
Case-Report | DOI: https://doi.org/10.31579/2641-0419/090
1Catheterization Laboratory, Cardio-Thoracic and Vascular Department, University of Pisa
*Corresponding Author: Marco Angelillis, MD, PhD Catheterization laboratory, Cardio-Thoracic and Vascular Department, University of Pisa.
Citation: Marco Angelillis, Andrea Christou, Marco De. Carlo, Cristina Giannini, Laura Stazzoni, Paolo Spontoni, Anna S. Petronio, (2020) A valve-in-valve transcatheter aortic valve implantation with commissural alignment using advanced imaging reconstruction: a case report. J, Clinical Cardiology and Cardiovascular Interventions, 3(9); Doi:10.31579/2641-0419/090
Copyright: © 2020 UA Eyubova, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 30 September 2020 | Accepted: 09 October 2020 | Published: 16 October 2020
Keywords: aortic valve disease; computed tomography; structural valve deterioration.
Transcatheter valve in valve (ViV) implantation actually represents a valid alternative to surgical reinterventions in patients with previous surgical aortic valve replacement (AVR). In patients less than 80 years old, it is crucial to correctly position the new valve leaving a feasible and easy access to coronary ostia, both for future percutaneous coronary intervention (PCI) than for a future possible TAVinTAV procedure. We report a 71 year old man with prior AVR presented with structural valve deterioration (SVD) leading to severe aortic stenosis. In order to guarantee comfortable coronary access we aligned, the commissures of the new percutaneous valve with the ones of the surgical bioprothesis by reconstructing the headframes of the surgical bioprosthesis with computer tomography (CT) and fluoro-CT.
Transcatheter aortic valve implantation (TAVI) has become an recognized therapy for patients with aortic stenosis who are at high or intermediate surgical risk [1]. Recently, TAVI is moving toward treatment for low risk patients, which in many cases are patients with less than 75 years old [2]. Moreover, in the last years, treatment of degenerated surgical bioprostehsis with TAVI (ViV) has emerged as an effective alternative to a redo surgical intervention [1]. When a ViV procedure is performed, a crucial aspect is to avoid coronary occlusion and allow smooth access to the coronary ostia. There are different technique proposed, from the CHIMNEY stent [3]. to the BASILICA technique [4].
When we treat with TAVI a young patient, it is mandatory to ensure a safe coronary access as there is a higher risk to dial with coronary syndromes. To guarantee an easy coronary engagement the best is try to make a commissural alignment during the implant between the native commissural and the TAVI as is performed in surgery.
We report a case of ViV when we perform a commissural alignment.
We report a case of a 71 years old male that, in 2011, for a symptomatic bicuspid aortic stenosis, was treated with surgical aortic valve replacement (AVR) using a Perimount Magna Ease 25 bioprosthesis with a mini-sternotomy approach.
He performed follow up every year until 2019, when a prosthesis structural valve degeneration (SVD) [5], was diagnosed by echocardiographic, without symptoms.
At the beginning of 2020 patient was admitted to emergency room for pulmonary edema, treated with intravenous diuretic. A systolic left ventricular dysfunction was observed with an ejection fraction of 40%. Echocardiographic data confirmed SVD: peak aortic velocity 3.7 m/s, medium gradient 36 mmHg. Patient described also in the previous week angina for minimal effort.
The patient was referred to our department, where he performed coronary angiography, which showed a critical right coronary stenosis, and angio-computed tomography (CT). The case was discussed during the Heart Team and, though young with estimated low surgical risk (STS score was 2.5%), the patient was planned for percutaneous valve-in-valve (ViV) treatment due to extensive calcification of the aortic annulus and risk of a reintervention. A staged percutaneous coronary angioplasty of right coronary was performed through a right radial access. Then, a Corevalve Evolut R 26 was decided particularly for the suprannular valve design that allow obtaining low residual gradient. Moreover, considering the age of patient and his history of coronary disease, the planning of a correct ViV position was decided to be mandatory in order to ensure an easy coronary access for future PCI procedure, and to allow a potential new TAVI procedure.
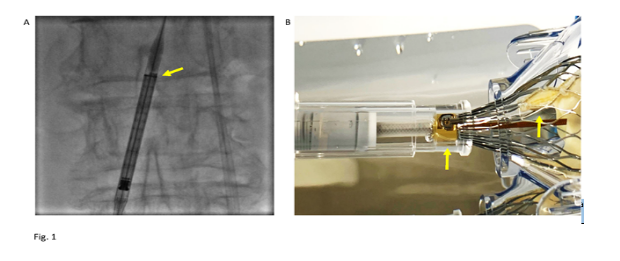
A complete study of relationships between coronary ostium, valve leaflets and the metallic ring of the surgical prosthesis valve was performed using CT. Reconstruction of annulus, coronary ostium and rotation of the surgical valve was done which we marked to be identified with the coplanar fluoroscopic views and CT imaging fusions. Our aim was to obtain commissural alignment between the surgical bioprosthetic valve and the new transcatheter aortic valve. In order to recognize the commissure, Evolut R and Evolut Pro have a radiopaque marker align with the anterior commissure. So, it is possible to rotate the device during the procedure in order to align a the radiopaque marker (Figure. 1-A) to the commissure of the surgical bioprosthesis (Figure. 1-B). After valve deployment, new commissural correspond to the Hat pad (C-tab). Tang et al [6]. Describe as, rotating the device of 90° externally before introducing it, with the flush port facing 3 o’clock (Figure. 3-A), it is possible to obtain alignment of the Hat pad (and consequently of the TAVI’s commissure) to the outer curve (OC) of the aorta during valve deployment. Consequently, placing a marker on the surgical commissure and having it on OC, it is enough to perform the rotation maneuver to obtain commissural alignment (Figure.1-A).
The ViV technique was performed using Corevalve Evolut R n° 26 through a right femoral access; left femoral artery was used as the secondary access. Post dilatation was performed using 25 mm balloon. At the end of the procedure, angiographic and echocardiographic control showed no paravalvular leak. To verify the feasible of coronary access, we engage the left coronary ostium with a diagnostic Judkins 4 left catheter (Figure. 2).

Surgical bioprosthetic aortic valve are implanted with commissure-to-commissure alignment to the native aortic valve. When we perform a ViV procedure, the risk of unsuccessful is mostly due by the TAVI’s commissure in front of the coronary ostium, making coronary engagement for coronary angioplasty or PCI difficult if not impossible. To avoid this, recently some authors have suggested an intra-procedural alignment between TAVI and surgical valve commissures [7,8].
Corevalve Evolut has the anterior C paddle that indicates one of the commissure. This paddle can be identify after valve deployment (Figure. 1). Moreover, the orientation of this paddle can be performed before introducing the valve in the patient, since the radiopaque marker correspond to the “hat marker” visible on the delivery system. Recently, Tang et al [6]. described a significative lower overlap of commissure with left main (15.7% vs. 66.0%, p < 0.001) and right coronary (7.1% vs. 51.1%, p<0.001) when the hat marker stands in the aortic OC (Figure.3-B).

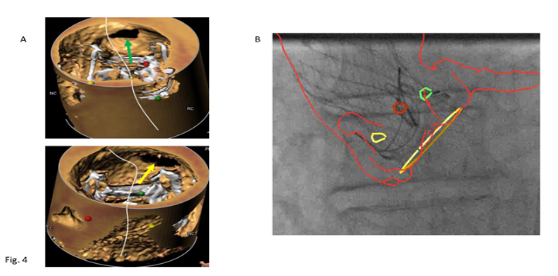
In this case, CT imaging fusion protocol was used to identify both the coronary ostium and their relation with the bioprosthesis metallic frame. For this purpose, we identify with different color each headframe of the valve (Figure.4).
During the procedure, we identified the angiographic projection with the CT reconstruction aligned in a LAO projection (Figure. 4) with the OC of the aorta on the left side where we expected to see the hat marker.
After the deployment, we perform a post-dilatation to reduce residual gradient that was 8 mmHg. Finally, in order to demonstrate that TAVI commissure were in a correct position, we engage with a left diagnostic catheter the left coronary (Figure. 3).
This technique performed with the help of CT fusion is able to guarantee a correct alignment and a coronary percutaneous treatment in the future. Moreover, in younger patients the great challenge is represented by having to perform a TAVI in TAVI procedure for TAVI degeneration. In case series report of TAVI in TAVI degeneration, this is not always free of complications for coronary occlusion (9,10). Moreover, the chance of coronary disease and PCI is higher in younger patients in whom an unsuccessful would be unjustified.
ViV represent a valid alternative to a redo surgical intervention in SVD. In young patients, it is essential to preserve a safe and easy coronary access. To perform this, the new generation of Corevalve allows performing a commissural alignment as in surgery. Advanced 3D CT elaborate images are essential.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
