
Case Report | DOI: https://doi.org/10.31579/2690-1919/413
1 Department of General Surgery and Trauma, Fellow in Trauma, Acute care surgery and General Surgery, Hôpital Edouard Herriot/Hospices Civils de Lyon, University of Claude Bernard Lyon 1, 5 Place D’Arsonval, Lyon 69003, France. ORCID https://orcid.org/0000-0001-9729-1657
2 Department of Diagnostic and Interventional Radiology, Hôpital Edouard Herriot/Hospices Civils de Lyon, University of Lyon, 5 Place D'Arsonval, Lyon, 69003, France.
3 Third year Medical Student, FGSM3, University of Claude Bernard Lyon 1 (participation in this article as part of Biomedical Research Teaching Unit), Anatomy, Imaging and morphogenesis. 5 Place D’Arsonval, Lyon 69003, France
4 Department of General Surgery and Trauma, Military General and Trauma Surgeon, Hôpital Edouard Herriot/Hospices Civils de Lyon, 5 Place D’Arsonval, Lyon 69003, France.
5 University Professor and Senior Consultant in Trauma, Acute Care Surgery and General Surgery. University of Claude Bernard Lyon 1/Hôpital Edouard Herriot/Hospices Civils de Lyon, 5 Place D’Arsonval, Lyon 69003, France. 5 Place D’Arsonval, Lyon 69003, France
*Corresponding Author: Sara Al Awad, Department of General Surgery and Trauma, Fellow in Trauma, Acute care surgery and General Surgery, Hôpital Edouard Herriot/Hospices Civils de Lyon, University of Claude Bernard Lyon 1, 5 Place D’Arsonval, Lyon 69003, France.
Citation: Sara Al Awad, Romain l’Huillier, Mr. Hugo Achaintre, Cedric Scheiwe, Olivier Monneuse (2024), A Silent Journey: Uncovering Congenital Tracheo-Oesophageal Fistula in Adults, J Clinical Research and Reports, 17(1); DOI:10.31579/2690-1919/413
Copyright: © 2024, Sara Al Awad. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 September 2024 | Accepted: 27 September 2024 | Published: 31 October 2024
Keywords: : thoracic surgery; extra corporeal circulation; esophagus; tracheo-oesophageal fistula
Tracheo-Oesophageal fistula (TOF) is a widely known congenital anomaly, frequently associated with oesophageal atresia, which requires an urgent surgical correction during infancy. Congenital TOF rarely presents in adults. However, this diagnosis has been observed recently in certain patients as described in the literature explained in this article. Adults suffering from it experience chronic chest infections and chronic cough, usually attributed to other pathologies rather than the persistence of a TOF. This article reports the case of a young 22-year-old lady who since the age of five has been diagnosed with a psychogenic cough and was given anxiolytics and inhalers without any amelioration of her clinical state. An acute pneumopathy leads to a Computed tomographie, which allow us to suspect a TOF. A multidisciplinary approach and a thorough surgical plan are of great importance after confirming such diagnosis to solve this anatomic anomaly.
TOF : Tracheo-oesophageal fistula
CT : Computed tomography
A 22-year-old lady not known to have any medical comorbidities presented to our tertiary hospital of trauma and acute care surgery after being referred from a local secondary facility with a suspicion of a TOF. The patient explained that at the young age of five she started to develop a cough which is not associated with food or has any specific triggering factors. At the age of five, she lost her grandmother, and physicians theoretically diagnosed her cough to be psychological due to sadness.
Initially, she consulted a secondary healthcare facility because her cough became forceful and associated with important bouts of hypoxia. According to their clinical investigations, she was found to have hypoxemic pneumopathy along with an oxygen saturation of 94% under 5 Liters of oxygen via facemask. She had an injected Computed Tomography (CT) revealing a large slit-like communication between the base of the trachea and the oesophagus with a diameter of 1 cm at the level of the 3rd thoracic vertebra (Figure 1). CT also showed aspiration pneumonia in the left lower lobe. The Virtual endoscopic reconstruction of the CT (Philips IntelliSpace Portal®, Philips Eindhoven, The Nederlands) is shown in Figure 2
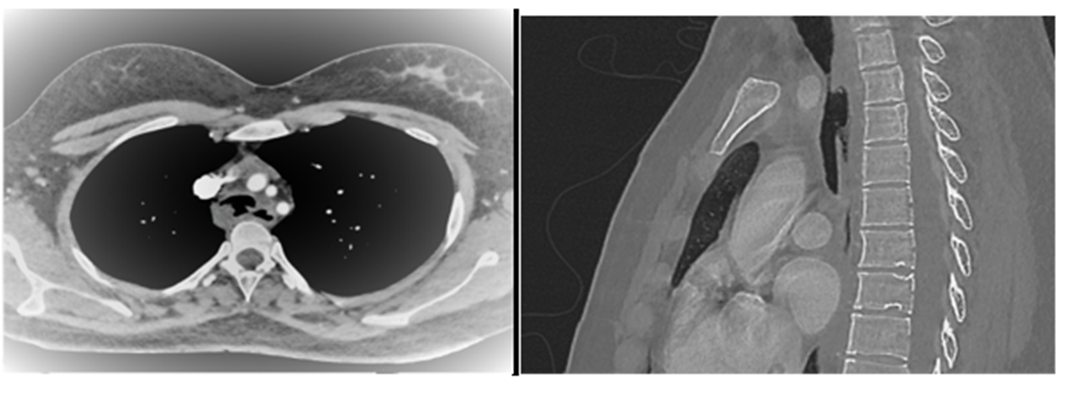
Figure 1 : Axial and Sagittal CT scan view of the Tracheoesophageal Fistula
The patient was immediately referred to our tertiary centre intensive care unit where she was kept nil orally and given parenteral nutrition, corticosteroids, nebulisers, antibiotics, anxiolytics, fluoxetine chloride and amitriptyline.
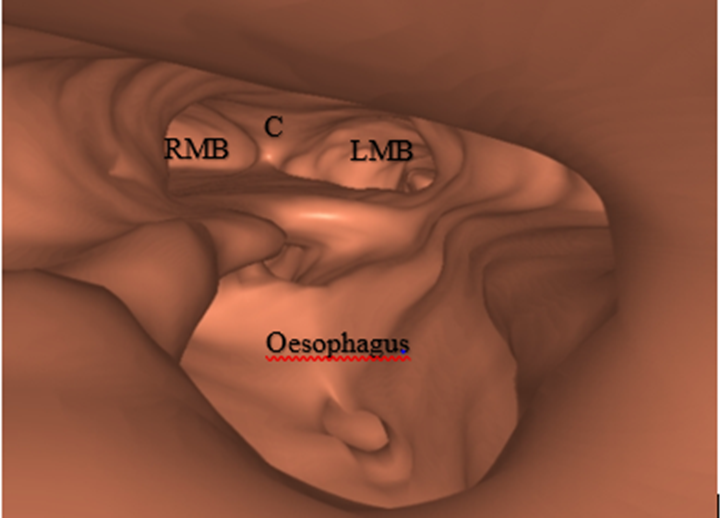
Figure 2: Virtual endoscopic reconstruction: Oesophagus, RMB: Right Main Bronchus, C: Corina, LMB: Left Main Bronchus
A multidisciplinary discussion with complete transparency was conducted, inclusive of General surgeons, Anesthetists, Ear nose and throat specialists, Gastroenterologists, Dietitians, Respiratory physiotherapists, psychologists and Cardiothoracic surgeons
The patient also underwent an oeso-gastrosduodenoscopy (OGD) and a bronchoscopy portraying a large voluminous loss of substance between
the oesophageal and the tracheal wall of around 16 cm to 20 cm from the oesophageal mouth with a wide length of approximately 4 cm. The endoscopic examination was poorly tolerated, with a very low oxygen saturation of less of 50%. Endoscopic management was excluded due to the large fistulous tract (Figure 3).
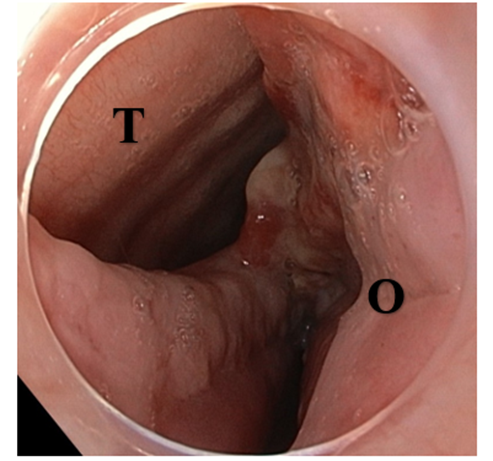
Figure 3: Tracheoesophageal Fistula viewed by the Oeso-gastroduodenoscopy. O: Oesophagus, T: Trachea
The patient was optimised in terms of her nutritional status and her respiratory symptoms, then transferred to our neighbouring Cardiothoracic Center for a combined surgical repair by our General surgeons and Cardiothoracic Surgeon colleagues with an extracorporeal circulation on standby.
The patient underwent a right postero-lateral thoracotomy and a large important fistula was identified with its distal end found at 2 cm above the carina and its proximal limit at the thoracic outlet
The thoracic surgeons faced difficulty accessing their work field with the presence of the intubation tube, so they opted to extubate the patient and they selectively intubate the left bronchus through the fistula with a Montandon tube. It was a successful initiative that allowed complete repair of the trachea and withdrawal of the broncheal intubation into the trachea.
Closure of the esophagus was done with interrupted sutures; closure of the trachea with a heterologous pericardium patch, the third rib was excised, followed by the interposition of a latissimus dorsi flap between the esophagus and trachea, finishing off the surgery with thoracic drainage kept on continuous suction.
The post-operative period was marked by an inflammatory process due to a deep-seated thoracic abscess and a small oesophageal fistula which was drained by interventional radiologists. Her evolution was remarkable and she tolerated fractionated soft diet really well. After a reassuring thoracic CT scan, her pleural drains were removed with multiple assessments carried out by radiographical images and she was discharged home with a satisfying follow-up including another CT scan a month later.
Tracheo-oesophageal fistula is a rare disease in adulthood and patients usually live a normal life with the history of multiple aspiration pneumonias, respiratory infections throughout their lives, which goes misdiagnosed or missed due to the lack of vigilance and further investigative methods.
TOF without esophageal atresia exists in 4% of all congenital anomalies. In recent years, it has been observed and properly diagnosed in adulthood with the evolution and low threshold of carrying out CT scans, especially in centers of high expertise. Most patients present the Ono sign, an uncontrollable cough after deglutition. Many will complain of recurrent chest infections, and some will have easier swallowing with postural change.
Saxena and Tam described the reasons for which patients present with late manifestations and a delayed diagnosis. Firstly, the fistula having an oblique path (starting higher up in the trachea with a downwards path into the oesophagus. Secondly, the presence of a membrane blocking the lumen of the fistula. Thirdly, the presence of a valve mechanism and lastly due to spasms of the fistulous tract [1].
The diagnosis is based on bronchoscopy, esophagoscopy or barium swallow and it needs a strong suspicion of tracheoesophageal fistula. Sometimes, it is an incidental finding during intubation [1].
Congenital TOF are usually short and small in caliber unlike our patient who presented a long and very wide fistula.
Management of a fistula should be discussed with all the concerned specialists and care should be taken while planning out the intervention as we are working with two of the largest systems in the body.
TOF can also be acquired. In acquired they can be due to malignant tumors or benign illnesses. There is also a group of iatrogenic TOF which manifest post traumatic intubation and prolonged tracheostomies.
Its diagnosis remains the worst prognostic factor due to many physicians rarely considering it and there is no reliable index of suspicion for adults with chronic cough. The eldest to have been diagnosed with persisting TOF is 79 years of age [2].
Hon Chi Suen [2] has reported 3 cases of persisting TOF in adults over the last 16 years. All 3 cases were misdiagnosed initially, and one case has a concomitant Esophageal Cancer associated with congenital TOF.
Another case is a 4-year-old patient who has been misdiagnosed as severe reflux requiring Nissen fundoplication and gastrostomy. He persisted to have the severe respiratory symptoms and despite CTs and OGD the TOF has been missed leading doctors to undo the ‘tight’ Nissen fundoplication and discuss a possible esophagectomy. As the patient consulted a specialized center, the radiologists and doctors immediately picked up the presence of a congenital H Type TOF confirmed furthermore with an esophagoscopy and bronchoscopy. They stated that the Fistula was very large that the bronchoscope can pass from the trachea to the esophagus easily [2].
The diagnosis of TOF can be achieved on a simple noninvasive chest CT by highly experienced radiologists, particularly when there is a high index of suspicion in the clinical examination of patients. However, the gold standard is a laryngotracheal endoscopy, in the operating room, under general anesthesia with spontaneous breathing [3]. The discovery of an adult congenital TOF is very rare and it is more often made on young people. Two other similar cases report mentioned a 15-year-old boy [4] and 22-year-old woman [1]. But there are also similar cases of older people of 59-year-old woman [5], 54-year-old man [6] and 67-year-old man [7].
Luscan R. et al proposed endoscopic guidelines for diagnosis of TOF. They mentioned the importance of assessing the recurrent laryngeal nerves (RLN) before the patient is completely sedated as there is a high risk of RLN paralysis with the surgical repair of this fistula. They present three different permeability assessment techniques: a methylene blue test, the introduction of a ureteral catheter (3 Fr) and the use of a surgical probe [3].
The treatment of TOF is based on the ablation of this communication between those two tubes. Highlighted by Chauhan SS and KIM HS, the endoscopic treatments involve fibrin glue, septal occluders and stents. Stenting is more viable and well established in patients with malignant TOF requiring a palliative approach [8,9].
Other treatments are based on a more aggressive intervention requiring a lateral thoracotomy with ablation of the fistula and application of a muscular patch like a split of the latissimus muscle between the two repaired orifices [10].
After all the involved specialists validate the surgical intervention, it is of great importance to carry it out in a highly specialized center as the patient will most likely require an intra-operative extubation with selective bronchial intubation for the trachea-oesophageal repair as it was the case with our patient and sometimes patients may require an extra-corporeal circulation.
Knowing the origin and nature of the fistula is the first and most important step in order to proceed with a successful treatment plan. Some patients may be eligible for stents and others requiring a more aggressive approach such as surgery with a muscle patch between the esophagus and the trachea. The position of the fistula is highly important in deciding between a cervicotomy or a thoracotomy, as well as in determining the most suitable muscular patch.
The choice of repair can be adapted if the region has the pectoral muscles anteriorly and the latissimus dorsi muscles posteriorly [11]. Higher fistulas can be patched using neck or cervical muscles such as the sternocleidomastoid muscle [11], the sternohyoid muscle [12] or a posterior tracheal flap.
Congenital Tracheo-oesphageal fistulas are common in newborns and is often associated with oesophageal atresia, which is surgically corrected in infancy. However, it can present without oesophageal atresia bypassing the infancy period and discovered later in adulthood as we have shown in this case report.
The use of a muscle flap when possible has been demarcated in the literature to reduce the chances of recurrence of large fistulas significantly even though the two repaired regions are at different levels. Follow up of such patients should be close and any arising respiratory symptoms should be treated with care and vigilance.
We conclude that, it is of great importance that the approach of such patients is to be taken with great vigilance and the suspicion of such diagnosis is to be confirmed meticulously. Addressing similar cases requires a multidisciplinary approach, multiple confirmatory investigations, access to extra-circulatory circulation, the ability to selectively intubate perioperatively and a well- tailored and planned surgical intervention.
Author Contributions: S. A. Literature Review, Writing, and Editing; R. L Virtual endoscopic reconstruction of radiological images and Editing; H. C. Writing and Literature review; C. S. Surgical management; O.M. Supervision, Surgical management, Editing and Mentoring.
This research received no external funding.
Informed Consent Statement: A written informed consent has been obtained from the patient to publish this paper.
Acknowledgments: We thank all volunteers who took the time to contribute to this excellent article.
None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
