
Review Article | DOI: https://doi.org/10.31579/2640-1045/013
1 Department of Neuroendocrinology, Ethiopia.
*Corresponding Author: Maryam Jahangirifar, Department of Neuroendocrinology
Citation: Maryam Jahangirifar, Hosna Gomari, Mona Moniri, Samira Behboudi-Gandevani, S M Ghazi, Ramin Khameneh Bagheri, A Review Based Analysis of Recent Developments in Acute Pancreatitis: Evaluation and Management. J. Endocrinology and Disorders, DOI:10.31579/2640-1045/013
Copyright: © 2018. Maryam Jahangirifar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 January 2018 | Accepted: 29 January 2018 | Published: 08 February 2018
Keywords: Acute Pancreatitis, Severity Scoring, Diagnostic Imaging, Management Of Gallstone Pancreatitis.
The incidence of acute pancreatitis (AP) has been increasing worldwide, but the major etiologies remain gallstones and alcohol. Several studies have reported that smoking is an independent risk factor for developing AP. Classification of AP has traditionally used the categories of mild and severe disease. However, a new intermediate category of moderately severe AP has been described with intermediate characteristics including a high incidence of local complications but a low mortality. Assessment criteria that can serve as early predictors of AP severity are often complex and not sufficiently accurate. However, several recently described criteria that rely on criteria such as the body mass index, physical findings, and simple laboratory measurements could prove useful if validated in large prospective studies. Many issues related to the therapy of AP are still unresolved. Although preliminary studies support the importance of early volume expansion for the treatment of acute pancreatitis, optimization of the amount and type of fluids will require further studies. Similarly, preliminary studies suggest that enteral nutrition might benefit patients with AP and could even be useful early in the course of disease. However, the timing and type of fluids as well as the intestinal infusion site require further study. Finally, issues related to the prophylactic use of antibiotics in patients with severe AP have not been resolved. While the process of clinical investigation moves slowly, progress has been made in clinical studies of AP.
Data from the National Center for Health Statistics have demonstrated a 100% increase in the overall hospitalization for AP in the United States during the last 2 decades.Similarly, there has been a 75% increase in admissions for AP in The Netherlands between 1992 and 2004, and this is predicted to increase by another 9.9% in 2010 Recent studies from the United Kingdom have shown a 3.1% annual increase in the overall incidence of AP, with the highest increase among women younger than 35 years. The age standardized incidence was higher among elderly people (odds ratio [OR], 1.06 per year) and in economically deprived areas (OR, 2.4 between least and most deprived).Additional evidence of an increase in the incidence of AP came from a recent meta-analysis of 18 European studies, which also showed a linear increase in the incidence of gallstone pancreatitis and an increase in mortality with age. The meta-analysis also showed that although the case fatality rate has decreased over the years, the overall mortality rate per 100,000 has been the same.
Alcohol and gallstones are the most common causes of AP. With respect to hypertriglyceridemia as a cause of AP, even though the triglyceride threshold required to cause pancreatitis has been established to be 1000 mg/dL, no correlation between the level of triglycerides and severity of AP has been found
Drug-induced pancreatitis is difficult to diagnose. The precise role of a drug in causing AP, the duration between the exposure and development of AP, the pathogenic mechanisms, and synergy with cofactors are usually not clear. On the basis of an extensive review of 1214 reports describing drug-induced AP during 50-year duration, Badalov et alclassified 120 drugs that were found to be associated with AP into 4 major classes (Class I, positive re-challenge; Class II, consistent latency; Class III, at least 2 cases in the literature without re-challenge and latency; and Class IV, single case report without re-challenge).
Antibiotic Prophylaxis in Acute Pancreatitis
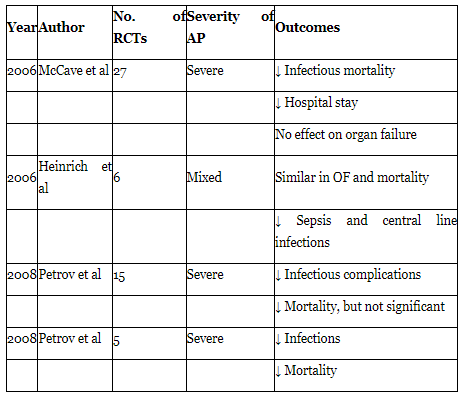
Antibiotic prophylaxis to prevent infection of pancreatic necrosis has been another controversial issue. Despite a number of clinical trials and meta-analyses, a clear consensus still does not exist. Earlier meta-analyses showed beneficial results from antibiotic prophylaxis. However, to date there are only 3 double-blind placebo-controlled trials studying role of antibiotic prophylaxis, and none of them showed any benefit in terms of prevention of infection of necrosis,
A patient complaining of sudden onset of epigastric pain radiating to the back, associated with nausea and vomiting, requires rapid exclusion of a wide range of life-threatening conditions involving the cardiovascular (myocardial infarction, ruptured, and/or dissecting aortic aneurysm) and gastrointestinal (peptic ulcer disease with perforation or bleeding, acute pancreatitis) systems. The clinician’s history and examination findings are augmented by relevant investigations in narrowing the differential diagnoses to eventually guide the management and treatment of a certain condition and its associated complications.
The incidence of acute pancreatitis in the UK is ~56 cases per 100,000 persons per year, while in the US over 220,000 hospital admissions annually are attributed to acute pancreatitis.An epidemiologic study that utilized UK and European data demonstrated an increasing incidence in all-cause acute pancreatitis.The incidence of acute pancreatitis was also noted to increase with age.The male population had an incidence that was 10%–30% higher than females.Despite a reduction in the case fatality being observed over time, the population mortality has remained largely unchanged. Of all hospital admissions with acute pancreatitis, ~20%–30% of patients have a severe course,while severe life-threatening complications will develop in ~25% of these patients. The mortality in severe acute pancreatitis can be as high as 30%, but the overall mortality in acute pancreatitis is estimated to be 5%.
Treatment
Antibiotic Prophylaxis in Acute Pancreatitis
Antibiotic prophylaxis to prevent infection of pancreatic necrosis has been another controversial issue. Despite a number of clinical trials and meta-analyses, a clear consensus still does not exist. Earlier meta-analyses showed beneficial results from antibiotic prophylaxis. However, to date there are only 3 double-blind placebo-controlled trials studying role of antibiotic prophylaxis, and none of them showed any benefit in terms of prevention of infection of necrosis,
Fluid Therapy
AP is associated with a significant amount of third space fluid sequestration. This can lead to hypovolemia and reduced perfusion pressure, which in concert with microvascular alterations can contribute significantly to the development of major local and systemic complicationsThere are very few high quality human studies that have assessed the role of fluid management in AP, and a recent review by us has addressed these issuesWe have recently shown that aggressive fluid therapy (33% or more of the initial 72-hour fluid volume within the first 24 hours of hospitalization) is associated with a significantly lower OF rate compared with nonaggressive therapy (7.1% vs 22.6%; P < .03).The other area, besides volume of fluid that needs further insight is the type of fluid (crystalloid or colloid) for resuscitation. The most recent American Gastroenterological Association technical review on AP recommends crystalloids in most cases, and that colloids (packed red blood cells and albumin, respectively) be reserved for special situations like a hematocrit drop to less than 25% and a serum albumin drop to less than 2 mg/d It should also be kept in mind that very aggressive fluid therapy might have its own problems like fluid overload, which might be detrimental to patients with cardiovascular problems and to those with acute respiratory distress syndrome.
Nutrition
AP is a hypercatabolic state, and early nutrition should be initiated with a therapeutic intent. In patients with mild AP, oral feeding can be considered within 24–72 hours of disease onset. A recent study has shown that initiating re-feeding with low fat soft diet is safe and can reduce hospitalization, when compared with clear liquid diet.
Early nutrition should also be considered in patients with SAP. Prolonged fasting can potentially lead to bacterial translocation across the gut barrier and subsequent local and systemic complications.Contrary to the earlier notion of pancreatic rest and parenteral nutrition (PN), data from recent studies have driven a paradigm shift in nutritional management in SAP toward enteral nutrition (EN). However, adequately powered studies to evaluate the appropriate timing for initiating EN are lacking
Surgical Intervention in Acute Pancreatitis
All patients with acute gallstone pancreatitis should have imaging of the common bile duct to assess for choledocholithiasis Preoperative imaging utilizes noninvasive methods such as transabdominal ultrasound and/or MRCP, while intraoperative cholangiography provides real-time imaging of the common bile duct. Management of choledocholithiasis is reliant upon availability of local expertise and can be broadly classified into 1) the single-stage approach – laparoscopic or open cholecystectomy with intraoperative cholangiography and common bile duct exploration, or 2) two-stage approach – preoperative ERCP with or without ES followed by laparoscopic or open cholecystectomy. There is no significant difference in the morbidity, mortality, retained stones, and failure rate between the two management approaches for choledocholithiasis.
Local complications of acute pancreatitis include pancreatic necrosis with or without infection, pancreatic pseudocyst formation, pancreatic duct disruption, and peripancreatic vascular complications. These local complications can be managed using a combination of endoscopic, radiologic, and surgical techniques, and have been reviewed previously. Open surgical debridement requires multiple laparotomies and is consequently associated with a high postoperative morbidity. However, surgical techniques have evolved to become minimally invasive, which may be associated with better outcomes.
Acute pancreatitis is frequently encountered on the emergency surgical take. Once the diagnosis is made, clinical efforts should simultaneously concentrate on investigating for the underlying etiology and managing the condition by anticipating its complications, which can be aided by using any of the severity scoring systems described. Management of acute pancreatitis is largely supportive. There is still no consensus on the ideal type and regimen of fluid for resuscitation, but goal-directed fluid therapy is associated with better outcomes. Early enteral nutrition modulates the inflammatory response and improves outcomes by decreasing infective complications of acute pancreatitis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
