
Research Article | DOI: https://doi.org/10.31579/2578-8965/158
Department of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University. Cairo, Egypt.
*Corresponding Author: Rania G. El-Skaan, Department of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University. Cairo, Egypt.
Citation: Rana H. Seif, Basant M. Elsayed, Samiira M. Maalim, Bayan M. Badraway, Sara O. Elbastawisy, et al., (2023), A Retrospective Analysis of Antepartum Haemorrhage at Ain Shams University Hospital, J. Obstetrics Gynecology and Reproductive Sciences, 7(2); DOI:10.31579/2578-8965/158
Copyright: © 2023, Rania G. El-Skaan. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 February 2023 | Accepted: 27 February 2023 | Published: 22 March 2023
Keywords: antepartum haemorrhage; APH, placenta previa; accidental haemorrhage; abruptio placenta; placenta accreta; maternal morbidity and mortality; neonatal morbidity and mortality; antepartum complications
Background: Antepartum haemorrhage (APH) can be described as a malicious phenomenon that is lying in wait to send their patients straight to the grave if it was not taken seriously from the start. Therefore, it has always been considered one of the commonest leading causes of maternal and perinatal morbidity and mortality. APH is defined as any bleeding from or into the genital tract after the period of viability and before the delivery of the baby. The aim of the current study was to assess maternal and neonatal outcome in patients with antepartum haemorrhage, prevalence of their different types, the associated risk factors and complications, and the different lines of management that were implemented.
Methods: The present study was a retrospective observational study undertaken in the Obstetrics and Gynaecology department of Ain shams University Maternity and Women's Hospital, during a period of 3 months from August 1st, 2020 to October 31st, 2020. Total number of patients recorded were 99 cases of antepartum haemorrhage who have fulfilled the inclusion criteria. Data was recorded on the MS excel sheet for further analysis and processing using statistical package for social science, version 20.2 (SPSS inc., Chicago, Illinois, USA).
Results: Total 3063 cases were registered during this period out of which 99 presented as APH and incidence of APH was found to be 3.23%. Placenta previa (67.68%) was the most common type of APH followed by placenta accreta (34.34%) and accidental haemorrhage (30.30%). The mean age of most women was 30.53±6.08 years and the mean gestational age was 34.96±2.96 weeks. High risk factors included previous Lower Segment Caesarean Section (LSCS), previous Dilation and Curettage (D&C), hypertension, multiple pregnancies and mal-presentations. Most of the patients underwent preterm LSCS (61.62%) but 8.08% performed caesarean hysterectomy. Neonatal Intensive Care Unit (NICU) admissions recorded were 26.26%. Most fetal complications were due to prematurity. 66.6% of the patients required blood transfusion. Overall perinatal mortality was 5.05% and maternal mortality was zero.
Conclusion: Women with APH have to be considered as high-risk pregnancy and need institutional supervision. Early diagnosis and management of the condition along with trained team of doctors are considered key strategies in avoiding APH related maternal, fetal and neonatal complications.
Antepartum haemorrhage (APH) is an obstetric emergency contributing to a significant amount of perinatal and maternal morbidity and mortality. It complicates about 2-5percentage of all pregnancies. Thirty percent of maternal deaths are caused by antepartum haemorrhage of which 50percentage are associated with avoidable factors. APH is defined as any bleeding from or into the genital tract after 28 weeks of gestation and before the period of viability. It can be classified into minor haemorrhage: blood loss less than50 ml; major haemorrhage: blood loss 50-1000 ml; massive haemorrhage: blood loss greater than1000 ml.[1]
The causes of antepartum haemorrhage can be divided into three main groups, placenta previa, placental abruption and others which include obstetrics and general causes. Placenta previa exists when the placenta is implanted wholly or in part into the lower segment of the uterus. An abruptio placentae is the condition whenever bleeding occurs due to partial or complete premature separation of a normally sited placenta before delivery [2] Other causes may be related to local lesions of the cervix and vagina, e.g., cervicitis, cervical erosion, genital tumours, vulvar varicosities, ruptured vasa previa, and heavy show. Systemic diseases like leukaemia and bleeding disorders are rare causes of APH. Placenta praevia and abruptio placentae account for almost half cases of APH.[1]
APH occurs without warning signs; thus, there is a need to identify the risk factors associated with antepartum haemorrhage to help obstetricians in the early diagnosis and treatment. These risk factors include previous APH, previous caesarean section, advanced maternal age (age greater than 35), urban/rural residence, previous termination of pregnancy (curettage), pregnancy-induced hypertension (PIH), multiparity, and multiple pregnancy.[3] Maternal complications of APH include malpresentation, premature labour, postpartum haemorrhage, shock, retained placenta. They also contribute to higher rates of caesarean section, peripartum hysterectomy, coagulation failure, puerperal infections and even death.[1]
The objective of this study was to observe the incidence of antepartum haemorrhage at tertiary care hospital and the prevalence of their different types, to study the maternal and neonatal outcome in antepartum haemorrhage and to study the associated risk factors and complications contributing to maternal and neonatal morbidity and mortality. Also, to assess the different types of management applied.
This retrospective Observational study was carried out in the department of Obstetrics & Gynecology at Ain Shams University Maternity and Women's Hospital, Cairo, Egypt. It comprised 99 cases of antepartum haemorrhage (APH) out of 3063 cases in the department. Over a 3 months period, a list of all patients that had APH from August 1, 2020 to October 31, 2020, was collected from the labour ward, and the cases notes were then retrieved from the Medical Records Department of the hospital. Inclusion criteria were patients who had APH, which included placenta previa, accidental haemorrhage (abruptio placentae), placenta accreta and others, from 26 weeks of gestation and beyond. Exclusion criteria were patients who didn’t have APH or had bleeding from the genital tract before 26 weeks of gestation. The names and hospital numbers were carefully cross-checked to ensure there was no repetition. Patients’ data such as name, age, blood group, parity, previous caesarean section or abortion, living offspring, duration of marriage, gestational age, medical and surgical history, ultrasound, diagnosis of the cause of the APH, management done to the patient, haemoglobin level, blood transfusion, Intensive Care Unit (ICU) admission, mortality, complications was recorded. Also, neonatal gender, weight, Apgar score, if he or she was under observation, if they entered Neonatal Intensive Care Unit (NICU) or were discharged with their mother’s data were all collected. Data collection was transformed into MS excel sheet. The data were analyzed using the statistical package for social science, version 20.2 (SPSS inc., Chicago, Illinois, USA). Paired sample of t-test of significance was used when comparing between related samples. P less than 0.05 was considered significant.
Statistical analysis
Data collected was transformed into MS excel sheet for further processing and analysis using the statistical package for social sciences, version 20.0 (SPSS Inc., Chicago, Illinois, USA). Quantitative data were expressed as mean± standard deviation (SD) while qualitative data were expressed as frequency and percentage. Paired sample t-test of significance was used when comparing between related samples. Since the confidence interval was set to 95percentage and the margin of error accepted was set to 5percentage, the probability (p-value) was considered significant according to the following: P-value less than0.05 was considered significant, P-value less than0.001 was considered as highly significant and P-value greater than0.05 was considered insignificant.
The present study was a retrospective analysis of ante-partum haemorrhage. It was conducted at Ain shams University Maternity and Women's Hospital. The data were recruited from patient documents of 3 months duration, starting from August 1st, 2020 to October 31st, 2020. All were diagnosed with ante-partum haemorrhage which were either accidental haemorrhage, or associated with placenta previa or placenta accreta or others.
Total number of patients who were admitted to the hospital during these 3 months was 3063 patients; 99 patients were diagnosed with ante-partum haemorrhage. So, the incidence of ante-partum haemorrhage in the current study is 3.23percentage.
Demographic distribution and baseline characteristics of the women recorded were shown in Table (1). It illustrates that the mean age of the women was 30.53±6.08 years (range 17–41 years). It also includes the total number of the different blood groups recorded and the median number (IQR) of parity calculated was 2 (1-3), while the median number (IQR) of Cesarean Section (CS) conducted was 1 (0-3). Furthermore, the median number (IQR) of the living offspring was 2 (1-3) and the mean gestational age was 34.96±2.96 weeks.
In addition, the medical history of the women comprised of hypertension, diabetes and cardiac problems which were 4.04percentage, 2.02percentage and 1.01percentage respectively. While the surgical history involved previous Cesarean Section (CS) which was 65.66percentage and previous Dilation and Curettage (D&C) which was 7.07percentage.
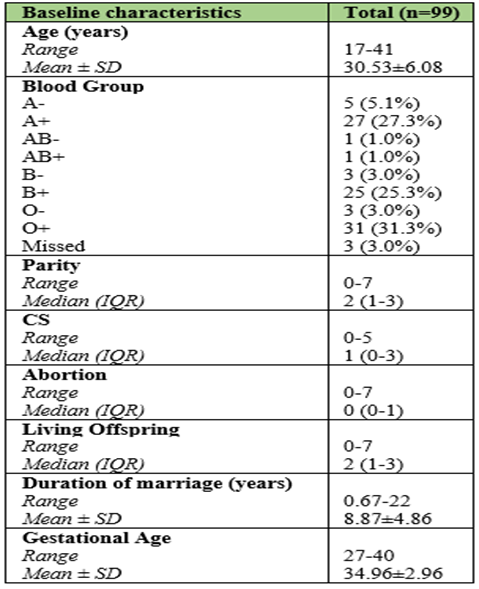
Table 1: Distribution of women according to their demographic data and baseline characteristics (n=99).
Table 2 demonstrates the incidence of the different types of ante-partum haemorrhage encountered which were: Placenta Previa 67 (67.68percentage), Accidental Haemorrhage 30 (30.30percentage), Placenta Accreta 34 (34.34percentage); and others such as, Premature rupture of membranes (PROM) 9 (9.09percentage), Established Preterm Labour 1 (1.01percentage), Fetal Distress at 36 weeks 1 (1.01percentage), Intrauterine Fetal Death (IUFD) associated with placental abruption 1 (1.01percentage), Placenta fundal anterior 1 (1.01percentage), Polyhydramnios 1 (1.01percentage), Retroplacental hematoma 1 (1.01percentage) and Threatened Preterm Labour (PTL) associated with Severe Preeclampsia (SPET) and Premature rupture of membranes (PROM) 1 (1.01percentage).

Table 2: Distribution of women according to their diagnosis (n=99).
However, table 3 elicits the incidence of different types of ante-partum haemorrhage as well but according to the ultrasound results which were Placenta Previa 53 (53.54percentage), Signs of Invasion 28 (28.28percentage) and Haematoma 5 (5.05percentage).
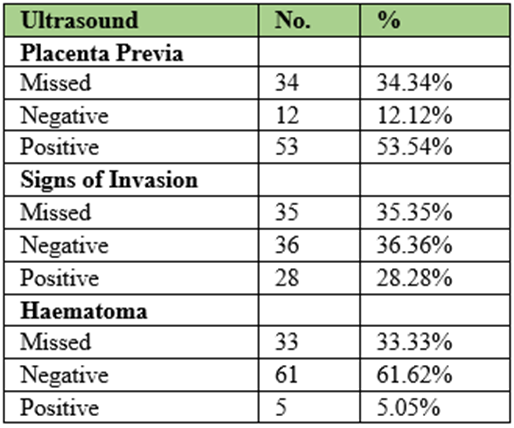
Table 3: Distribution of women according to their ultrasound (n=99).
Table 4 shows that the number of patients who received conservative management were 12 (12.12percentage), while those who had vaginal delivery were 29 (29.29percentage) and those who had Lower Segment Caesarean Section (LSCS) delivery were 61 (61.62percentage). The table also indicates that the number of patients who underwent CS with hysterectomy were 8 (8.08percentage). Other adjuvant management included were uterine artery ligation which was done for 12 patients (12.12percentage) and tubal ligation which was carried out for 7 patients (7.07percentage). The following procedures were also performed: cervico-isthmic sutures, internal iliac ligation, myomectomy, oophorectomy and repair of cervical tear which was recorded as 1 patient (1.01percentage) for each of these procedures respectively as demonstrated in the table.

Table 4: Distribution of women according to their management (n=99).
Table 5 shows the incidence of complications which clearly denotes that there were no ICU Admissions, maternal mortalities, bladder injuries, intestinal injuries and no incidence of postpartum haemorrhage.
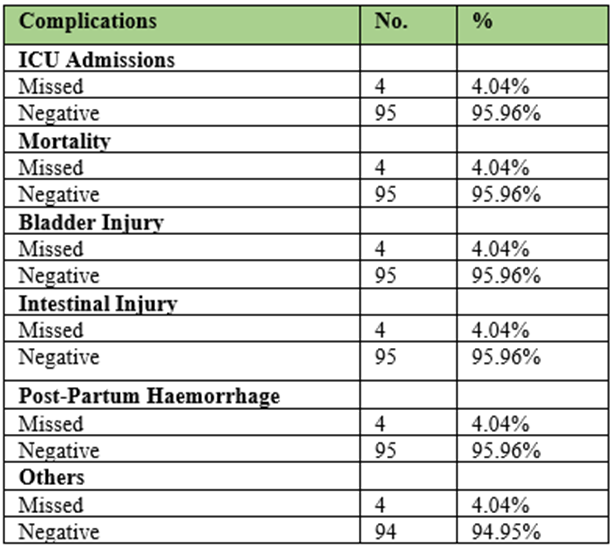
Table 6 shows that the mean haemoglobin (Hb) pre-operatively was 10.57±1.65(g/dl) while post-operatively was 9.64±1.27(g/dl). The mean difference calculated was 0.93(g/dl) and the t-test was 5.42. The p-value shows (less than 0.001) which indicates that the difference between preoperative and postoperative haemoglobin was statistically significant.
| Hb (g/dL) | Pre-operative | Post-operative | Mean Diff. | t-test | p-value |
| Range | 4.9-13.4 | 2-13.7 | 0.93 | 5.428 | <0> |
| Mean ± SD | 10.57±1.65 | 9.64±1.27 |
Table 7 shows the median blood transfusion required was 1 (0-3) and ranged between 0 and 10 while the median (IQR) of plasma needed was 0 (0-0) and ranged between 0 and 4.
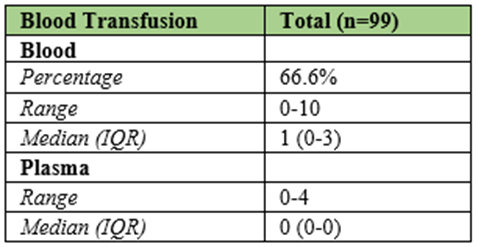
IQR: Interquartile range
Table 7: Distribution of women according to their blood transfusion (n=99).
Figure 1 shows that the number of women whose conditions were improved on discharge was 90 (90.91percentage), while those who were discharged against medical advice was 5 (5.05percentage). However those who required follow up were 3 (3.03percentage) and those who had escaped was 1 (1.01percentage).
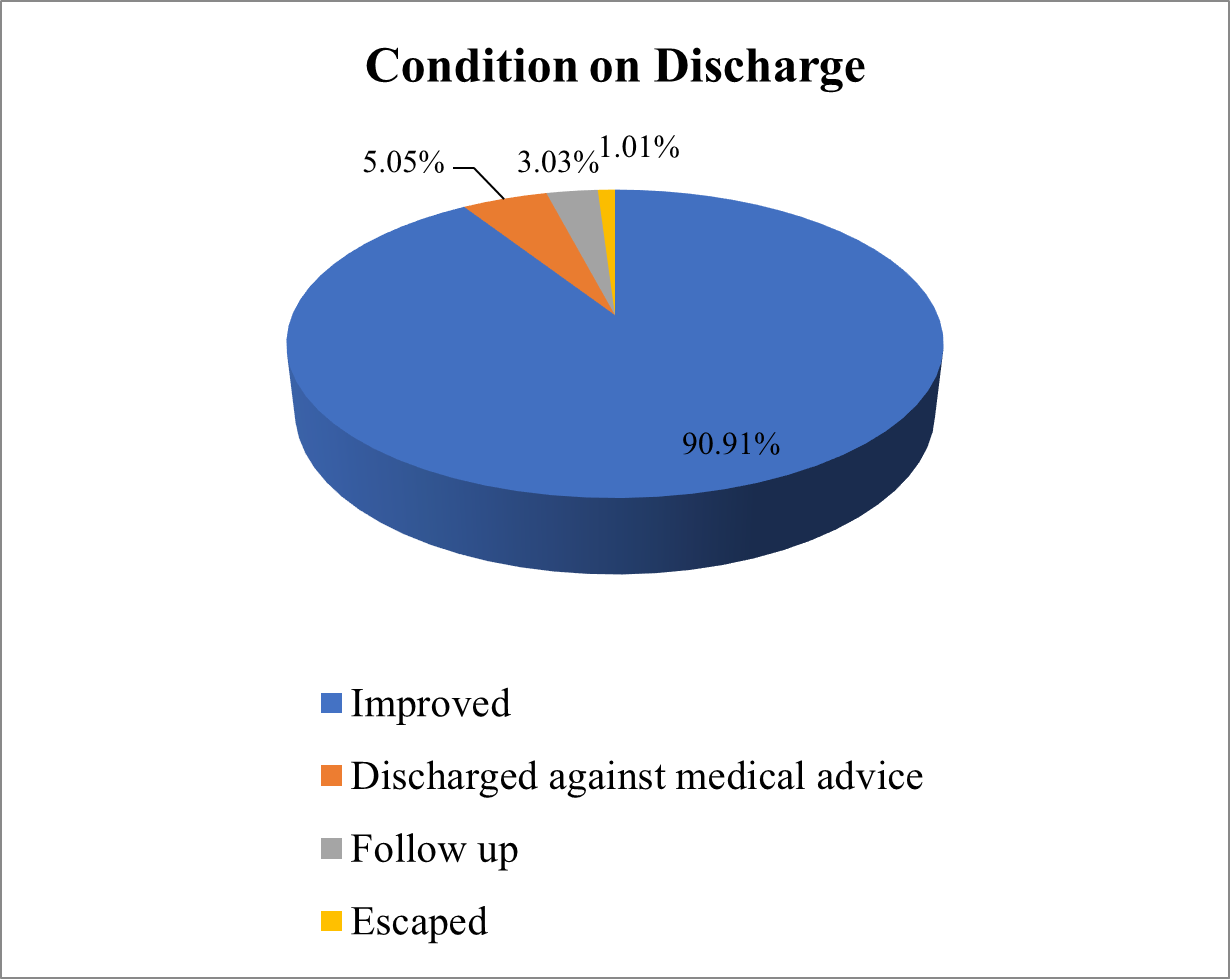
Figure 1: Pie chart of women according to their condition on discharge.
Table (8) shows the neonatal outcome which includes the mean weight of neonates which was 2.43±0.66 and the mean Apgar score was 8.31±1.25. It also illustrates that the number of new-born females were 36 (36.36percentage) and the new-born males were 54 (54.55percentage while the number of twins delivered were 5 (5.05percentage). The number of neonates who were kept under observation was 45 (45.45percentage) while those who required to be admitted to the NICU were 26 (26.26percentage), and those who were born with congenital malformations (CMF) was 1 (1.01percentage). Finally, the table also demonstrates that the number of babies who were discharged with their mothers were 84 (84.85percentage) and those who eventually died were 5 in number (5.05percentage).

Table 8: Distribution of women according to their neonatal outcome (n=99).
The incidence of APH reported from this study is 3.23percentage while it is quoted to be 2-5percentage, 2.01percentage and 2.53percentage in other studies from other parts of the world. The incidence of our study was similar to the incidence observed by Rajoriya et al., 2020 [1] which was found to be 3.27percentage while Jain et al., 2016 [4] study reported the incidence of 2.43percentage.
The range of the age of the patients with APH in this study is 17-41 with mean age presented 30.53±6.08 years which is similar to the results reported by Takai et al.,2017 [5] which stated that the mean age of the patients was 32.8 ± 5.5 years with a range of 20–44 years. This was also comparable to a study conducted by Gandhi et al., 2020 [2] which reported a mean age of 28 years.
Placenta previa was the main cause of APH which was 67.68percentage, followed by placenta accreta, accidental haemorrhage (abruptio placentae) and others which were 34.4percentage, 30.30percentage and 11.11percentage respectively. These results were comparable with a study conducted by Jharaik et al., 2019 [6] which recorded the following results: Placenta previa as 58.5percentage, abruptio placentae as 23.3percentage and undetermined cases as 18.05percentage. However, according to the results of the ultrasound examination, we have found that the incidence of the different types of APH were as the following: Placenta previa 53 (53.54percentage), signs of invasion 28 (28.28percentage) and haematoma 5 (5.05percentage) which was considered as more accurate results than the primary results of diagnosis of the cases. These results were comparable to a study conducted by Lankoande et al., 2017 [7] which observed that the incidence of placenta previa was 52 (42.6 percentage) and uterine rupture was 30 (24.6percentage) while the retro placental hematoma was 40 (32.8 percentage) which was different from our results but this could be due to the fact that their results were not all diagnosed using ultrasound examination as stated in their paper. Nevertheless, it is commonly known that especially retro placental hematoma could be easily misdiagnosed if ultrasound was not performed for confirming its diagnosis.
Rhesus blood grouping and haemoglobin measurement were performed in emergency as described in the literature. In our study the mean preoperative haemoglobin level is 10.57±1.65, while mean postoperative haemoglobin is 9.64±1.27. In comparison to a study conducted by Lankoande et al., 2017 [7] mean haemoglobin level before and after transfusion was 6.8g/dl. In our study, around 66.6percentage of APH patients required blood transfusion; in comparison to a study conducted by Lankoande et al., 2017 [7] around 84.4percentage patients of APH required blood transfusion. The difference in haemoglobin levels could be justified as there was usually so much blood lost during the delivery whether it was vaginal delivery or CS, and therefore many patients required blood transfusion as mentioned above in an attempt to compensate for the blood loss and to avoid further complications in the postpartum period.
In the present study, 61 (61.62percentage) of the patients underwent caesarean section, while 29 (29.29percentage) performed vaginal delivery. This was found similar to the study conducted by Jharaik et al., 2019[6] which recorded 63percentage of the patients underwent caesarean section while 46percentage performed vaginal delivery. This higher incidence of caesarean section was due to maternal indications which included increased rate of prior CS, major placenta previa, maternal medical conditions such as hypertension, diabetes, cardiac problems as well as maternal surgical history such as D&C which could also contribute to this phenomenon, while fetal indications include malpresentations and twins’ gestations. However, 8 (8.08percentage) patients required CS with hysterectomy which was comparable to results found by Tyagi et al., 2016 [8] which recorded 7 percentage of patients had performed caesarean hysterectomy.
In addition, the following procedures were also executed: Uterine artery ligation, tubal ligation, cervico-isthmic sutures, internal iliac ligation which were performed on 12 (12.12percentage), 7 (7.07percentage), 1(1.01percentage), 1(1.01percentage) of the patients respectively. These findings were almost similar to a study conducted by Malini et al., 2016 [9] which listed the following: Cervico-isthmic apposition stitch (4.7percentage), B-lynch stitch (2.8percentage) and uterine artery ligation (1.9percentage). These conservative surgical measures were administered to avoid further complications such as postpartum haemorrhage and peripartum hysterectomy. It was also documented that there was 0percentage maternal mortality in this study which was consistent with studies conducted by Jharaik et al., 2019 [6] and Samal et al., 2017 [10] which also noted zero maternal mortality. This might be due to the fact there were good antenatal, intranatal and postnatal care with good conduct of labour under strict aseptic conditions, correction of any medical disorders encountered prior to labour, careful control of bleeding with availability of blood banks and most importantly proper precautions were regularly taken and timely interventions were skilfully carried out by expert obstetricians and anaesthesiologists with all patients throughout the whole process. Therefore, this also explains our results regarding the fact that 90 (90.91percentage) of mothers’ conditions on discharge were successfully improved.
In the current study, 12 (12.12percentage) patients were booked and received conservative management for several days until delivery which included adequate hydration and nutrition, correction of any medical disorders, assessment of venous thrombo-embolism risk and its management, control of any risk factors, administration of corticosteroids and regular monitoring of maternal and neonatal conditions to avoid any complications later on. This result could be comparable with studies conducted by Tyagi et al., 2016 [8] and Yadav, 2019 [11] which registered 34percentage and 39 (35.12percentage) of patients were booked respectively. The lower booking status of the present study might be due to the fact that during this period most patients were practicing self-quarantine at their homes because of the coronavirus disease of 2019 (COVID-19) pandemic emergence, and so the antenatal care visit rates were considerably reduced. Thus, most patients came in as emergency cases with severe bleeding per vaginum and/or labour pains that required immediate management and delivery.
On the other hand, neonatal outcomes observed included the following: Mean birth weight of 2.43±0.66 kg which is similar to Chen et al., 2021 [12] study which is 2.50±0.49. While the number of multiple pregnancies registered were 5 (5.05percentage) twins in this study which is similar to Jharaik et al., 2019 [6] study which recorded 4 (3percentage) twins. Furthermore, 5 (5.05percentage) of neonatal deaths were recorded in our study. This rate was compatible with a study conducted by Das and Bhattacharyya, 2020 [13] where they recorded 4 (3.5percentage) early neonatal deaths. Our NICU admission rate was 26percentage (26.26percentage) which was compared to a study done by Tyagi et al., 2016 [8] which had 32percentage of their newborns admitted to NICU. These results could be correlated mainly to the prematurity of most cases as a consequence of early management of the patients and the numbers of preterm birth due to the increased numbers of emergency cases dealt with in this study. These findings highlight the significance of antenatal care and prior knowledge of complicating factors, as surgery scheduled electively with prior knowledge of complicating factors lead to a multidisciplinary approach and better preparedness, potentially lowering morbidity in these cases.
This study concludes that APH is still one of the principal causes of maternal morbidity and mortality in our country with increased rates of caesarean section, blood, and blood products transfusion, and NICU admissions. Causes of APH are placenta previa, placenta accreta, and placental abruption. The commonest mode of delivery was lower segment caesarean section. The NICU admissions and neonatal observation were high due to high rates of prematurity. Clinical care should therefore concentrate on prevention, early detection, proper antenatal care planning and prompt management with well-equipped facilities. Furthermore, pregnant women with APH should be considered high risk and timely management should be offered. In addition to the importance of the availability of senior obstetrician and anaesthetist during the delivery as well as a multidisciplinary preoperative preparation process ought to be pursued.
Limitations of the study
Since this study was retrospective in nature, there were some difficulties in accessing the records and collecting the required data due to lack of proper documentations and some patients' documents were missing.
Funding
No funding sources.
Conflict of interest
None declared.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
