
Review Article | DOI: https://doi.org/10.31579/2692-9759/043
Department of Cardiac Anaesthesia and Cardiothoracic and Vascular Surgery, GB Pant Hospital [GIPMER], New Delhi, India.
*Corresponding Author: Vishnu Datt DA, Department of Cardiac Anaesthesia and Cardiothoracic and Vascular Surgery, GB Pant Hospital [GIPMER], New Delhi, India.
Citation: Vishnu Datt DA (2022) A Rare Quadricuspid Aortic Valve: Incidentally, detected on Intraoperative Tranesophageal Echocardiography J. Cardiology Research and Reports 4(6); DOI: 10.31579/2692-9759/043
Copyright: © 2022, Vishnu Datt DA, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 11 May 2022 | Accepted: 25 May 2022 | Published: 14 July 2022
Keywords: QAV; TEE; supravalvular PS; TR; RV dysfunction
The quadricuspid aortic valve (QAV) is an exceedingly rare congenital cardiac anomaly; often isolated, sometimes associated with other heart diseases. In many cases, the transthoracic approach is suitable for the diagnosis but, transesophageal echocardiography (TEE) is a tool for the accurate assessment of the valve anatomy. Clinical manifestations of patients with a QAV depend on the functional status of the QAV anFd the associated disorders. We present a one- year- old, 10 kg female child, who was diagnosed on TTE as Ostium secundum atrial septal defect (OS- ASD) with bidirectional shunt, supra- valvular pulmonary stenosis (PS) with a peak gradient of 120 mmHg, severe tricuspid regurgitation (TR) and Right ventricular (RV) dysfunction. However, in addition to the TTE findings, TEE examination performed while the baby was undergoing intracardiac repair, also incidentally detected the normally functioning QAV characterized by four cusps of equal size.
The quadricuspid aortic valve (QAV) is one of the rare congenital cardiac anomalies with an incidence of 0.00028-0.00033% in autopsy series, 0.0059-0.0065% for patients undergoing TTE assessment and 0.05-1% for those undergoing aortic valve replacements for aortic regurgitation (AR) [1]. It frequently appears as an isolated congenital anomaly, but may also be associated with other malformations like; coronary anomalies, coronary artery abnormalities, ventricular septal defect, patent ductus arteriosus, pulmonary stenosis, ruptured sinus of valsalva, complete heart block, hypertrophic cardiomyopathy and Ehlers–Danlos syndrome.[2] We also incidentally detected the normally functioning QAV characterized by four cusps of equal size in a one- year- old, female child, on perioperative TEE examination performed during cardiac correction surgery for OS -ASD, supravalvular PS , severe TR and RV dysfunction.
A 2 years old, 10kg, female child presented with bluish discolouration on crying since one and a half months of age. TTE revealed a large OS-ASD with bidirectional shunt, supravalvular and infundibular PS with peak gradient of 120mmHg, mild right RV dysfunction (TAPSE- 13 mm). The patient also underwent balloon dilatation for infundibular and supravalvular PS at the age of 5 months, and that led to some relief from the symptoms. However, she again started having bluish discolouration of lips and fingertips on cry. Therefore, she was referred to CTVS unit for intra-cardiac repair. Following confirmation of first and fifth day negative RTPCR reports and obtaining the Informed consent [ including cross infection from COVID -19] from the parents she was posted for intracardiac repair under cardiopulmonary bypass (CPB).
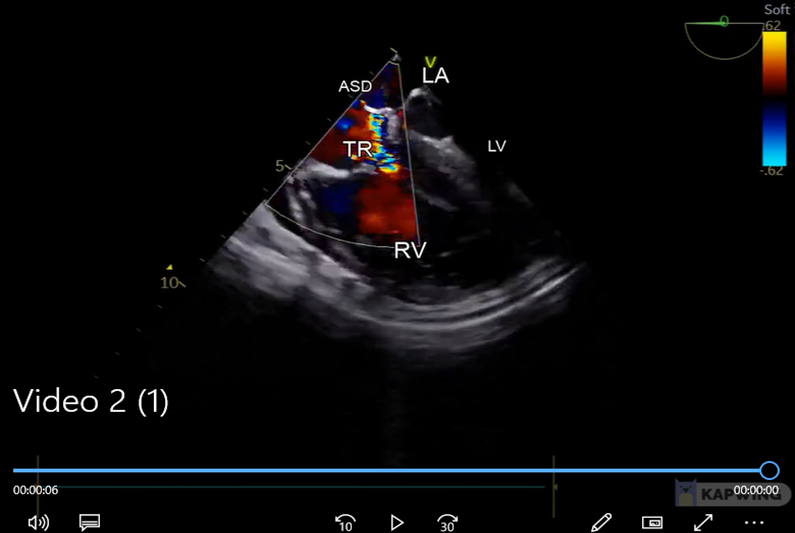
In OR, her base line SpO2 was 92%. The anaesthesia technique was used similar to any high-risk patients with complex congenital heart disease. In addition to standard ASA monitoring, TEE was also performed using paediatric probe (Size- 11x8mm, Model- GE VIVID S60 N) which also confirmed TTE findings, and severe TR with jet reaching to LA through large ASD suggestive of extremely high RA pressures (CVP =22 mmHg). RV was severely dilated, almost akinetic, and interventricular septum shifted towards LV. In contrast, LV was D-shaped, exceedingly small and hyper-contractile (lateral wall was touching septum during systole) with LV ejection fraction of 80%. (Video 1,2).

Video 1: 2-D image of Mid-esophageal aortic valve short axis view (0 degree) obtained through intraoperative TEE exam, demonstrating a normally functioning QAV with all equal size cusps. In addition, it also revealed a dilated and almost akinetic RV
TR- tricuspid regurgitation, OS- ASD – ostium secundum atrial septal defect, RV- right ventricle, LV- Left ventricle, LA – left atrium, IVS- interventricular septum
Video 2: Mid- esophageal 4Chamber View, color doppler demonstrate that the TR jet going into the LA via OS-ASD, suggestive of very high RA pressure. It also revealed a severely dilated and hypokinetic RV and IVS shifting towards LV suggestive of RV dysfunction. In contrast LV is exceedingly small but hypercontractile.
Incidentally, TEE also detected normally functioning QAV with all equal sized cusps that was missed during TTE. (Fig.1,2) (Video-3).
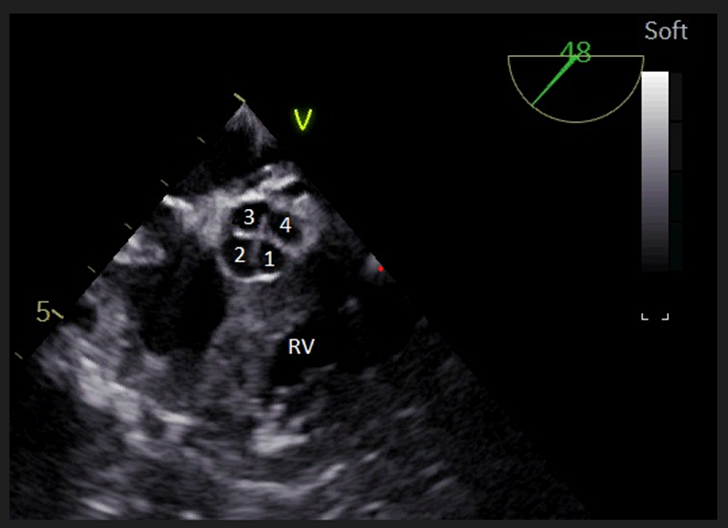
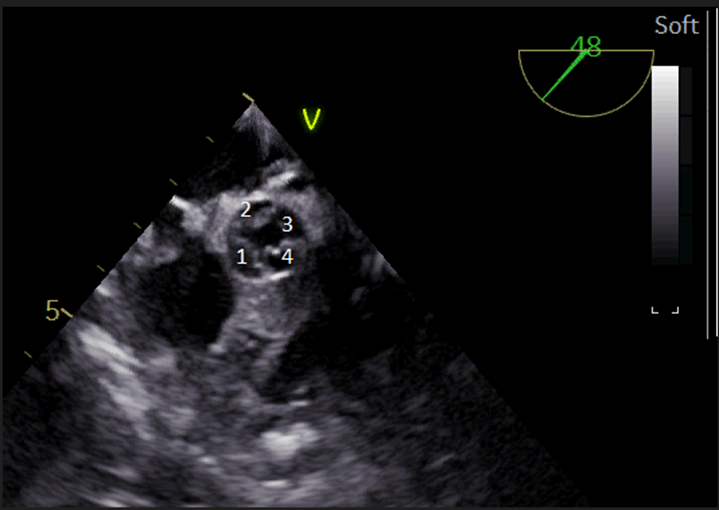
Figure 2: Mid-esophageal aortic valve short axis view obtained through intraoperative TEE exam, demonstrating in systole, a QAV valve and it opens like a “square”. [labelled]

RV- Right ventricle, LV – left ventricle, LA – left atrium, AA- ascending aorta
Video 3: Mid- esophageal LAX view (120 degree), 2-D image demonstrates a severely dilated and almost akinetic RV, and a very small sized LV with preserved LV functions suggestive of severe RV dysfunction
Heparin (300 units /kg) was used as an anticoagulant and after achieving an ACT value > 480 seconds, standard CPB technique with moderate hypothermia (27.5 degrees C) and antegrade blood cardioplegic (Del Nido) myocardial protection was used for intra - cardiac repair. The cardiac repair involved as pericardial patch closure of OS -ASD, RVOT muscle bundle resection, non- transannular pericardial patch augmentation of RVOT and MPA.
After rewarming, patient was successfully weaned off CPB using infusion of Adrenaline (.05ug/kg/min), Milrinone(0.5ug/kg/min), NTG(1mic/kg/min) and Noradrenaline (.0 5ug/kg/min). However, patient was low in haemodynamic; SBP- 68/27mmHg, CVP-10mmHg. in view of low haemodynamics and prolonged bypass time [CPB time 210 min, Aortic cross clamp time 83 minutes], Modified ultrafiltration [MUF]was performed and total 800 cc water was removed. Following that there was significant improvement in haemodynamics (BP -108/53mmHg, CVP-7mmHg, Hb- 16.6gm%). Heparin was neutralized with Protamine (1:1.3), and then aorta was decannulated. Following adequate haemostasis, the chest was closed, and the patient was shifted to ICU for elective ventilation. However, during ICU stay, the patient required regular peritoneal dialysis for 3-4 days. Gradually, patient was weaned off inotropes and tracheal extubation was done on fifth post-operative day. Rest of the course was uneventful, and patient was shifted into the ward on 10 th POD.
Incidence of QAV in the general population ranges from 0.013%-0.043%. [1] We conducted a literature review for the incidence of QAV with OS -ASD, infundibular and supra valvular PS, severe TR and RV failure and discovered that no similar case has been reported thus far. In 1973, Hurwitz and Roberts introduced the classification system in which seven subtypes, named A to G by the relative size of the four cusps, have been classified [2]. There are two classification systems for QAV: The Hurwitz & Roberts [3], in which the QAV is classified according to the size of the supranumerary cusp into seven categories from A to G, and to which Vali [4] has added the H type i.e. one large cusp, one mid -size and two equal small sized cusps. Nakamura et al. [5] have proposed another system of classification based on the position of the supranumerary cusp, whether it is located between the right and left coronary cusps (type 1), between the right and non-coronary cusps (type 2), between left and non-coronary cusps (type 3), and type 4 when there are four equal sized cusps present. QAV frequently appears as an isolated congenital anomaly, but may also be associated with other congenital cardiac malformations like; coronary anomalies, coronary artery abnormalities, ventricular septal defect, patent ductus arteriosus, pulmonary stenosis, ruptured sinus of valsalva, complete heart block, hypertrophic cardiomyopathy and Ehlers–Danlos syndrome. [2]
Though this patient had a normally functioning QAV, often such patients present with Significant aortic regurgitation while in their 50s and 60s and require subsequent intervention for AR.[6 ] QAV appears also to be at an increased risk of developing IE and therefore many authors have recommended antibiotic prophylaxis along with the annual follow to the patient. [ 7,8]
TTE and TEE are currently used as a diagnostic and follow-up method for this anomaly. Although in this patient the QAV was missed by the TTE, that was later detected during intraoperative TEE. TEE is the gold standard for the detection of QAV anomaly, as well as other possible cardiac lesions and it should therefore be indicated when morphological features of AVs cannot be evaluated by TTE. [9,10,11] In these cases, TEE is an accurate tool to define the diagnosis, demonstrate the four cusps, their size, ranking variant QAV, and visualize the possible displacement of coronary ostia.[12] Magnetic resonance imaging and computed tomography have an extremely high diagnostic value, but their use in clinical practice is not advised [12]
In addition, intraoperative TEE also provides valuable information on the hemodynamic measures of cardiac pressures, volumes and measures of the heart, and thus guides the anesthetic management, as well as the knowledge of estimated measures such as cardiac output, systolic/diastolic- volume/ function , regurgitant volume, ventricular ejection fraction and the evaluation of cardiac contractility, a better understanding of the present hemodynamic disorder can be obtained, and thus, to institute more effective and specific therapeutic interventions [13]
QAV is an exceedingly rare congenital cardiac anomaly. TEE showed more sensitivity and specificity in diagnosing the QAV compared with TTE. [14,15]
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
