
Case Report | DOI: https://doi.org/10.31579/2641-0419/315
Supraventricular tachycardias (SVTs) are common arrhythmias in clinical practice – they produce symptoms and lead to frequent emergency department visits1,2. The term “SVT” refers to tachyarrhythmias with a ventricular rate > 100bpm, where the mechanism for the arrythmia involves cardiac tissues above the bundle of His. The majority of SVTs conduct to the ventricles using the His-Purkinje system thereby producing a narrow QRS (< 120bpm). Presence of bundle branch blocks or other methods of aberrancy can result in SVT that presents as a wide QRS tachycardia.
*Corresponding Author: Pavel Antiperovitch
Citation: Pavel Antiperovitch, Allan Skanes, George Klein (2023), A Rational Approach to the Diagnosis of Narrow Complex Tachycardia. J. Clinical Cardiology and Cardiovascular Interventions, 6(5); DOI:10.31579/2641-0419/315
Copyright: © 2023, Pavel Antiperovitch. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 March 2023 | Accepted: 25 April 2023 | Published: 05 June 2023
Keywords: supraventricular tachycardias; arrhythmias; qrs tachycardia
Supraventricular tachycardias (SVTs) are common arrhythmias in clinical practice – they produce symptoms and lead to frequent emergency department visits1,2. The term “SVT” refers to tachyarrhythmias with a ventricular rate > 100bpm, where the mechanism for the arrythmia involves cardiac tissues above the bundle of His. The majority of SVTs conduct to the ventricles using the His-Purkinje system thereby producing a narrow QRS (< 120bpm). Presence of bundle branch blocks or other methods of aberrancy can result in SVT that presents as a wide QRS tachycardia.
Supraventricular tachycardias (SVTs) are common arrhythmias in clinical practice – they produce symptoms and lead to frequent emergency department visits [1,2]. The term “SVT” refers to tachyarrhythmias with a ventricular rate > 100bpm, where the mechanism for the arrythmia involves cardiac tissues above the bundle of His. The majority of SVTs conduct to the ventricles using the His-Purkinje system thereby producing a narrow QRS (< 120bpm>
When approaching a problem on a tracing, it is best to create a list of differential diagnoses. A list of common differential diagnoses is included in Figure 1. However, many diagnoses share mechanistic features, and are often grouped together into 4 main categories: atrial tachycardia (AT), AV Nodal Re-entrant Tachycardia (AVNRT), Atrioventricular Re-entrant Tachycardia (AVRT), and Junctional Tachycardia (JT).

Figure 1 - Differential diagnosis of a narrow complex tachycardia. NOTE: Ventricular tachycardia with early access to the His-Purkinje system is on the differential but is not included in this list.
In this review, we advise against pattern recognition and memorization of diagnostic algorithms, and instead encourage the reader to adapt a deeper understanding of the key mechanistic features for each arrhythmia. When approaching an unknown tracing, the reader should attempt to play out each mechanism to determine which arrhythmias can be excluded from the differential diagnosis list. We provide a number of tools to help clinicians with this exercise.
A Practical Approach to Svt Mechanisms
Mechanisms of arrhythmia generally fall into 4 types: automaticity, triggered activity, microreentry, and macroreentry. The first two are distinguished
biochemically, whereas microreentry refers to a small (generally < 2cm>focal arrhythmias because they originate from a “point source”. This is distinguished from macroreentry, which is an identifiable circuit that allows a propagating impulse to repeatedly reexcite tissue - a common example is atrial flutter, which is a macroreentry circuit in the atria that uses the caval-tricuspid isthmus to re-activate the atria [4].
Atrial tachycardia (AT) refers to mechanisms of arrhythmia that are entirely contained within the atria (Figure 2A).

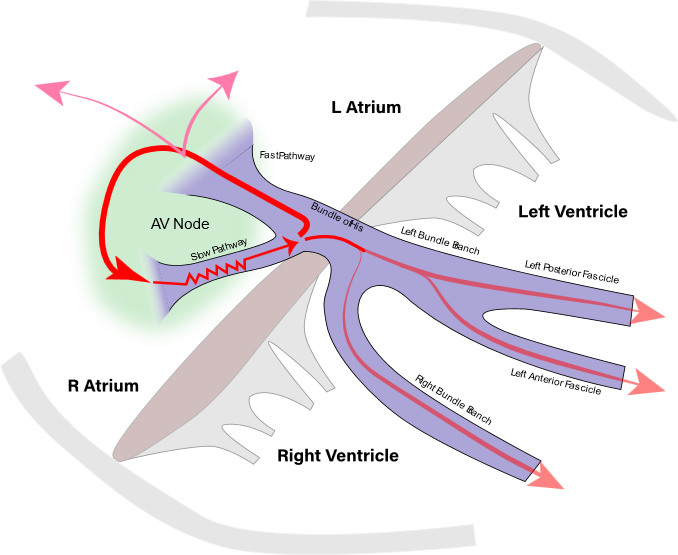
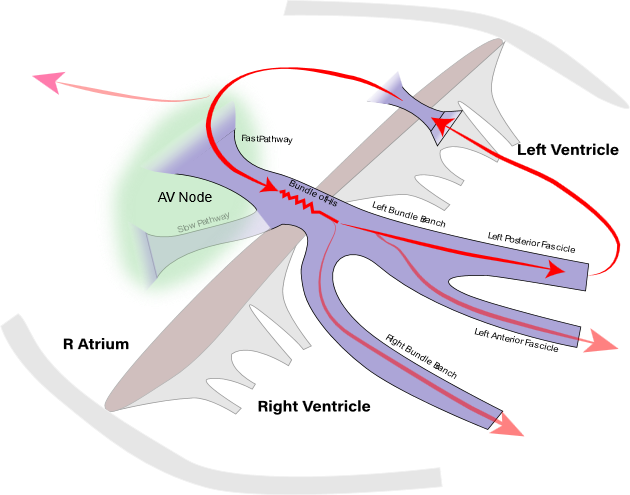
Figure 2 – A: Atrial Tachycardia mechanism is contained within the atrium. This diagram illustrates focal atrial tachycardia as an example. B: AV Nodal Reentrant Tachycardia (AVNRT) is a macroreentry circuit contained within the AV node. AVNRT does not require the atria or ventricles to sustain. This example demonstrates typical AVNRT with anterograde slow and retrograde fast pathways – note the simultaneous activation of atria and ventricles (in parallel) once the signal exits the slow pathway C: Atrioventricular Reentrant Tachycardia (AVRT) is a large macroreentry circuit, involving the accessory pathway, atrium, AV node, and ipsilateral bundle branch, and ventricular myocardium as part of its circuit.
The classic example is a focal atrial tachycardia, which originates from a point source within the atria. For simplicity, we consider atrial flutter to also fall into the category of AT because it is a macroreentry circuit that is entirely contained within the atria. Other common examples include sinus tachycardia and sinoatrial reentry tachycardia. All these mechanisms are non-AV node dependent, which means that a block in the AV node, either spontaneous or with administration of adenosine, is not expected to terminate the tachycardia since the mechanism does not require conduction through the AV node. AV Nodal Reentrant Tachycardia (AVNRT) is a macroreentry circuit where the obligatory component of the circuit is entirely confined to the compact AV node (Figure 2B). This circuit classically does not require the atrium or ventricles to sustain the tachycardia, and numerous examples
have been observed where AVNRT continues despite a conduction block to the atrium or ventricles5. Published case reports suggest that some AVNRT circuits do involve and require some atrial tissue [6]. AVNRT can be typical (tAVNRT), with an anterograde slow-pathway component, and a retrograde fast-pathway component – aka slow-fast AVNRT. Atypical AVNRT (aAVNRT) includes fast-slow and slow-slow configurations of the circuit, which are far less common. It is important to recognize that in tAVNRT the impulse travels antegrade via the slow pathway, and then simultaneously travels retrograde up the fast pathway to activate the atria as well as down the bundle of His to activate the ventricles. Conduction to both atria and ventricles occurs in simultaneously in parallel, which explains why the V-A time in tAVNRT is characteristically short. In fact, P-waves are often buried within the QRS, or can be seen in the tail end of the QRS (Figure 3C) – the so-called “pseudo-R prime” in V1. The simultaneous activation of atria are ventricles lead some clinicians to refer to it as an “A-on-V tachycardia”. In contrast, aAVNRT generally displays variable ventriculo-atrial (V-A) times and is often impossible to distinguish from AVRT and AT on surface ECG tracings on the basis of V-A relationship.
Atrioventricular Reentrant Tachycardia (AVRT) is a macroreentry arrhythmia with a large circuit that most commonly involves an accessory pathway (AP), atria, AV node, His bundle, ipsilateral bundle branch, and ventricular myocardium close to the AP (Figure 2C). This arrhythmia requires all the above structures, and conduction block in any of those structures would terminate or alter the arrhythmia circuit. Different variations of APs have been described, and we urge advanced learners to review them
Junctional Tachycardia (JT) is caused by an automatic circuit within the AV junction. Each beat of junctional tachycardia usually produces a retrograde P-wave and a QRS of supraventricular morphology. Just like in tAVNRT, conduction to the atria and ventricles occurs simultaneously in parallel, which manifests as a very short V-A interval. The relationship of P-wave and QRS depends on the location of the circuit and the relative conduction times to the atria and ventricles, but generally this will be an A-on-V tachycardia where the P-wave is within or just adjacent to the QRS.
The Search For P-Waves
The key to interpreting a narrow complex tachycardia lies with the identification of P-waves. Learners must train their eyes to recognize P-waves, which manifest as high frequency deflections that are outside the limits of the QRS. They can be easily distinguished from T-waves by their frequency: P-waves are sharper than T-waves because depolarization occurs faster than repolarization.
The presence of sinus beats allows readers to template the normal T-wave and compare it to the one in the tachycardia to detect any superimposed P-waves (see Figure 3A – Compare T-waves of the QRS1 and QRS2). Clinicians should avoid identifying P-waves within the limits of the QRS since parts of the QRS can mimic P-waves and are impossible to distinguish. Each time a candidate P-wave is identified, two candidate P-waves must be calipered to determine if an additional P-wave is hidden halfway. This reduces likelihood of missing 2:1 AV arrhythmias, commonly atrial flutter. Finally, it is important to note that many NCT tracings do not have visible P-waves, and the ability to narrow the differential diagnosis may be limited. Learners should search through tracings for other tools, such as the ones outlined in this review.
Diagnostic Tools
THE ONSET
The onset of an SVT can be somewhat helpful in determining the mechanism of the tachycardia. Most SVTs initiate with a premature atrial contraction followed by PR prolongation (Figure 3A), except for JT. PR prolongation itself is unhelpful because it can represent physiologic decrement in the AV node in response to a PAC, and is compatible with AT, AVNRT and AVRT. However, absence of decrement on the initiating PAC suggests that the slow conduction in the AV node is not required for the initiation of the tachycardia and helps exclude AV-node dependent macroreentry circuits - AVNRT and AVRT (Figure 3B).
Initiation with a PVC generally favours atypical AVNRT (aAVNRT) or AVRT. In AVRT, the PVC blocks in the AV node, conducts up the AP to the atrium, and re-enters the AV node anterogradely to complete the circuit. In aAVNRT, the PVC pe netrates the AV node retrogradely, finds the fast pathway refractory, which takes longer to recover than the slow pathway, allowing the stimulus to travel up the slow pathway retrogradely and re-enter the fast pathway to complete a cycle of atypical fast-slow AVNRT (Figure 3C). Finally, initiation with a ventricular event is very uncommon for AT, hence we can often rule out that possibility.
The onset also allows assessment of the ventricular-atrial (VA) time to determine presence of VA linking. In AT and JT, the first few P-waves in the tachycardia are not mechanistically linked to the timing of the previous QRS, unlike in AVNRT and AVRT. Therefore, presence of V-A linking, as in Figure 3A, suggests the diagnosis of AVNRT/AVRT and helps to exclude AT/JT, except if V-A appears linked by coincidence7. By contrast the tachycardia in Figure 3B does not demonstrate VA linking (measure from onset of QRS to P-wave) – some clinicians consider that this favours AT, but this can be compatible with any mechanism.
Figure 3A – Initiation of tachycardia with a long PR interval. Note the T-wave of QRS2 has a high-frequency component that is absent in QRS1, which suggests the presence of a P-wave (P3). The PAC labeled P3 initiates the tachycardia with a long PR interval. This finding does not help narrow the differential diagnosis. This tracing demonstrates VA linking (see text for details - Diagnostic Tools: The Onset). The VA is measured from the onset of QRS to onset of P-wave. This interval is fixed, suggesting that the first atrial activation (P3) is linked to the last QRS (QRS2), which helps rule out atrial tachycardia unless this happened by coincidence.
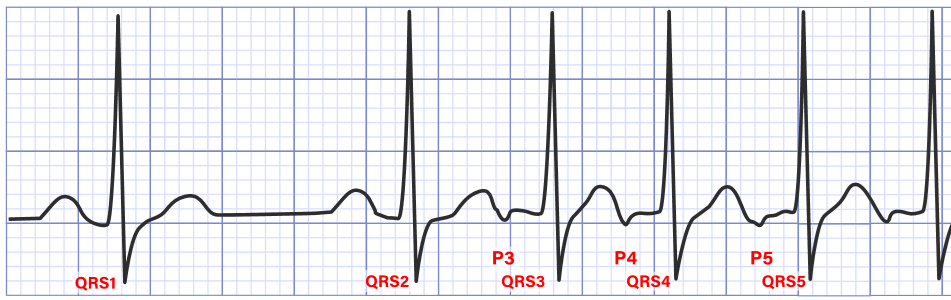
Figure 3B – PAC initiates the tachycardia without PR prolongation. This suggests that the delay in the AV node is not required for the tachycardia, and suggests against macroreentry involving the AV node, as in AVNRT and AVRT. Note VA linking is absent, favouring the diagnosis of AT. The VA time is measured from onset of QRS (i.e. QRS2) to onset of P-wave (i.e. P3) on tachycardia initiation, and compare it to the QRS3-P4 and QRS4-P5 intervals.
 Figure 3C – Initiation with PVC favours atypical AVNRT and AVRT. The ladder diagram illustrates the mechanism for initiation of fast-slow atypical AVNRT.
Figure 3C – Initiation with PVC favours atypical AVNRT and AVRT. The ladder diagram illustrates the mechanism for initiation of fast-slow atypical AVNRT.

Figure 4 – (A) Termination on a P-wave helps rule out AT, especially if observed multiple times. (B) Termination on a ventricular activation with a missing P-wave helps rule out JT.
Finally, the presence of a ramp-up and ramp-down phenomenon (aka non-paroxysmal) favours automaticity as the underlying mechanism of the tachycardia, which supports the diagnosis of AT or JT. Often, gradual changes in cycle length should prompt the clinician to consider sinus tachycardia as the mechanism, since the sinus node is heavily regulated by the autonomic nervous system.
Termination
The termination of the tachycardia can offer some important clues. Termination with an absent P-wave in the last cycle helps exclude AT. If an AT were to end on a P-wave (Figure 4A), then this P-wave must block in the AV node at the same time that the tachycardia mechanism terminates. This requires two isolated events to occur in two independent cardiac structures – atrium and AV node, which unlikely unless by pure chance. Similarly, JT would be unlikely if the last cycle is missing a P-wave (Figure 4B) because it would require a coincidental block from the JT focus to the atria on the same cycle that the JT stops. Seeing this type of termination more than once would help reduce likelihood of this being a coincidental finding.
Av Relationship
Once P-waves are identified, a clinician can use the AV relationship as an extra tool. A very short VA time suggests tAVNRT, and rules out AVRT.
Note that orthodromic AVRT requires activation of the ventricles before re-engaging the AP, which normally occurs apex-to-base. This means that the AP will not be engaged until most of the ventricles are activated, and the VA time in Figure 5A is too short to be AVRT. Although the exact cut-off was not defined in literature on surface tracings, a general cutoff value of 70ms is used [8]. Therefore, Figure 5A most likely represents tAVNRT, but AT with a long PR interval is possible, but far less common. Note that only very short AV times, the so-called A-on-V tachycardias, are helpful because they can exclude AVRT and bring tAVNRT/JT to the top of the differential. In adults, JT is uncommon, hence a very short VA tachycardia is often assumed to be tAVNRT. Any other AV relationship still carries the same differential diagnosis: aAVNRT, AVRT, AT, JT. For this reason, we find classifying NCTs as long-RP or short-RP does not help because both have the same differential diagnosis.
Variation in the tachycardia cycle length can also be helpful. If variation is detected, the clinician should caliper each QRS and candidate P-waves to determine which moves first (Figure 5B). In AT, the P-waves lead QRSs – AT can be ruled out if QRS leads the P wave. Conversely, if the P-wave moves first and leads the QRS, it is compatible with all SVT mechanisms, and nothing can be ruled out except for VT.

Figure 5 – AV Relationship – (A) Templating QRS1 to QRS3 - 6 reveals the presence of a pseudo-R’, which is a P-wave buried in the terminal portion of the QRS. This reveals a very short VA tachycardia, which excludes AVRT. This is a classic tAVNRT, which is common. Differential also includes AT over a slow pathway, but it is far less common. (B) ‘Wobble’ in the tachycardia cycle length reveals QRS complexes leading the P-waves, which rules out AT. Readers should caliper each QRS and P-wave and confirm that the QRS moves first. This is a similar concept to VA linking, which is demonstrated on this tracing.
It is important to note that a 12-lead ECG of the arrhythmia provides additional leads, which can help identify P-waves. The best leads to find the P-wave vary with each patient, but generally are the leads with the smallest QRS, anatomically proximal to the atria, and have the direction congruent with the vector of atrial activation. These are usually V1-V2, I, II, III, aVF.
The P-wave morphology in tachycardia on a 12-lead ECG can help identify the general direction of atrial activation. A retrograde P-wave activates the atrium in a low-to-high direction, registering as a negative deflection in the inferior leads. A high-to-low or left-to-right P-wave would not be compatible with arrhythmias that activate the atria from the AV node - JT and AVNRT.
We present a thoughtful approach to the diagnosis of narrow QRS tachycardia on a surface ECG. This method involves classifying the problem as a “narrow complex tachycardia”, creating a differential diagnosis list, and narrowing the differential by excluding items that are incompatible with the tracing. The tools illustrated in this figure include using the initiation, termination, AV relationship, variation in cycle length and P wave morphology. This approach allows the application of each SVT mechanism to diagnose arrhythmia and may be more intuitive to learners than memorization of diagnostic algorithms.
PAC – Premature Atrial Contraction; NCT – Narrow Complex Tachycardia; WCT – Wide Complex Tachycardia; AVNRT - AV Nodal Re-entrant Tachycardia; AVRT - Atrioventricular Re-entrant Tachycardia
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
