
Research Article | DOI: https://doi.org/10.31579/2578-8868/329
Department of Neurosurgery and Gamma Knife Center, International Medical Center (IMC), 42 km. Ismailia Desert Road, Cairo, Egypt.
*Corresponding Author: Raef F.A. Hafez, Osama M. Fahmy, Hamdy T. Hassan., (2024), A single institution retrospective study of efficacy and complications perspective of Gamma Knife Radiosurgery for benign skull base meningioma: A 12-year follow-up, J. Neuroscience and Neurologic
Citation: Raef F.A. Hafez, Osama M. Fahmy, Hamdy T. Hassan., (2024), A single institution retrospective study of efficacy and complications perspective of Gamma Knife Radiosurgery for benign skull base meningioma: A 12-year follow-up, J. Neuroscience and Neurological Surgery, 16(1); DOI:10.31579/2578-8868/329
Copyright: ©, 2024, Raef F.A. Hafez. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 25 June 2024 | Accepted: 12 July 2024 | Published: 26 July 2024
Keywords: cranial nerve; gamma knife radiosurgery; meningioma; stereotactic radiosurgery; skull base
Background and Objectives: Gamma knife radiosurgery (GKRS) has established its role as an effective treatment modality for inaccessible, recurrent, and residual benign skull base meningioma. Therefore, it is necessary to study the outcome in the long term. The current retrospective study aims to analyze and report the clinical and radiological outcomes after long-term follow-up of GKRS for skull base meningiomas >= 12 years.
Patients and methods: The present study was conducted on 106 consecutive patients harboring benign skull base meningiomas treated by GKRS at our IMC center between 2005 and 2012 and was followed till the end of 2023.
Results: After a median follow-up of 13 years (3.6-18 years), a tumor control rate was reported in 88.7% of patients (n 94/106). Recurrences and tumor progression occurred in 11.3% (n 12/106) at a median follow-up period of 5.4 years (3–10.3 years). The 3, 5-, 10-, 12-and 15-year actuarial tumor control rate was 100%, 95.3%, 89.7%, 88.7%, and 78.1% respectively.
Conclusions: The current retrospective study provides a long-term 12-year follow-up and comprises one of the longest follow-up studies of GKRS-treated benign skull base meningiomas. The current series documents a persistent long-term high local tumor control and an acceptable low incidence of neurological deficits. Benign skull base meningioma volume variant at the time of GKRS is a statistically significance predictor factor for tumor control at long-term outcomes.
Meningiomas are the most common intracranial tumor, comprise 37.6% of all primary central nervous system tumors. They are mostly benign tumors, derived from the arachnoid cap cells of the leptomeninges. One-third of intracranial meningiomas arise from the skull base. Surgery is the primary management option for symptomatic meningioma patients as it provides long-term disease-free survival for more than 90% of patients. [1, 2, 3, 4, 5, 19, 20] However, the proximity of these tumors to critical neurovascular structures makes complete surgical removal extremely difficult. [12, 13, 33, 36, 38]
Skull base meningiomas are often impossible to remove completely. Despite advances in microsurgical techniques, anesthetic management, and postoperative intensive care, surgical access to skull base meningiomas remains a challenge, and the related mortality and morbidity rates are still high. Therefore, surgery alone cannot be the ideal long -term solution to treat all skull base meningiomas. [8, 9, 14, 15, 16]
Gamma knife radiosurgery (GKRS) has been reported as a potentially effective alternative to surgical removal of small-to moderate-sized meningiomas especially at the skull base, and as an adjuvant treatment modality for recurrent and postoperative residual meningioma’s that achieves high rate of tumor control with a lower risk of complications [13,34]. The goal of GKRS, whether used as primary therapy or adjuvant therapy after surgery is to prevent tumor growth, and maintain or improve neurological function. Meningiomas are considered an ideal tumor type for GKRS due to their clear demarcation from the normal brain, and accurate localization with today's advanced neuroimaging techniques. [10, 11, 12]
The concept of planned surgical/GKRS cooperation for skull base meningioma has become more solidified where the need for aggressive tumor resection is reduced as GKRS offered a documented long-term tumor control with acceptable risks of complications. [7, 19, 25, 37]
Objective; The current retrospective consecutive cohort study reports the =>12-year follow-up of skull base meningioma patients treated with Gamma Knife radiosurgery according to current clinical and technical standards. Because of the known slowly growing benign skull base meningioma natural course, this study aims precisely to the report the long-term outcome efficacy and complication of GKRS treatment for these tumors.
Patients’ population; All records of the studied consecutive 106 patients with symptomatic benign meningioma at the skull base undergoing Gamma Knife radiosurgery between January 2005 and January 2012 at the Department of Gamma Knife Radiosurgery (GKRS) / International Medical Center (IMC)-Cairo-Egypt, were thoroughly retrospectively reviewed, analyzed and reported. These patients were included in a long-term =>12-year follow-up. Patients with anaplastic or atypical meningiomas, multiple meningiomas, with history of cancer, neurofibromatosis-II, and those without complete radiological and clinical data were excluded from the current study. GKRS-treated benign skull base meningiomas in the current study had been classified histologically according to WHO grade I in 28 patients and based on radiological criteria in 78 patients (Based on typical imaging findings, including a clear definition of the lesion, wide dural base, extra-axial location, uniform contrast enhancement, and sometimes intratumor calcification).
The anatomical locations reported of treated skull base meningiomas were cavernous sinus and parasellar meningioma in 31.1 (n 33/106, cerebellopontine angle meningioma in 20.8% (n 22/106), petro-clival &petrous apex in 13.2% (n 14/106), sphenoidal ridge in 12.3% (n 13/106), anterior clinoid meningioma 10.4% (n 11/106), olfactory groove (n 5/106), foramen magnum meningioma (n 3/106), suprasellar (n 3/106), tuberculum sellae and intra-orbital meningioma each in 1 patient. [Table I]
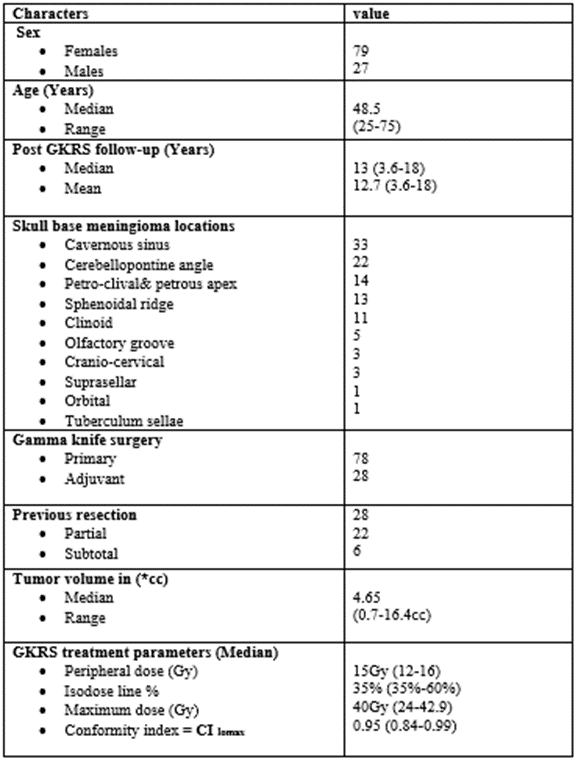
*cc=cubic centimeter
Table 1: Patient's population, tumors characters, and GKRS parameters
Neurological and cranial nerve deficits pre-GKRS were reported, including intermittent headache in 36 patients, diplopia and ocular movement disorders in 26 patients, trigeminal nerve affection in 22 patients (trigeminal neuralgia in 8 and trigeminal paresthesia in 14 patients, visual acuity and visual field deterioration in 18 patients, hearing deterioration in 14, motor weakness in 4 patients and 5 patients presented with seizures activity. [Table 2]
| No. of patients Pre -GKRS | No. of patients Post- GKRS | |||
| Neurological and cranial nerve deficits | Improved | Stable | Neurological and cranial nerve deficits post-GKRS | |
Headache
| 36 | 12 | 22 | No new agonizing persistent headache |
| Ocular movement disorders | 26 | 15 | 11 | - |
| visual acuity and visual field defect | 18
| 4 | 14 | 2 Permanent |
| Trigeminal Paresthesia | 14 | 4 | 10 | 5
|
| Trigeminal neuralgia | 8 | 2 | 6 | 1 Controlled |
| Facial nerve palsy | 3
| - | 3 | 1 partial |
| Hearing affection up to loss | 14 | 2 | 12 | 2 Permanent |
Bulbar symptoms
| 2 | - | 5 | - |
| Motor weakness | 4 | 1 | 3 | -
|
Ataxia
| 7 | 2 | 5 | - |
| Seizure activity | 5
| - | 5 | 2 Controlled |
Anosmia
| 4 | - | 4 | - |
| Exophthalmos | 3
| - | 3 | - |
| Dizziness | 11 | 5
| 6 | - |
Table 2. Pre. and post-GKRS neurological and cranial nerve deficits
Gamma knife procedure
The treatment was carried out using a 201 source Cobalt-60 Leksell Gamma Knife Model B and Model 4C-APS (Elekta AB, Stockholm, Sweden). In all cases, a stereotactic frame was applied under local anesthesia followed by a gadolinium-enhanced stereotactic MRI scan 1.5 Tesla. The tumor outline was delineated on the T1-weighted scans (Axial and or coronal acquisition), which were imported into the planning software (Leksell Gamma Plan). The tumor margins including critical anatomical structures were outlined, and the dose plan was created with isodoses, prescription doses, and maximum doses being determined by the responsible neurosurgeon and a medical physicist. The contrast-enhancing dura adjacent to the meningioma, dural tail, usually included within the GKRS treatment field within the prescription isodose whenever feasible.
Follow-up
Follow-up Clinical and radiological follow-up information was gathered by retrospective review of detailed patient records and attendance. MRI and clinical data were reviewed retrospectively as part of the clinical routine. Following GKRS, all patients underwent a clinical evaluation with accompanying imaging follow-up annual MRI in the first 5 years after GKRS and with bi-annual MRI thereafter or whenever needed. All follow-up MRI images were reviewed by neurosurgeons and neuroradiologists. The tumor size measured on the images was classified as tumor control (TC) i.e. (Regressed or stable) or lost tumor control (LTC), i.e. progressed. The images were also assessed for central necrosis or transient swelling.
These images as well as the radiological reports were used for the assessment of local tumor control after radiosurgery. The median (±SD) radiological and clinical follow-up period after the initial GKRS was 13 ± 3.29 years (3.6–18 years).
Statistical analysis
Kaplan-Meier plots were used to estimate the actuarial tumor control rates by applying the Med Calc-version 22.021. Descriptive statistics were calculated for all variables, including mean, median, standard, and frequency distributions as appropriate. Multivariate analysis was carried out using the Cox proportional hazards regression analysis including multiple covariates for assessing prognostic factors including patient age, tumor volume, peripheral prescription dose, maximum dose, conformity index of Lomax (CI Lomax) [40], and if there was pre-GKRS surgery.
In the present study skull base meningioma represented 43.6% (n 106-243) of all GKRS-treated meningioma patients in the same period of follow-up. During the observation period, 5 patients were re-treated with additional Gamma Knife sessions due to tumor progression.
The median age (±SD) at initial Gamma Knife treatment was 48 ± 10.64 years (25–75 years). There were 79 female and 27 male patients. The median tumor volume (±SD) at the time of radiosurgery was 4.65±3.59cc (range 0.7–16.4 cc). The median (±SD) prescription dose was 15.000 ± 1.23Gy (12-16Gy), the median maximum dose was 40.00±5.46Gy (24-42.9Gy), and the median CI Lomax was 0.95 ± 0.037 (0.84-0.99).
Before radiosurgery, 26.4 % of patients (28/106) had undergone an open tumor resection in various neurosurgical centers including ours.
Post-GKRS tumor Control: The overall tumor volume control was achieved in 88.7% (n =94) of patients at the last MRI control images. Tumor reduction was confirmed in (n 18/94pateints) 19.2% and stationary tumor size was observed in 80.8% (n 76/94). At the last follow-up, tumor progression was documented in 11.3% (n 12/106).
Seventy-eight patients (73.6%) had GKRS as a primary treatment with no previous surgical resection. Within this group, tumor control was attained in 88.5% (n 69/78 patients). In these patients who underwent a previous surgical resection 26.4%, (n 28/106), tumor control was attained in 89.3% (n 25/28). This difference between the groups did not reach statistical significance (P < 0>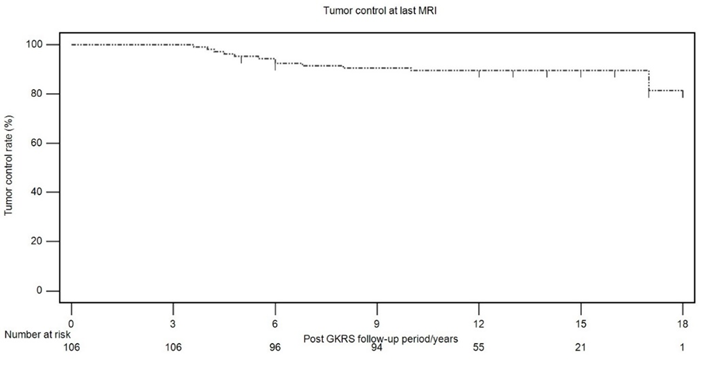
Figure 1. Kaplan-Meier curve presenting the 3, 5-, 10-, 12-and 15-year actuarial tumor control rate was 100%, 95.3%, 89.7%, 88.7%, and 78.1% respectively.
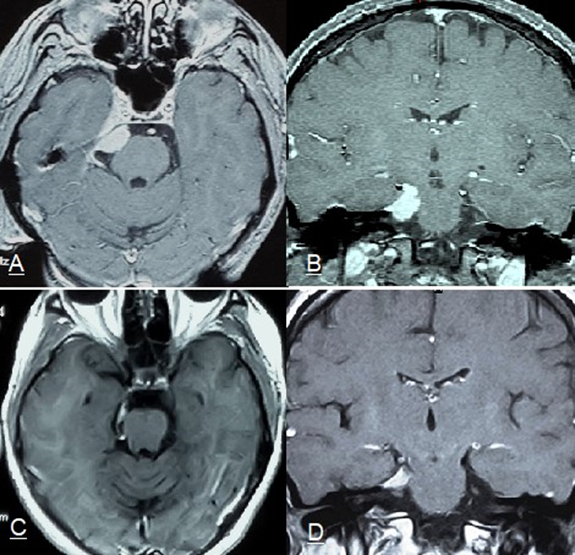
Figure 2. (A&B) T1-weighted contrast axial and coronal stereotactic MRI images of right petro-cavernous meningioma in a 40-year-old woman of 2.8 cc tumor volume presenting with right 6th nerve palsy and trigeminal pain treated with GKRS with 15Gy marginal dose at 50% isodose curve with 98% tumor coverage. (C&D) 14 years Post GKRS follow-up axial and coronal MRI showing local tumor control with evident decreased of treated tumor volume. The patient showed improvement clinical condition.
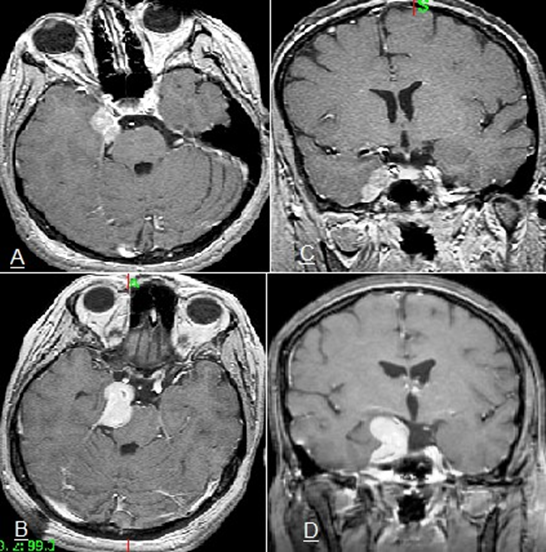
Figure 3. (A&B) T1-weighted contrast axial and coronal stereotactic MRI images of 1.9 cc right cavernous sinus meningiomas in a 27-year-old woman, presenting with right 3rd nerve palsy, ptosis, and right facial numbness treated with GKRS with 15Gy marginal dose at 50% isodose curve with 98% tumor coverage. (C&D) 5 years Post GKRS follow-up axial and coronal MRI confirmed lost tumor control LTC (tumor progress in Y&Z coordinates), the patient was retreated with GKRS
Post-GKRS clinical control: A total of 87.7% of patients (93/106) confirmed an unchanged or improved clinical status at the last follow-up. A later clinical deterioration associated with the treated skull base meningioma occurred eventually in 12.3% (n 13/106). In 8 out of 13 patients with later clinical deterioration, the symptoms were related to tumor recurrence and progression. None of the patients developed adverse radiation complications through the follow-up period.
A new onset of trigeminal neuralgia developed in one patient, additional trigeminal paresthesia in 5, deterioration of serviceable hearing in 2, and progressive deterioration of visual field in 2 patients with anterior clinoidal meningiomas. One developed new facial nerve palsy and one had motor weakness. Transient peritumoral edema was detected in 4 cases post-treatment; two of them developed a new onset of seizure activity. [Table 2]
A combined outcome parameter, favorable outcome, defined as a combination of tumor volume control and clinical neurological improvement or stability at the last evaluation, was attained in 85% of patients (n 90/106).
Skull-base meningioma typically presents many treatment challenges related to tumor location, patient age, comorbidities, recurrence after incomplete resection, and risks of neurological morbidity with microsurgery. The options available for the management of skull base meningiomas include observation with serial imaging studies, SRS, and surgical resection. For patients with small, asymptomatic tumors, observation can be considered. [4, 10] However, owing to the proximity of these tumors to critical neurovascular structures, tumor growth will often be associated with neurological deficits. [12, 13, 17, 38]
Complete tumor removal can be achieved in nearly all meningiomas located over the hemispheres. However, management in skull base meningioma is complicated by the proximity to neurovascular critical structures, thus an incomplete tumor resection as a surgical result is more frequent. [4, 7, 8, 33] With large Petro clival meningioma, tumor progression was observed in 15% of patients who had reportedly undergone complete tumor resection as reported by Natarajan et al. [18]
Surgery for skull base meningiomas faces a tough decision between performing an aggressive tumor resection, which carries a high risk of neurological complications, or partial removal which has a lower morbidity rate but a higher chance of tumor progression. Therefore, it is important to have additional adjunctive treatment of the tumor's remnant particularly when planned surgical/GKRS cooperation is considered, to optimize the GKRS option by reducing the size of the tumor mass [14, 17, 44, 45, 62]
Stereotactic GKRS is considered the most effective option for patients with small to moderately sized meningiomas, typically those that are less than 3 cm in diameter or <10>
In a large meta-analysis series of 2065 patients with cavernous sinus meningioma, Sughrue et al.2010, reported that those who had undergone primary stereotactic radiosurgery (SRS) demonstrated greater tumor control rates compared with patients who had undergone either complete or partial resection. In addition, the rate of postoperative cranial nerve deficits was greater in the patients with previous resection compared with primary stereotactic radiosurgery [21]
Although previous publications have found that radiosurgery was associated with favorable tumor control rates and acceptable morbidity in the first 5 years after GKRS, insufficient long-term outcome data exist. [3,9,14,22,23,24,25, 28, 37,39]
We report a tumor control rate at the last follow-up of 88.7% (n 94/106) at a median follow-up of 13 years and a median treated tumor volume of 4cc (range 0.7-10 cc). Lost tumor control and progression were reported in 11.3% (12/106) patients at a median follow-up period of 5.4 years (range 4-10) and a median treated tumor volume of 11.9cc (range 8.7-16.4). Multivariate analysis was carried out using the Cox proportional hazards regression analysis including multiple covariates confirmed tumor volume as a significant prognostic tumor control predictive factor of a P value (<0>
Skull base meningioma volume is a significantly complicated issue for stereotactic radiosurgery as larger tumors are associated with a higher risk for radiation-induced edema, hence tumor volume is generally seen as the most complicating factor in stereotactic radiosurgery. A recurring question concerns the largest possible volume that can be treated with stereotactic radiosurgery safely. This volume may differ depending on the tumor's location. Petro-clival meningiomas with volumes of 8cc and larger showed a significantly increased risk for tumor progression. [8] In cavernous sinus meningioma, the complication rate was considerably higher (21% vs. 3%) in meningiomas larger than 9.4 cc [31]. DiBiase and colleagues [20] reported a 91.9% 5-year disease-free survival for patients with meningiomas less than 10 cm3 as opposed to 68% for larger tumors.
Excellent tumor control rate with stereotactic radiosurgery has been reported by Kondziolka et al, for meningiomas up to a diameter of 3.0 cm or a volume of 7.5 cm3.[32] Likewise, other authors have found excellent local control and fewer radiation-related complications associated with the treatment of smaller meningiomas. [29, 30, 35, 36, 46, 47, 59]
Tumor Control: In the current study tumor reduction was reported in 19.1 % (n 18/94) and unchanged in 80.9% (n 76/94) of patients. Tumor progression was observed in 12 patients (11.3%) and was detected at a median of 5.4 years (range 4-10.3) after GKRS. The analysis of 3768 meningiomas in the European retrospective multicenter meningioma study documented five-and 10-year progression-free survival rates were 95.2% and 88.6%, respectively. [49]
Kondziolka et al. 2016 reported 53% of patients had residual or recurrent tumors after initial surgical resection at an interval of 10 or more years after GKRS, long-term tumor control rates were sustained. [42] This finding supports the present study's conclusion that tumor progression despite radiosurgery will typically be detected in the first decade after the procedure.
The North American Gamma Knife Consortium published actuarial progression-free survival rates of 84% at 10 years after Gamma Knife treatment of Petro clival meningiomas in a multicenter study of 254 patients [61].
Cohen-Inbar in a study of 189 parasellar meningioma patients treated with GKRS reported local tumors control in 88.1% in a series with a median follow-up of 8.5 years [1].
The documented local tumor control rate following GKRS treatment for benign skull base meningioma reported in this study was 88.7% at a median follow-up period of 13 years, which is slightly lower than control rates that have been published with a shorter observation time [46, 47, 50, 51], most probably because of the longer duration of follow-up. Generally, local control rates are slightly lower in series with long observation periods [1, 2, 4, 34] and are close similar to the tumor control rate (88.7%) after =>12 years follow-up found in the present study.
Clinical Outcomes and Complications: Clinical control (Improvement and unchanged) in pre-existing neurological and cranial nerve deficits was documented in 87.7% of patients (93/106). Clinical improvement was in the majority of patients who had achieved tumor reduction in the last control MRI (n 16/18 patients). Flannery et al. [8] argued that the pressure relief associated with tumor regression was a possible mechanism explaining the observed improvements.
In our study diplopia was the most common symptom to improve in 60% n (n 15/25) reporting improvement of pre-existing diplopia. Moreover, trigeminal symptoms improved in 27% (n 6/22). Nicolato et al. [45] reported that 60.5% of their patients who had undergone adjuvant SRS reported improvements in CN deficits. Hasegawa et al. [26] reported symptom improvement in 34% of their patients who had undergone adjuvant GKRS. In a long-term study after Gamma Knife treatments, Kondziolka reported that 94% of asymptomatic patients remained asymptomatic [42].
We observed a new onset of trigeminal neuralgia developed in one patient, additional trigeminal paresthesia in 4, deterioration of serviceable hearing in 2, and progressive deterioration of visual field in 2 patients with anterior clinoidal meningiomas. One patient developed new facial nerve palsy, one had increased motor weakness, and one developed an ataxic gait. Transient peritumoral edema was detected in 4 cases post-treatment, two of them developed a new onset of seizure activity. In 8 out of 13 patients who developed later clinical deterioration, the symptoms were related to tumor recurrence and progression.
The present data revealed a clinical long-term management risk of 12.3% (which was slightly higher than reported in comparable series with short-term follow-up), but the majority of side effects (8/13) were unrelated to the GKRS treatment and appeared to be associated with tumor recurrences. Long-term follow-up usually unveiled late complications and treatment-related morbidity of GKRS as radiation treatment modality. Similar to the present study, Starke et al. reported that tumor progression was present in 64% of patients with new or worsening neurological decline [61]
The limitations in the present study; include those inherent to the nature of retrospective data collection and the small studied number of patients. The current analysis comprises one of the longest available follow-up investigations in a larger series after stereotactic radiosurgery of skull base meningioma. It documents a persistent high local tumor control after Gamma Knife treatment, which is slightly lower than in published observations with shorter follow-ups.
The current retrospective study provides => 12-year follow-up and comprises one of the long-term follow-up studies of GKRS-treated skull base meningiomas. Tumor control from GKRS can accomplished with an acceptable low incidence of neurological deficits and related neuropathies. In a planned surgical/GKRS cooperation, the need for aggressive tumor resection could be reduced as stereotactic radiosurgery provides a documented long-term control of tumor residuals. Tumor volume at the time of GKRS is statistically significance and a reliable long-term predictor factor of tumor control. The long natural history of benign skull base meningioma's slow progression and unpredictable growth necessitates a long observation before any final conclusion regarding GKRS treatment outcome.
(cc) Cubic centimeter, (CN) cranial nerve, (GKRS) Gamma Knife Radiosurgery, (PPD) Peripheral prescription dose, (SRS) Stereotactic Radiosurgery, (TV) Tumor volume, (WHO) World Health Organization.
Ethics approval, consent to participate and consent for publication. ‘Not applicable'
Availability of data and material. Patient’s retrospective data are available
Retrospective study for this type of study formal consent is not required, it does not contain any studies with human participants"
Competing interests: The authors declare that they have no competing interests, and certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial in the matter or materials discussed in this manuscript. We declare that this is an original article.
No funding was received for this research.
All authors read and approved the manuscript.
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
