
Research Article | DOI: https://doi.org/10.31579/2692-9562/042
1 Federal University of São Paulo, Paulista School of Medicine. Department of Otorhinolaryngology and Head and Neck Surgery, Discipline of Otology and Otoneurology, Sao Paulo, SP, Brazil.
*Corresponding Author: Marília Batista Costa, Federal University of São Paulo, Paulista School of Medicine. Department of Otorhinolaryngology and Head and Neck Surgery, Discipline of Otology and Otoneurology, Sao Paulo, SP, Brazil.
Citation: Marília Batista Costa, Beatriz Santos Botelho, Adriana Perez Ferreira Neto, Norma de Oliveira Penido, Ektor Tsuneo Onish (2022) A Systematic Review of the Auditory and Vestibular Effects of Chloroquine and Hydroxychloroquine Journal of Clinical Otorhinolaryngology 4(2); DOI: 10.31579/2692-9562/042
Copyright: © 2022, Marília Batista Costa. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 19 November 2021 | Accepted: 07 December 2021 | Published: 21 May 2022
Keywords: chloroquine, hydroxychloroquine, ototoxicity, hearing Loss, COVID-19
Introduction: chloroquine and hydroxychloroquine are antimalarial drugs that, although normally well tolerated, have side effects, such as gastrointestinal intolerance, retinopathy and arrhythmias. There are reports of sensorineural hearing loss, tinnitus and vertigo related to the two drugs. However, the ototoxic potential of these medications is routinely not researched. With the significant increase in the use of these drugs in the face of the COVID-19 pandemic, the study of their ototoxic effects becomes even more important.
Objective: to evaluate the ototoxic potential of chloroquine and hydroxychloroquine through a systematic review of the articles available in the literature.
Method: a search for articles published until April 2020 was carried out in the PubMed, Web of Science, SciELO and Lilacs databases, with descriptors registered in MeSH. Articles that associated the use of chloroquine or hydroxychloroquine with auditory and / or vestibular effects were included.
Result: the search resulted in 161 articles, of which 18 met the inclusion criteria. Of these, 16 demonstrated ototoxic effects of chloroquine and / or hydroxychloroquine. Chloroquine was considered the second main drug involved in ototoxicity in 2 studies. A 5-fold higher risk of hearing loss has also been reported in neonates whose mothers used chloroquine during pregnancy.
Conclusion: studies have shown that chloroquine and hydroxychloroquine have ototoxic action, which may initially go unnoticed if there is no active investigation. The significant increase in the use of chloroquine and hydroxychloroquine in the face of the COVID-19 pandemic may represent an escalation in ototoxicity, which should not be neglected.
Chloroquine is an antimalarial drug synthetically derived from quinolone and developed more than 80 years ago, during World War II. Due to its side effects, in 1945 a new equally effective and less toxic drug was synthesized: hydroxychloroquine. In the late 1950s, these drugs were gradually added in the treatment of autoimmune diseases [1-2].
Generally, these drugs are well tolerated and rarely need to be discontinued due to systemic adverse effects. However, they can be irreversibly toxic and severe for the visual, cardiovascular, neuromuscular, and auditory systems, as well as causing gastrointestinal intolerance and skin reactions when taken in higher doses. These last two can be easily resolved by reducing the dose or discontinuing the medication [3-5]. The pharmacokinetics of chloroquine, with a long plasma half-life, leads to its accumulation in the plasma when taken in higher dosages, especially in patients with renal or hepatic impairment, facilitating the appearance of more serious side effects [6]. Hydroxychloroquine toxicity is known for being significantly lower, but there are concerns about its cardiotoxicity (cardiomyopathies and prolongation of the QT interval), which can be lethal [7].
The ototoxicity caused by medications is defined by the temporary or permanent decline in auditory and/or vestibular functions induced by their use [8]. Auditory and vestibular disorders were described as chloroquine side effects, being widely observed in patients being treated for malaria and systemic lupus erythematosus. It has been shown that this medication induces oxidative stress in Schwann cells, vascular injury and degenerative lesions in the inner ear [4, 9]. Regarding hydroxychloroquine, there are reports of its ototoxicity, but with no exact elucidation of its injury mechanism [10, 11].
Tinnitus, sensorineural hearing loss (SNHL), and vertigo are the most common symptoms resulting from ototoxicity caused by antimalarial drugs. Brainstem Evoked Response Audiometry (BERA) appears to be the most sensitive test to detect early cochlear injury due to the use of these medications. The ototoxicity of these drugs is believed to be reversible, as would appear some studies have shown that the cochlear-vestibular system can recover if medication is discontinued and adequate corticosteroids treatment and plasma expansion are applied [12]. The reversibility of dysacusis resulting from the use of these medications depends on the length of administration and the management after its interruption [13, 14].
Currently, amid the pandemic caused by the new coronavirus (Sars-CoV-2) and the difficulty in finding an effective treatment for the disease of the new coronavirus 2019 (COVID-19), in the course of a public health emergency, the Ministry of Health authorized, through official note number 5/2020-DAF/SCTIE/MS, published in March 2020, such drugs to be used as a therapeutic alternative in severe cases of hospitalised patients [15]. In May 2020, the Ministry of Health published new guidelines for the early treatment of patients diagnosed with COVID-19, authorizing the use of chloroquine or hydroxychloroquine on outpatients with mild signs and symptoms of the disease [16]. Thus, the criteria for indicating these medications have been expanded, significantly increasing the number of patients exposed to their potential ototoxic effects.
The protocol for the use of antimalarials involves periodic ophthalmological, electrocardiographic, and liver enzyme dosage, in order to detect early toxicity in these organs. Cochlear vestibular impairment, however, has been ignored and rarely investigated [9]. Therefore, the most in-depth knowledge about the auditory and vestibular effects become necessary given the unbridled use of this medication in the current health scenario.
The objective of this paper is to evaluate the scientific evidence of the auditory and vestibular effects in patients using chloroquine and hydroxychloroquine, comparing randomized controlled trials and other studies available in current literature, through a systematic review.
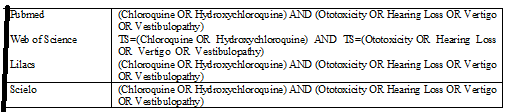
A systematic review was performed of the published articles on the use of chloroquine and hydroxychloroquine and hearing loss/vertigo until April 30, 2020 in the databases of PubMed, Web of Science, SciELO and Lilacs. The following descriptors registered in the Medical Subject Headings (MeSH) were used: chloroquine, hydroxychloroquine, ototoxicity, hearing loss, vertigo and vestibulopathy, according to strategies shown in Table 1.
The articles were accessed online, through the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior- CAPES [Coordination of Superior Level Staff Improvement] website, using the Regional Library of Medicine (BIREME), in order to obtain copies of published journals.
Inclusion criteria were articles that associated the use of chloroquine or hydroxychloroquine to auditory and or vestibular effects. However, studies that were not in English, Spanish or Portuguese, as well as letters to the editor and systematic reviews were excluded. Two independent reviewers made the initial selection of articles by reading the title and abstract, and only the studies that met the inclusion criteria were read in full. Discrepancies were resolved by mutual consent. From the selected articles, the following data was extracted: authors, year of publication, study design and its level of evidence, sample size, and main results of association between the use of these medications and hearing loss or vestibular complaints. The classification of the scientific evidence level of each article was carried out following the study design, according to guidelines adapted from The Oxford Center for Evidence-Based Medicine [17].
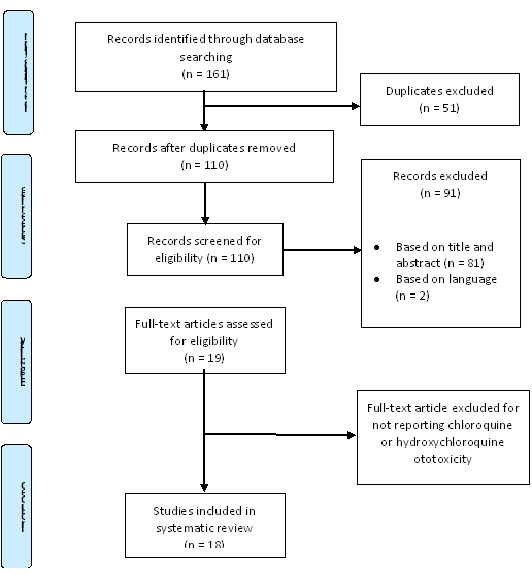
The search resulted in 161 articles, 70 of which were found in PubMed, 61 in the Web of Science, 17 in Scielo and 13 in Lilacs. The articles were published between 1963 and March 2020. Out of the 161 studies, 18 were included in our systematic review after eliminating duplicate studies that did not meet the inclusion criteria, as shown in the flowchart (Figure1). The eighteen articles that met the inclusion criteria did not present the necessary data, from a statistical point of view, for the conduct of meta-analysis.
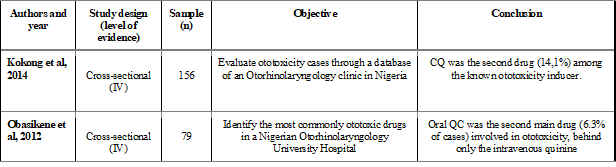
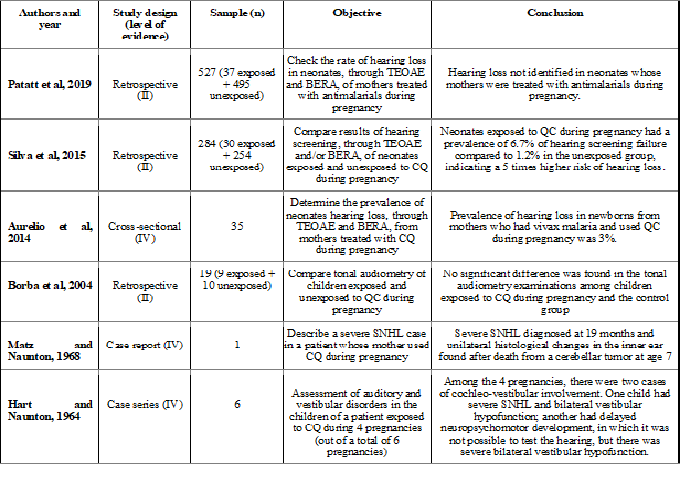
Among the 18 articles, 3 were cross-sectional studies, 1 was prospective, 3 were retrospective, 1 case series and 10 case reports. Regarding the classification by levels of scientific evidence of the selected articles, 3 articles are level II and 15 are level IV. Table 2 shows the studies that evaluated the prevalence of ototoxicity by use of chloroquine. The main interest parameters of the selected articles are in Tables 3 to 5, which were separated, respectively, in: use of chloroquine during pregnancy; ototoxicity caused by chloroquine and ototoxicity secondary to the use of hydroxychloroquine
*CQ: chloroquine; BERA: brainstem evoked response audiometry; TEOAE: transient evoked Otoacoustic emissions; SNHL: sensorineural hearing loss
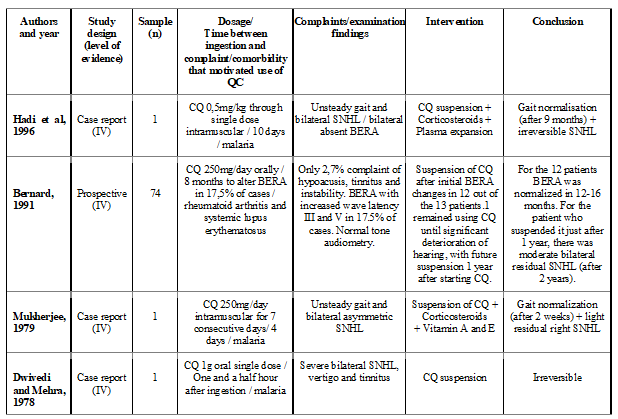
*CQ: chloroquine; BERA: brainstem evoked response audiometry; SNHL: sensorineural hearing loss.
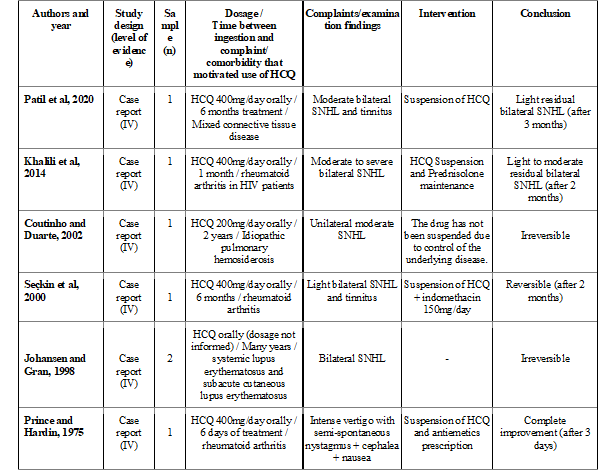
HCQ: hydroxychloroquine; SNHL: sensorineural hearing loss; -: not informed; HIV: human immunodeficiency virus.
Chloroquine is an antimalarial drug with immunomodulatory action in the treatment of rheumatological and dermatological diseases such as rheumatoid arthritis, lupus systemic erythematosus, Sjogren's syndrome and scleroderma [18]. The hidroxychloroquine has the same clinical efficacy, but with less potential for toxicity, a fact that justifies its more common use [9].
Chloroquine is completely absorbed by the gastrointestinal tract. A small part is excreted, and the rest is widely distributed to the tissues. Residues of the drug can last for months in the body, which means its effects continue even after suspension. The most common adverse side events of antimalarial drugs include skin hyperpigmentation and changes in the gastrointestinal tract, such as abdominal discomfort, diarrhea, nausea, and vomiting. Long-term effects, on the other hand, include mainly retinopathy and cardiovascular disorders, such as increased QT interval, cardiac arrhythmias and myocarditis [14].
Ototoxicity is defined as a temporary or permanent loss of auditory and/or vestibular function induced by medication [9]. In studies by [19, 20], chloroquine was the second most commonly known drug responsible for ototoxicity, demonstrating that its potential to damage the inner ear is proven, but it is insufficiently studied and reported. Patients who make chronic use of these medications usually undergo periodic ophthalmological evaluation; however, auditory analysis is often neglected [21].
Chloroquine is accumulated and fixed in the melanocytes. Specifically, in relation to the inner ear, the areas that have melanin are stria vascularis, modiolus, planum semilunatum, saccular and utricular walls and semicircular canals. Most studies suggest that stria vascularis is the most affected, acquiring an atrophic and vacuolated aspect, later affecting the cochlear neurons and the organ of Corti, with destruction of the ciliated and supporting cells [21, 23]. However, Matz and Naunton in the histopathological examination of a teratogenicity case due to the use of chloroquine, did not demonstrate changes in the stria vascularis [24].
There are some hypotheses to explain the mechanism of injury caused by chloroquine in the inner ear. Oliveira et al4 suggested, through glial cells culture of organs of Corti in the mice, the occurrence of neuronal excitotoxicity due to the increase in glutamate in the extracellular environment. This occurs due to the deleterious action of chloroquine on glial cells, which are responsible for the uptake of glutamate into the intracellular environment. Another fact pointed out by the same study is the increase in the production of reactive oxygen species, resulting in local oxidative damage. This explains the use of antioxidant substances, such as ascorbic acid or vitamin E, in the treatment of ototoxicity [4].
Another hypothesis consists of the ischemic mechanism of the ototoxic action of chloroquine, which causes spasms of the cochlear arteries, reducing blood supply to the stria vascularis and the outer ciliated cells [23, 24]. It is believed that the vasoconstriction in the inner ear results from a hypersensitivity reaction to the drug, a fact that justifies the use of corticosteroids in the treatment and the possible reversibility of the condition [14., 19]. The vascular lesion promotes changes in the composition of the endolymph and consequently lesions in the receptor cells. The most exuberant damage occurs in the basal gyrus, responsible for the high frequencies [9]. The hydroxychloroquine mechanism of injury in the inner ear is believed to be similar to that of chloroquine, however there are no studies on the subject.
The symptoms related to ototoxicity are mainly SNHL, tinnitus and instability [25]. The time between the use of antimalarial drugs and the development of cochlear-vestibular complaints is variable and individual. Some reports outline the development of symptoms a few hours after a single dose of the medication, others after the fourth dose or even after chronic use [22, 14, 26]. Hadi et al suggest the possibility of idiosyncratic effects of these drugs.
In audiometry, there is usually a mild to moderate symmetric bilateral SNHL, with a flat or descending configuration [9, 28]. The typical bilateral and symmetrical involvement is easily explained, since chloroquine and hydroxychloroquine have systemic action. However, there are reports of unilateral involvement, as well as reports of asymmetric losses, without other possible justifiable causes, demonstrates that these audiometric findings, although rare, are possible [14, 28].
Bernard12 found alteration in the BERA in 17.5% of cases in patients with rheumatoid arthritis in chronic use of chloroquine. However, only 2.7% reported sporadic symptoms of tinnitus and instability, with normal audiometry and ophthalmic examination. This suggests that the audiological investigation with BERA of patients using antimalarial drugs would be more appropriate, in order to detect early hearing disorders, not yet clinically perceptible, for possible reversibility of the condition.
Hydroxychloroquine is believed to be less toxic and, consequently, safer and less likely to present side effects. Nevertheless, a total of 7 cases of ototoxicity have been reported as a consequence of its use. This demonstrates that hydroxychloroquine has the ability to trigger hearing loss - often irreversible - and vestibular symptoms. Therefore, patients using hydroxychloroquine should also undergo routine audiological investigations for early diagnosis and intervention [10, 11, 21, 23, 26, 28].
The cochlear-vestibular alteration caused by the use of antimalarial drugs can be transient. It is believed that reversibility can occur with early intervention. Mukherjee [14] reported a case of cochlear-vestibular injury caused by chloroquine treated with prednisolone and vitamins A and E, beginning 10 days after the first symptoms, with complete resolution of the vestibular condition and important hearing recovery. Seçkin et al [26], in turn, described a case of SNHL by hydroxychloroquine treated by the suspension of the medication and indomethacin 150mg/day from the first symptoms, with a return to normal thresholds in a period of two months. However, in the case report presented by Hadi et al27, there was no improvement of instability or hearing loss right after the use of corticosteroid therapy and plasma expansion, performed from the tenth day after the beginning of symptoms; after 9 months, the gait normalized, but the SNHL remained profound.
Also, when administered during pregnancy, chloroquine is capable of crossing the placental barrier causing lesions in the inner ear of the fetuses. In Aurelio et al [29] and Silva et al [30] studies, the prevalence of hearing loss in children whose mothers used chloroquine during pregnancy ranged from 3% to 6.7%, with a 5 times higher risk of developing SNHL. However, Patatt et al [31] and Borba et al [18] have not shown this relationship in their studies. It is worth mentioning that hydroxychloroquine is not able to cross the placental barrier, and its use is safe for pregnant women.
In view of our systematic review and considering that chloroquine and hydroxychloroquine are ototoxic and that the time for the development of their cochlear-vestibular effects is variable, it is important to discuss the precautions given the significant increase in the use of these medications in the pandemic scenario of COVID-19. Attention should be paid to the possibility of these patients developing hearing loss and/or vestibular symptoms, in addition to the other possible side effects.
A limitation aspect of this study is the fact that many articles are case reports (with low scientific evidence), sample size and the lack of prospective studies that follow a larger number of patients since the beginning of medication intake, with periodic ototoxicity examinations.
In the light of the objective of discussing the ototoxicity of chloroquine and hydroxychloroquine, the following is highlighted:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
