
Research Article | DOI: https://doi.org/10.31579/2578-8965/157
1Obstetrics and gynecology department - Faculty of Medicine Helwan University
2Obstetrics and gynecology department - Faculty of Medicine Ain shams University
3Radiodiagnosis department - Faculty of Medicine Ain shams University
4Obstetrics and gynecology department - Ahmed Maher Teaching hospital
*Corresponding Author: Walaa E. Ahmed, Obstetrics and gynecology department - Faculty of Medicine Helwan University.
Citation: Walaa E. Ahmed, Rania G. Elskaan, Mai M.K. Barakat, Heba M. Khattab, Mortada E. Ahmed, (2021), A Simple Procedure to Decrease the Pain Perception of the Patients during Hysterosalpingography; A Prospective RCT, J. Obstetrics Gynecology and Reproductive Sciences, 5(1) DOI:10.31579/2578-8965/157
Copyright: © 2021, Walaa E. Ahmed. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 January 2021 | Accepted: 20 February 2021 | Published: 26 February 2021
Keywords: counseling; education; hysterosalpingography; infertility; instruments; pain
Objectives: Hysterosalpingography (HSG) is a standard procedure to check for uterine and tubal causes of infertility. However, many women are afraid of the potential pain associated with it. This study aimed to assess the impact of visualizing instruments used during HSG on the pain perception of the infertile patients.
Patients and Methods: This prospective randomized control trial was done on 60 patients with infertility and was scheduled for an HSG at Ain Shams University Hospital from July to December 2020. Patients were randomly assigned into two groups. Group I (30) patients were verbally counseled about the procedure, while Group II was advised with a visual and full explanation of each instrument in the HSG set. Patients in both groups rated their expected pain severity using a visual analog scale (VAS) before HSG. Five minutes after the procedure, perceived pain severity was evaluated using VAS.
Results: There was no statistically significant difference in expected pain, perception before the HSG in the two groups (6.8±1.47 vs 6.7±1.46, Pless than 0.05). There was a statistically significant decrease in pain perception after HSG in Group II than in Group I (1.2±0.4 vs 6.6±1.54, Pless than0.001).
Conclusion: Visualization of instruments used in HSG potentially reduces pain perception and positively affects patient compliance.
Infertility refers to the inability to conceive a pregnancy after one year or more of regular unprotected sexual intercourse [1]. Tubal factor infertility is responsible for almost one-third of all cases of female infertility [2]. The hysterosalpingography (HSG) is considered the gold standard for the diagnosis of the tubal factor of infertility [3].
HSG can cause significant pain. According to several studies, 84% of patients reported moderate to severe pain after undergoing HSG [4]. The most intense pain occurred during dye instillation. Fortunately, the pain typically subsides within 5-10 minutes. However, patients often describe the experience as uncomfortable [5-7]. The pain associated with HSG is a concern, as it could negatively impact patient cooperation, potentially limiting the use of HSG as a diagnostic tool in infertility work-up [8,9].
The release of local prostaglandins due to cervical traction, uterine cavity stretching, and peritoneal irritation by the contrast agent initiates uterine cramps and consequently causes pain [10, 11]. Previous studies have presented pharmacological and technical strategies for improving the pain experience, such as paracervical or intrauterine lidocaine, different analgesics, a metal cannula versus balloon catheter, and water-based compared to oil-based contrast media [11-13].
In addition to the anatomical and physical factors mentioned above, anxiety caused by uncertainty and unfamiliarity during invasive gynecological procedures plays a role in pain perception. Anxiety activates the adrenergic system, where epinephrine release produces hyperalgesia [4].
Non-pharmacological methods, such as guided imagery, music therapy, hypnosis, and distraction, can improve pain experience during painful procedures [14,15]. Education and counseling are effective in reducing anxiety and pain reduction [4]. Proper counseling and education before HSG could enhance comfort and prepare patients psychologically. This consequently improves the patients’ experience and reduces pain perception when undergoing HSG [16].
This study aimed to assess the impact of visualizing instrument sets used during Hysterosalpingography on perceived pain.
Patients and methods
This prospective randomized control trial was conducted on 60 patients with infertility scheduled for an HSG at Ain Shams University Hospital from July to December 2020. The institution review board approved the study proposal, which complied with the Declaration of Helsinki.
Inclusion criteria: women with the inability to conceive after one year of unprotected intercourse and seeking fertility. Exclusion criteria included infertile women refusing to participate and women refusing to sign the consent form.
Primary outcome of the study: The VAS score pain perception after doing the HSG.
Secondary outcome: VAS score of expected pain from the procedure.
Sample Size calculation: the sample size was calculated using the STATA program, statistical software commonly used for data analysis. The type-1 error, which represents the probability of rejecting a true null hypothesis, was set at 0.05, and the power, which indicates the probability of rejecting a false null hypothesis, was set at 0.9. These values were chosen to ensure that the study had a high level of statistical significance. In addition, previous research conducted by Gulten et al. (2020) was used to determine the minimum sample size needed for this study. Their research indicated that a minimum of 30 cases per group was needed to ensure sufficient power to detect meaningful differences between the studied groups.
Methodology
The study recorded the patient's age, BMI, type, and duration of infertility. All patients underwent a thorough examination, which included basic hormonal profiling (follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin, and thyroid-stimulating hormone (TSH)), mid-luteal serum progesterone, and day-2 ultrasound. Semen analysis was also conducted as part of the infertility work-up.
The HSG was performed from day 5 to day 10 of the menstrual cycle, and participants were allocated into groups (I) and (II). Candidates were randomly assigned to two groups using a computer-generated sequence with a 1:1 allocation. Each candidate received an opaque sealed envelope with either verbal or visual counseling for the HSG. The patients in group (I) underwent HSG after receiving the usual care (defining the purpose of HSG, its benefits, and verbal explanation of the procedure). The patients in group (II) underwent HSG after education and counseling, aided by visualization of the HSG instrument set.
In group (II), the purpose and benefits of HSG in infertility treatment were explained. The procedure steps were demonstrated using instruments to normalize expectations and alleviate unfamiliarity. The patient was shown the smooth edges of the Cusco speculum, non-traumatic serrations of the vulsellum, and the small fenestrated end of Rubin's cannula. The colorless and water-like characteristics reassured the patient of the dye to be injected.
Procedure:
HSG was performed after counseling both groups. The cervix was fixed with vulsellum, and Rubin's cannula was applied, through which 10 ml of water-soluble contrast medium was injected. Radiographic images of the uterus and fallopian tubes were obtained before and after the dye injection. Prophylactic doxycycline was prescribed.
Patients in both groups rated their expected pain severity using a visual analog scale (VAS) before HSG. Five minutes after the procedure, perceived pain severity was evaluated using VAS. Pain severity was presented as a point on a continuous line from 0 to 10, with 0 representing no pain and 10 representing excruciating pain. The VAS score was determined by measuring the distance in centimeters (to the nearest 0.1 cm) of the marked point from the 0 edges.
Statistical analysis: SPSS software (version 21.0; IBM Corp, Armonk, NY, USA) was used for statistical analyses. Numerical parametric variables were described as means and standard deviations, and categorical variables as numbers and percentages. Independent t-test was used to compare quantitative variables, whereas paired Student’s t-test was used to analyze differences between two independent groups. For parametric data (SD less than 50% mean), the significance level was set at 0.05.
Sixty patients were included in the study; Figure 1 shows the flow chart of the patients. Table 1 shows the different demographic criteria of all patients, including type and duration of infertility. There was no statistically significant difference between the two groups.
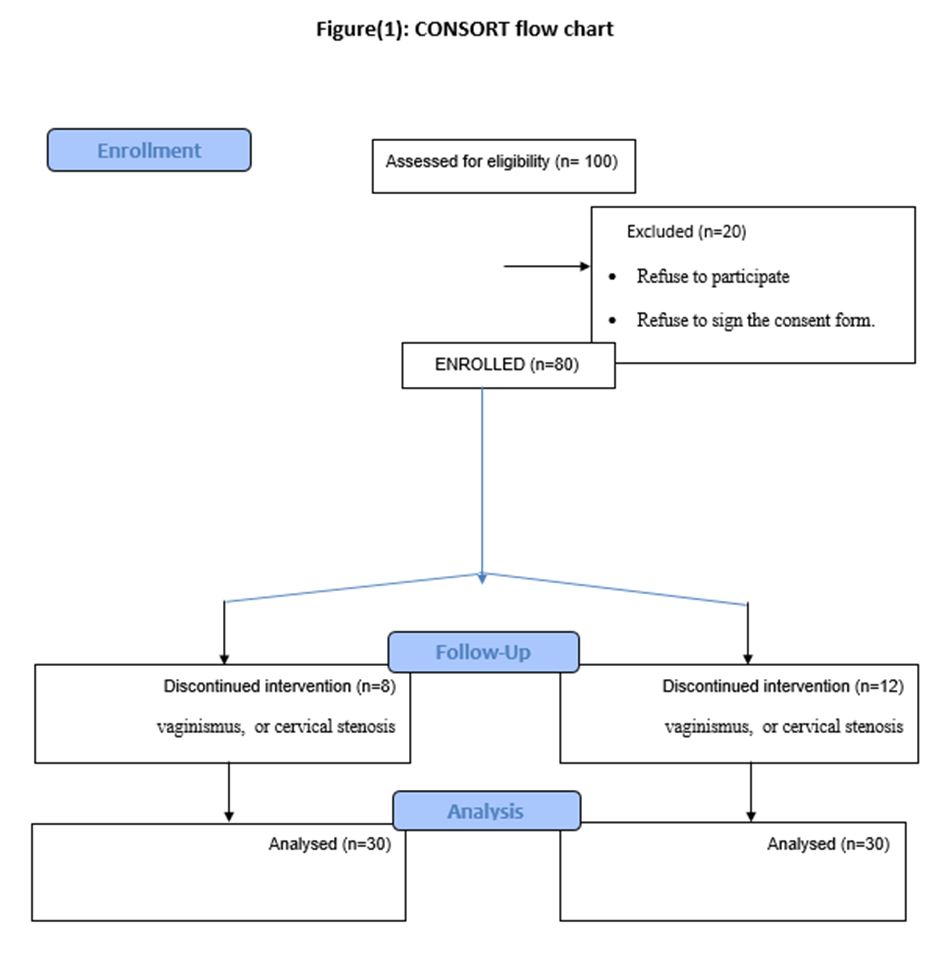
Table 1: The demographic characteristics of the two study groups
| Group (I) (n=30) | Group (II) (n=30) | P value | |
| Age (years) | 30.2± 6.8 | 28±7.2 | 0.382 |
| BMI (Kg/m2) | 28±4.5 | 27.8±4.8 | 0.951 |
| Primary infertility | 17 (56.66%) | 18(60%) | 0.332 |
| Secondary infertility | 13(43.44%) | 12(40%) | 0.352 |
Data are presented as mean ± standard deviation or numbers (n) and percentages (%)
Table 2 shows no statistically significant difference between the two groups regarding the pain expectation before performing the HSG (P>0.05). However, there was a statistically significant decrease in VAS score in Group II, where the patients received verbal and visual explanations of the HSG instruments.
Table 2: VAS scores before and after HSG in the 2 study groups
| VAS | Group (I) (n=30) | Group (II) (n=30) | T a | P - value |
| Expected pain before HSG | 6.8±1.47 | 6.7±1.46 | -0.259 | 0.642 |
| Percieved pain after HSG | 6.6±1.54 | 1.2±0.4 | -29.187 | 0.001 |
| T b | - 2.17 | - 29.1 | - | - |
| P - value | 0.17 | less than 0.001 | - | - |
a Independent t-test
b paired t-test
Our results and their interpretation
Our study showed no statistically significant differences between 2 groups regarding the demographic criteria or type of infertility. There was no statistically significant difference in expected pain perception before the HSG in the two groups (6.8±1.47 vs 6.7±1.46, Greater than 0.05). There was a statistically significant decrease in pain perception after HSG in Group II than in Group I (1.2±0.4 vs 6.6±1.54, Pless than0.001).
The pain experienced during Hysterosalpingography (HSG) can be a significant factor as it may restrict the use of HSG as a diagnostic tool in infertility investigations. It is essential to educate and counsel women undergoing this procedure. Visualizing the instrument sets used in HSG might help normalize their expectations and decrease the perceived pain during HSG. By providing detailed information about the procedure, women can be better prepared, and their anxiety levels can be reduced, leading to a more comfortable and less stressful HSG experience.
Comparison of our results to similar studies
Similar to our results, Gluten et al., 2020 performed RCT on 105 patients. They were randomly assigned to either the intervention (52) or control (53) groups. Before the hysterosalpingography procedure, both groups were assessed using the State-Trait Anxiety Inventory and a visual analog scale. The intervention group received individual learning and counseling sessions on the HSG procedure. The control group received standard care. Comparing the intervention and control groups showed that the education and counseling provided before the procedure significantly reduced the level of pain and anxiety experienced by women. They showed a significant reduction in pain scores compared to the control group who received routine care (mean pain scores of 3.04 ± 2.38 vs. 6.40 ± 2.29, respectively). Furthermore, a significant positive correlation was observed between pain and anxiety after training in the intervention group [16].
Few studies have shown that counseling and education are effective in reducing pain during invasive procedures in female patients. Studies presented by Balci et al. [17] and Walsh et al. [18] reported that patient education effectively reduced pain in patients undergoing amniocentesis and colposcopy, respectively.
In contrast to our study, La Fianza et al. 2014 randomized their patients into two groups: control (n=108) and intervention (n=109). Both groups filled out questionnaires before and after HSG, and pain was scored using a visual analog scale. The intervention group received personalized counseling 48 hours before HSG. Results showed that the intervention group had lower anxiety and depression scores than the control group. The intervention was an independent predictor of the difference in Z-SAS scores before and after HSG. Their study was the first to evaluate the efficacy of a single education and counseling intervention in reducing anxiety in a diagnostic setting. The study determined that education and counseling on their own did not prove to be enough to manage pain levels. According to the study, those who were in the intervention group that received education and counseling did not show any decrease in pain scores compared to those in the control group who were receiving usual care [19].
The strengths and limitations of our study
The strength of our study is that it is the first study to be performed on Egyptian women. Our study had limitations. The pre-procedure assessment didn't evaluate anxiety and pain scores using standardized inventories. Also, the data presented are patient-dependent, and other factors causing pain during HSG were not fully evaluated. Furthermore, more extensive studies are needed to confirm these results.
Clinical implications of our study: By providing HSG verbal and visual education and counseling and handing out brochures to every patient, pain and anxiety during the HSG procedure can be decreased.
Recommendation for further studies: Multi-centric studies are needed to evaluate the effect of education and visual counseling of patients regarding the HSG procedure.
Visualizing HSG instrument sets can reduce pain, improve satisfaction and increase compliance of the patient during the HSG procedure.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
