
Case Report | DOI: https://doi.org/10.31579/2690-4861/1023
1Reproductive Medicine Unit, Service of Gynaecology, Department Woman Mother Child, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
2Andrology and Reproductive Biology Laboratory, Department Woman Mother Child, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland
*Corresponding Author: Sandrine Cuénoud, Reproductive Medicine Unit, Service of Gynaecology, Department Woman Mother Child, Centre Hospitalier Universitaire Vaudois, Av. Pierre-Decker 2, 1011 Lausanne, Switzerland.
Citation: Sandrine Cuénoud, Philippe Renard, Caroline B. Chabot, Anna Surbone, (2026), A Successful Pregnancy and Live Birth after Intracytoplasmic Sperm Injection with Globozoospermic Sperm and Artificial Oocyte Activation, International Journal of Clinical Case Reports and Reviews, 33(5); DOI:10.31579/2690-4861/1023
Copyright: © 2026, Sandrine Cuénoud. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 December 2025 | Accepted: 16 January 2026 | Published: 26 January 2026
Keywords: globozoospermia; artificial oocyte activation; calcium ionophore; fertilization failure; lack of standardized protocol; impact on long-term child development
Globozoospermia is a rare form of teratozoospermia still challenging the success of Assisted
Reproductive Technology (ART). The use of intracytoplasmic sperm injection (ICSI) with artificial oocyte activation (AOA) with an adapted medium containing calcium ionophore made parenthood possible for couples facing fertilization failure with conventional in vitro fertilization (IVF).
Nevertheless, no consensus exists about AOA protocols, making this technique difficult to reproduce. We report the case of a patient with total globozoospermia with successful pregnancy and live birth after a single cycle of ICSI using AOA. Although successful, more research and understanding are required about the use of this method, as fertilization success also depends on multiple other factors and as the impact on long-term child development is still unknown.
Globozoospermia is a rare form of teratozoospermia, concerning less than 0.05% to 0.1% of infertile men [1], characterized by round-headed spermatozoa without acrosomes, with cytoskeleton defects around the nucleus [2] and coiled tails [3]. The absence of acrosome prevents spermatozoa to penetrate the zona pellucida and causes therefore infertility [4]. Singh, in 1992 [5], differentiated two types of globozoospermia. In type I, also called total or classic globozoospermia, all the spermatozoa are round-headed, which causes primary male infertility. In type II or partial globozoospermia, the semen analysis finds both normal and round-headed spermatozoa in a variable proportion. Vicari et al., in 2002, further defined the partial globozoospermia as a form of oligoasthenoteratozoospermia (OAT) with more than 25% of acrosome-less spermatozoa [6], as round-headed spermatozoa can also be found in a smaller proportion in normal ejaculates. The primary cause of globozoospermia is attributed to genetic factors. Mutations in eight human genes (C2CD6, CCDC62, DPY19L2, GGN, PICK1, SPATA16, SPINK2, and ZPBP1), involved in acrosome formation, have been associated with globozoospermia and six additional genes (CCIN, C7orf61, DNAH17, DNAH6, PIWIL4, and CHPT1) may also be implicated, however requiring further confirmation [7].
For couples facing this pathology, the Assisted Reproductive Technology (ART) has been unsuccessful until the introduction of ICSI, as the absence of acrosome prevents fertilization in conventional IVF [1]. Moreover, globozoospermic spermatozoa have a reduced ability to activate oocytes to complete second meiotic division, which reduces therefore the fertilization rate even in ICSI [8, 9].
In the fertilization process, oocyte activation is mainly characterized by intracellular calcium (Ca) oscillations within a few minutes after spermatozoa and oocyte fusion [10]. In ICSI, calcium influx is produced by the ICSI process itself from the culture medium. However, the sub-optimal fertilization rate observed even in ICSI with globozoospermic sperm indicates that, beyond the ability to penetrate inside the oocyte, other essential events must occur after spermatozoa injection in the oocyte, especially those promoted by factors linked to sperm acrosome and calcium influx. Especially, the sperm protein phospholipase C zeta (PLCζ), which evokes the characteristic cytosolic Ca oscillations necessary for completion of meiosis and oocyte activation [8], has an abnormal expression, localization and structure in spermatozoa of globozoospermic patients [11]. Moreover, other factors, like the poor sperm chromatin condensation and the high levels of sperm DNA fragmentation observed in globozoospermic spermatozoa, also contribute to the ICSI sub-optimal fertilization rate, as mentioned further below.
Some authors found that the fertilization and cleavage rate could be increased by using oocyte activating factors, such as calcium ionophore or calcium chloride, with several pregnancies and even live births described [12, 13, 14]. Calcium ionophores increase the calcium permeability of the cell membrane, allowing extracellular calcium to enter the cell, mimicking the physiological cell signaling mechanisms resulting in oocyte activation [13, 15].
The aim of this case report is to describe the clinical management and outcome of a couple with total globozoospermia treated by ICSI combined with calcium ionophore-mediated oocyte activation, and to discuss the place of this strategy in assisted reproductive practice.
We report the case of a patient with total globozoospermia, by whom a single cycle of ICSI using artificial oocyte activation (AOA) with calcium ionophore permitted a pregnancy and a live birth of a healthy girl.
A 30-year old healthy patient visited our fertility unit with his wife for a 2-year primary infertility. He was not known for any significant medical or surgical comorbidities except a slight overweight (BMI 28.4 Kg/m2) and a passed smoking status (3 pack-years). During the infertility work-up, a total globozoospermia was confirmed on 3 different spermograms in a 3-year interval. The last complete sperm test showed an isolated total teratozoospermia with 100% round-headed spermatozoa (Kruger classification 0% of normal shaped spermatozoa) [16], a normal volume and pH, a concentration of 29.6 millions of spermatozoa per ml, 44% progressive motility, and a viability of 81% assessed by using hypo- osmotic swelling (HOS) test. The patient’s partner was 27 years old and she was known for an autoimmune hypothyroidy under Levothyroxin 100 mcg/day and a stage 1 obesity (BMI 31 Kg/m2). She had no gynecological comorbidities, with regular and ovulatory menstrual cycles. Her fertility check at cycle day 5 showed a good ovarian reserve (follicle stimulating hormone (FSH) 5.7 UI/l, estradiol (E2) 0.13 nmol/l, antimullerian hormone (AMH) 17.6 pmol/l, antral follicle count 30).
We performed a first ovarian stimulation using an antagonist protocol synchronized with oral estradiol (Progynova 2 mg twice a day). The stimulation involved a total dose of 937.5 IU of recombinant FSH alpha (Gonal-f) at a daily dose of 187.5 UI for 5 days, followed by a total dose of 1125 UI of urinary gonadotrophins (Merional HG) at a daily dose of 225 UI. For pituitary suppression, we used a daily injection of the GnRH antagonist Cetrorelix 0.25 mg (Cetrotide) starting from the 6th day of stimulation. Ovulation was triggered at the 11th day of stimulation with recombinant human chorionic gonadotrophin (r-HCG) (Ovitrelle), with seven > 13 mm follicles, one > 17 mm follicle and a 4.08 nmol/l of estradiol [17]. Thirty six hours after r-HCG trigger, 10 oocytes were retrieved by transvaginal ultrasound-guided follicle aspiration, of which 8 in metaphase II were microinjected with motile round- headed spermatozoa.
Semen collection was performed after 2 days of sexual abstinence. Sample was stored at 37°C until liquefaction. Semen analysis was conducted according to World Health Organization (WHO) criteria [18]. Briefly, appearance, volume, and pH were first evaluated. The sample was subsequently mixed and a 10 μl aliquot was withdrawn for evaluating the presence of round cells, sperm agglutination and/or aggregation, using a 100x magnification inverted microscope. Finally, sperm concentration and motility were evaluated by using a Computer Aided Sperm Analysis (CASA) System (Microptic mySCA). Semen analysis revealed the following data: volume 3.0 mL; normal appearance and liquefaction time; pH 7.9; no round cells; no sperm agglutination nor aggregation, sperm concentration 47x106/mL; progressive motility 32%; total motility 42%. All sperm cells were round-headed. Semen sample was prepared for ICSI by two-layers (90% and 45%) discontinuous Isolate (Irvine) gradient technique, and sperm pellet was suspended in 0.3 mL G-IVF medium (Vitrolife)[18].
Following ICSI, the injected oocytes were immediately placed into the oocyte activation medium (GM508 CultActive, Gynemed) for 15 min at 37°C and 6% CO2. Oocytes were then washed twice in G- IVF PLUS (Vitrolife) and cultured overnight in G-IVF PLUS (Vitrolife) in a MINC incubator (Cook Medical) at 37°C and 6% CO2 [19].
About 18 hours post-ICSI, only 1 oocyte showed signs of fertilization (2 polar bodies and 2 pronuclei). The subsequent observations revealed the development of a 4-cell embryo at Day 2, and an 8-cell embryo at Day 3 (Photo 1). The day 3 embryo was transferred under progesterone support with 10 mg dydrogesterone three times a day (Duphaston) [17].
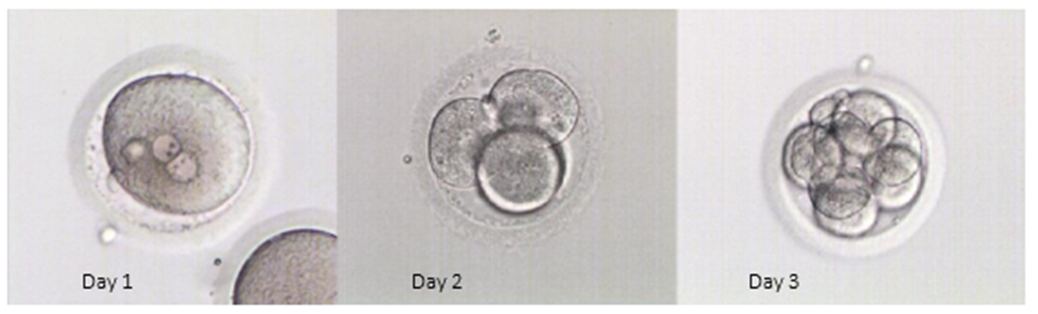
Photo 1: Development stages of transferred embryo from Day 1 to Day 3
The pregnancy test performed 13 days after embryo transfer by serum beta-HCG level was positive (292 UI/l). The first pregnancy ultrasound at 7 1/7 weeks of amenorrhea showed a unique evolutive pregnancy (Crown-Rump Length (CRL) 10 mm) with positive cardiac activity. The pregnancy was marked by an isolated maternal arterial hypertension treated with Labetalol (Trandate) 200 mg three times a day. The patient delivered spontaneously without complication at 38 5/7 weeks of amenorrhea, giving birth to a healthy baby girl (3005 grams, 48.5 centimeters, Apgar score at 1 and 5 minutes 9/9).
This case report underlines the difficulty of reaching fertilization even by ICSI with an adapted medium in case of total globozoospermia. This is due to reduced ability to activate oocyte, but also to poor sperm chromatin condensation and high levels of sperm DNA fragmentation (SDF) in globozoospermic spermatozoa, which can lead to failure of nuclear decondensation, inability to support the early stages of embryo development and consequently fertilization failure [1].
Recently, some studies showed an association of globozoospermia with mutations of several genes affecting oocyte activation and sperm capacitation and finally leading to fertilization failure. A slight increase in aneuploidy rate in the acrocentric and sex chromosomes was also observed, with the result of a diminished development potential of the embryo [7, 20, 21].
Remarkably, the AOA protocols described in different reports diverge in the ionophore concentration used (5–10 mmol/l or unknown), the duration of ionophore exposure (10–30 min), the moment of ionophore exposure following ICSI (immediately or 30 min after ICSI) and the number of ionophore exposures (once or twice) [19, 22, 23].
Another successfully described technique, alone or in combination with AOA, is the motile sperm organelle morphology examination (MSOME), which enables the evaluation of the sperm morphology at high magnification (up to x6600) and increases the chance of success by intracytoplasmic injection of morphologically selected sperm (IMSI) [1]. Sermondade et al., in 2011, described a case of total globozoospermia on classic spermogram, by whom MSOME detected a small bud of acrosome in 1% of the spermatozoa. IMSI was performed using only vacuole free spermatozoa presenting a small bud of acrosome, with a comparable fertilization rate with or without calcium-ionophore AOA [24]. This technique, however, is of limited availability due to its high cost and need for expensive equipment and specialized operators, without guarantee of success.
The existing literature on this topic is scarce and no standardized protocol has been reached yet. Regarding the long-term outcomes, babies born after ICSI with AOA do not seem to have specific medical issues or negative developmental and behavioral outcomes in several studies with a follow-up of the children up to the age of 10 [15, 8]. Nevertheless, some recent studies using mice suggest that AOA might cause epigenetic alterations in the resulting embryos and offspring [8], rendering this procedure still experimental, with further research mandatory.
This case report suggests that ICSI with AOA can result in successful oocyte fertilization, embryo development and pregnancy with birth of a healthy baby. Thus, this method can give the opportunity of fathering even to individuals with totally globozoospermic sperm. Nevertheless, more research is needed to increase the fertilization rate and to definitively assess the impact of this promising technique on the long-term child development.
Contributors: All Authors contributed to planning, literature review and conduct of the review article.
Competing Interests: None
Patient consent for publication: Informed consent was obtained from the patient included in this report
Funding: No funding was obtained for this report
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
