
Research | DOI: https://doi.org/10.31579/2578-8949/089
1 Ex resident, Department of Dermatology, Shree Krishna Hospital, Karamsad.
2 Third year resident, Department of Dermatology, Shree Krishna Hospital, Karamsad
3 Second year resident, Department of Dermatology, Shree Krishna Hospital, Karamsad
4 Senior consultant nephrologist and transplant physician, Shree Krishna Hospital, Karamsad
5 Professor and Head, Department of Dermatology, Shree Krishna Hospital, Karamsad
*Corresponding Author: Rita Vora, Professor and Head, Dept of Dermatology, Shree Krishna Hospital, Karamsad, Anand. 388325 Gujarat.
Citation: R Vora. (2022). A Study of Mucocutaneous Manifestations in Patients with Chronic Kidney Disease. Dermatology and Dermatitis. 7(1); Doi:10.31579/2578-8949/089
Copyright: ©2022 Rita Vora, This is an open-access article distributed under the terms of The Creative Commons. Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 November 2021 | Accepted: 24 November 2021 | Published: 03 January 2022
Keywords: chronic renal failure; mucocutaneous manifestations; chronic kidney disease
Background: Chronic renal failure is associated with diverse mucocutaneous manifestations as a result of underlying etiology as well as due to various treatment modalities which can significantly impair the quality of life.
Aim: To study the clinicodemographic profile of Chronic Kidney Disease (CKD) patients and to compare the cutaneous manifestations in CKD both on dialysis and pre-dialysis group.
Methods: This study was carried out in the Department of Dermatology, Venereology and Leprology, Medicine and Dialysis unit at Shree Krishna Hospital, Karamsad, Anand. One hundred and twenty patients with CKD were examined for mucocutaneous changes over a period of one year. The descriptive statistics was used to describe the quantitative data and the qualitative data was presented using frequency and analyzed using Chi Square test.
Result: All one hundred and twenty patients had at least one mucocutaneous condition due to CRF. The most prevalent finding was xerosis (34 Pre-dialysis+ 31 Dialysis) 65(54.2%), followed by pruritus (33 Pre-dialysis+ 24 Dialysis) 57(47%), pallor (6 Pre-dialysis+21Dialysis) 27(22.5%) and cutaneous pigmentation (10 Pre-dialysis+14 Dialysis) 24(20%). Other cutaneous manifestations included fungal 10(8.3%), viral 9(7.5%) and bacterial 7(5.8%) infections, purpura 9(7.5%),perforating disorder 6(5%),uremic frost 1 (0.83%).The nail changes included onychomycosis 5(4.2%), koilonychia 4(3.3%),half and half nail 2(1.7%), subungual hyperkeratosis 2(1.7%) and onycholysis 2(1.7%). Hair changes included brittle and lusterless hair 21(17.5%), sparse scalp hair 10(8.3%) and sparse body hair 8(6.7%). Oral changes included xerostomia 15(12.2%), ulcerative stomatitis 4(3.3%) and angular cheilitis 4(3.3%).
Conclusion: The most common mucocutaneous manifestations in the patients under our study were xerosis and pruritus, irrespective of hemodialysis status. Early recognition and treatment can reduce morbidity and improve these patients' quality of life. In all such patients, lifelong follow up is needed.
Chronic kidney disease (CKD) is a worldwide public health problem. Adverse outcomes of CKD include loss of kidney function, sometimes leading to kidney failure, cardiovascular disease and mucocutaneous manifestations. These can be prevented or delayed by early diagnosis and treatment. Unfortunately, CKD is under-diagnosed and under-treated [1]. Indeed, it has been recently estimated that the age-adjusted incidence rate of End stage renal disease (ESRD) in India is 229 per million population [2], and >100,000 new patients enter renal replacement programs annually [3]. Mucocutaneous manifestations usually reflect the internal condition. CKD is an irreversible deterioration in renal function classically developing over months or years through five stages and is defined as kidney damage or glomerular filtration rate <60>
Non modifiable risk factors for the progression of CKD are genetic, age, family history, gender, ethnicity. Modifiable risk factors are diabetes, hypertension, anemia, smoking, inflammation, obesity, nephrotoxic drugs, systemic conditions, persistent activity of underlying disease, persistent proteinuria, hyperlipidemia, hyperphosphatemia, cardiovascular disease. Other factors include elevated angiotensin II, hyperaldosteronism, increased endothelin, decreased nitric oxide
Specific mucocutaneous manifestations of CKD include acquired perforating dermatosis, calcific uremic arteriolopathy (calciphylaxis), bullous lesions and nephrogenic fibrosing dermopathy. Nonspecific manifestations include pruritus, xerosis, nail disorders, hair disorders, pigmentary changes, purpura, mucosal changes, pallor, and uremic frost etc. Based on Etiology these can be divided into: 1) Associated with ESRD, 2) Due to Uremia, 3) associated with dialysis, 4) Due to renal transplant
According to site of involvement they can be divided as follows:
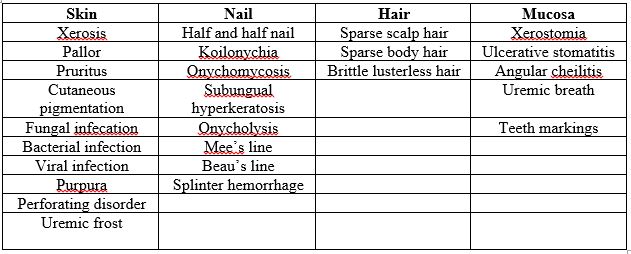
The cutaneous, mucosal, nail and hair changes in CRF patients are impacted by climatic conditions of the locale, race, socioeconomic conditions of patients, accuracy of diagnosis and the light of environment in which cutaneous examination have been done [9].The present clinicodemographic study is aimed to reflect the frequency of different dermatologic changes including those of skin, mucous membrane, hair and nails in patients of CRF in both pre-dialysis and dialysis group.
A cross sectional study was carried out in the Department of Dermatology, Venereology and Leprology, Medicine and Dialysis unit at Shree Krishna Hospital, Karamsad, Anand after approval from ethical committee at a tertiary care hospital over a period of 1 year. Patients with Chronic Kidney Disease(CKD) attending the Nephrology OPD, Dermatology Department (OPD), Medicine Department (OPD and IPD), and Dialysis Unit of Shree Krishna Hospital were recruited after taking their written consent. A detailed history was taken, and a thorough general, physical, local and systemic, cutaneous examination was carried out. If not done previously, investigations like Histogram with DC, Random blood sugar, Blood urea, Serum Creatinine, Serum electrolytes, serum calcium, phosphorus, thyroid, parathyroid hormone level, renal biopsy were done. Skin biopsy, KOH wet mount, tzank smear of the skin were done when clinically indicated. Photographs were be taken after taking patient's consent and ensuring them that confidentiality will be maintained at all levels.
Total 120 patients with chronic kidney disease (CKD) were included in the study. Sixty-eight (56.7%) patients were in pre-dialysis group and fifty-two (43.4%) were in dialysis group. The age of the patients ranged from 11 years to 73 years, with the mean age of 53.14 years. 51-60 years was the most commonly affected age group in pre-dialysis group. More than 60 years was the most commonly affected age group in dialysis group. According to education wise distribution maximum patients were graduate 53(44.2%) while 12(10%) patients were illiterate and 12(10%) were post graduate. Occupation wise, highest number of cases was found to have office jobs with 30(25%) cases.
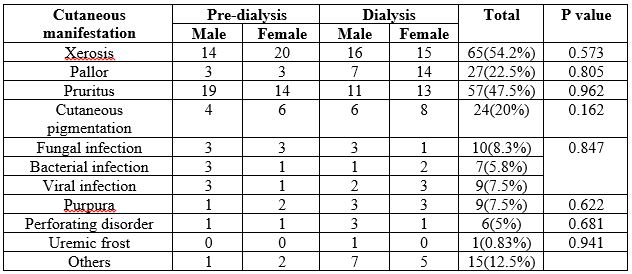
Xerosis was the most common cutaneous abnormality in sixty-five (54.2%) cases, while pruritus was present in fifty-seven (47.5%) cases and pallor was present in twenty-seven (22.5 %) cases.
Out of 65 patients with xerosis, thirty-one (25.8%) cases had Dry skin, while twenty (16.7%) had smooth skin and fourteen (11.7%) had dry skin with scaling. 34 cases were of pre-dialysis group and 31 were of dialysis group. From all the patients ,total 26(21.7%) patients had infections, fungal in 10(8.3%), bacterial in 7(5.8%), and viral in 9(7.5%). In our study, out of 65 patients with xerosis, thirty one(25.8%) cases had dry skin, while twenty(16.7%) had smooth skin and fourteen(11.7%) had dryskin with scaling, according to modified morton’s scale for xerosis. Out of 120, 16 cases had pigmentation over photo exposed areas and 8 had over non-photo exposed areas, 10 were pre-dialysis patients and 14 were of dialysis group. Among 120, 10 having sparse scalp hair, 8 having sparse body hair, 21 having brittle lusterless hair, 16 were pre-dialysis patients and 23 were dialysis patients. In our study, we did not find any patients with Mees lines, Beau’s lines or splinter hemorrhages in neither dialysis nor pre-dialysis group.
Among 120 CKD patients in our study, 66 were males and 54 were females. 68 were of pre dialysis and 52 were of dialysis group. In the dialysis group the most commonly affected age group was more than 60 years with twenty (38.5%) cases followed by fifteen (28.9%) cases in 51-60 years age group. In pre dialysis group, the most commonly affected age group was 51-60 years with twenty one (30.8%) cases followed by nineteen (28%) cases who were more than 60 years. In our study, age ranged between 11 and 73 where as in Rashpa et al [10], 21 was the youngest and 85 was the oldest age.
In our study, all 120 patients had at least one dermatological manifestation, 92.5% had at least one skin manifestation. Along with skin, nail, hair and mucosal manifestations were seen in 12.5%, 32.5% and 19.2% respectively. In Chanda et al [11], out of 100 patients, 95% had at least one skin manifestation and nail, hair, and mucosal manifestations were seen in 46%, 16%, and 10% respectively. In Pico et al [9]and Bencini et al [12] prevalence of mucocutaneous disorders with kidney disease was seen in 100% and 79% respectively. Nunley [6] reported that 50-100%of patients with ESRD had at least one cutaneous lesion. Udayakumar et al [8] has studied cutaneous disorders in hemodialysis group and changes were present in 82
The most common mucocutaneous manifestations in the patients under our study were xerosis and pruritus, irrespective of hemodialysis status. Early recognition and treatment can reduce morbidity and improve these patients' quality of life. Patients with end stage renal failure (ESRD) may present with an array of skin abnormalities. With the advent of hemodialysis, the life expectancy of these patients has increased, giving time for more and newer cutaneous changes to manifest. Some prophylactic and remedial measures can prevent or decrease some of the adverse changes. These include emollients for xerosis; sunscreens, sun avoidance measures and clothing for pigmentary changes and cutaneous malignancies; oral hygiene to prevent oral mucosal changes; nutritional supplementation to prevent vascular fragility, angular cheilitis and hair loss; and prompt recognition and treatment of fungal infections like onychomycosis and tinea pedis, which are increased in CRF. Lifelong follow-up is needed to reduce the morbidity from dermatoses considered CKD/hemodialysis specific that may appear over time. Short duration and the cross-sectional nature of the study are some of the limitations of this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
