway
AF: Atrial Fibrillation
RR: R wave to R wave interval
ICU: Intensive Coronary Unit
ECG: electrocardiogram
Wolf Parkinson White syndrome can be a challenge pathology, the right evaluation include determination of refractory periods anterograde and retrograde, induction of tachycardia, and atrial fibrillation induction to the aim to determinate if there is a sudden cardiac death risk related.
The posteroseptal accessory pathway can be found related to Coronary Sinus aneurysm, Ebstein disease or left superior cava vein.
The rapid recognition and diagnosis of the venous cardiac anomaly is useful for ablation therapy during EP study.
Learning objectives
The posteroseptal accessory pathways can be difficult to ablate, trickiest cases are some of them who were present with: no succeed previous procedure, no clear Kent potential during mapping. As discussed before where QS at DII reported on the ECG during posteroseptal accessory pathway is a consistent pattern to have high suspicious index of CS aneurism, nevertheless other ECG pattern like the present clinical case can be found with venous cardiac anomalies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
