
Case Report | DOI: https://doi.org/10.31579/2768-2757/079
1 Department of Plastic, Reconstructive and Aesthetic Surgery, Liv Hospital, İstanbul, Turkey
2 Department of Plastic, Reconstructive and Aesthetic Surgery, Private Hospital of Büyükşehir, Konya, Turkey
3 Department of Plastic, Reconstructive and Aesthetic Surgery, Necmettin Erbakan University Meram Faculty of Medicine, Konya, Turkey
*Corresponding Author: Moath Zuhour, Department of Plastic,Reconstructive and Aesthetic Surgery, Liv Hospital, İstanbul, Turkey.
Citation: İsmayilzade M., Zuhour M., Soylu A., İnce B., Dadacı M., (2023), A Tunneled Posterior Auricular Transposition Flap for Ear Concha Defect, Journal of Clinical Surgery and Research, 4(4); DOI:10.31579/2768-2757/079
Copyright: 2023, Moath Zuhour. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 June 2023 | Accepted: 12 June 2023 | Published: 23 June 2023
Keywords: basal cell carcinoma; concha; ear; transposition flap; tunnel
Surgical treatment of ear defects requires the awareness of reconstructive concepts. Acceptable cosmetic appearance is not always achievable because of its complex anatomy, a limited availability of soft tissue around defects and a great number of aesthetic units. Retro-auricular zone is frequently applied as a flap donor area because of its rich vascularization. While repairing of the ear defects, three-dimensional structure and different plane of the ear on the mastoid surface should be taken into consideration very carefully. In this case we present a case of basal cell carcinoma on the concha of the ear. The resulting defect was repaired with a tunneled posterior auricular transposition flap which provided a good aesthetic result.
An ear region entails a risk for nonmelanoma skin cancers in terms of the recurrence rate and agressive progress [1]. Surgical treatment of ear defects requires the awareness of reconstructive concepts. Acceptable cosmetic appearance is not always achievable because of its complex anatomy, a limited availability of soft tissue around defects and a great number of aesthetic units. Defect related parameters such as size and depth are the main factors in the choice of reconstructive option in this region. The options of skin graft, local flaps, island flaps, distant flaps etc. are frequently considered as a treatment method of ear defects. Retroauricular zone is frequently applied as a flap donor area because of its rich vascularization [2]. While repairing of the ear defects, three-dimensional structure and different plane of the ear on the mastoid surface should be taken into consideration very carefully. Thus, tunneled flaps are much more preferable in this topography than the bridging flaps which require two sessions of surgeries. In this case report, we demonstrated the usage of a tunneled posterior auricular transposition flap for coverage of the defect including conchal cartilage succesfully.
Case Report
A 68-years old male patient applied to our department with the lesion in the inner side of his ear accompanying with intermittant bleeding attacks from its surface. The patient had a history of skin cancer removal surgery several times and he had a diagnosis of basal cell carcinoma from the previous pathology reports. While planning the surgery the underlying cartilage invasion by tumor was also took into consideration because of the higher risk localization. The patient underwent the operation under local anesthesia and 0,2 cm surgical margin was planned before the resection. Tumor was excised including underlying conchal cartilage remaining the posterior wall intact. A superior pedicled transposition flap along the posterior fold of the ear was designated. After flap harvesting, vertical cut was done in the posterior cartilage where the flap planned to be passed through. Flap was reached to the defect after passing through the tunnel and the area which was planned to be de-epithelialized was marked. After de-epithelialization flap adaptation to defect area was completed (Figure 1). Flap donor area was closed primarily in a tension- free manner (Figure 2). The pathology result was reported as basal cell carcinoma with the tumor free surgical margins and it was similar to the previous reports of the patients. No complication was encoutnered in the follow-ups.

Figure 1: Early postoperative view after the inset of the flap.
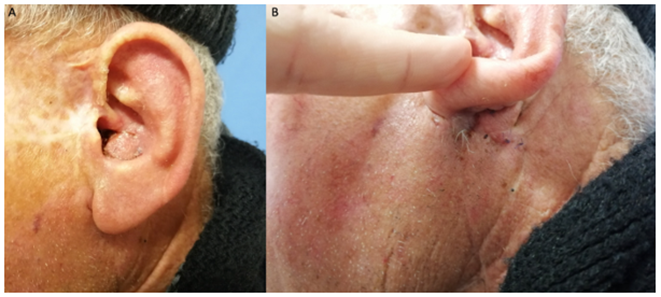
Figure 2: A: late postoperative view. B: Posterior donor area with minimal scar.
Nonmelanoma skin cancers of concha increase morbidity because of the higher rate of recurrence and cartilaginous infiltration by tumor [3,4]. Because the skin cancers presented in this area should be evaluated in terms of cartilage invasion MOHS surgery is recommended [1]. MOHS surgery and intraoperative frozen section were not provided in our hospital, thus we performed enbloc resection of tumor including underlying cartilage due to the possible infiltration. Skin grafts are also considered as a reconstructive option in concha tumors if the cartilage is not removed. In their randomized controlled study, Dessy et al. demonstrated the favorable outcomes of retroauricular flaps in the wide concha defects comparing to skin grafts [5]. It was reported that preference of skin grafts can increase the operating time, slow down the healing period causing centripetal contraction in surgical area, and result in unfavorable aesthetic outcomes. In our case, we preferred the flap reconstruction to prevent the contour deformity in a wound bed without cartilage. Though there are several flap options for the partial reconstruction of ear, the concept including tunnelization of retroauricular flaps to cover cartilagineous framework has been frequently performed by surgeons. In 1972, retroauricular island flap for concha defects was firstly defined as a ‘revolving door flap’ by Masson [6]. The retroauricular island flaps are usually based on a adipofascial pedicle and do not require the second session. We prepared a transposition flap in our case and the only part which remained under tunnel was de-epithelialized. This kind of planning decreases the venous outflow problem which is common in island flaps. The similar transposition flap was previously reported by the auhtors for the earlobe reconstruction [7]. The disadvantage of the flap mentioned in the case was a bulge in pivot point however it was camouflaged in the posterior fold of ear.
In conclusion, tunneled posterior auricular transposition flaps may be alternative to retroauricular flaps in the selected cases with concha defect. The future investigations comparing the rate of complication and aesthetic outcomes of the flaps will contribute to the literature positively.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
