
Case Report | DOI: https://doi.org/10.31579/2690-8794/087
*Corresponding Author: Unnati Desai, Associate Professor and Incharge, Department of pulmonary medicine, TNMC & BYL Ch Nair Hospital, Mumbai India.
Citation: Neenu N., Ketaki Utpat, Ammar Modi, Unnati Desai, Kishor Rajpal, D Shetty, Ramesh Bharmal (2021) A Rare Case of Pulmonary Arteriovenous Malformation - A Diagnostic Dilemma J, Clinical Medical Reviews and Reports. 3(7); DOI: 10.31579/2690-8794/087
Copyright: © 2021, Neenu N., This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 21 May 2021 | Accepted: 05 August 2021 | Published: 17 August 2021
Keywords: pulmonary arteriovenous malformation; refractory hypoxemia; vascular plugging
Pulmonary arteriovenous malformations (PAVM) are rare anomalies of pulmonary vascular system which may be incidentally detected or can have manifestations resulting from right to left shunt. PAVM can cause various systemic implications including central nervous system complications like stroke, brain abscess due to paradoxical emboli which mostly seen in previously undiagnosed PAVMs indicating importance of early diagnosis and timely intervention in PAVM. Computed Tomography Pulmonary Angiography (CTPA) is the diagnostic method of choice in PAVM. We present here a unique case of complex multiple PAVM presented with refractory hypoxemia in a middle aged patient diagnosed in our centre initially evaluated for malignancy based on chest radiography & High Resolution Computed tomography(HRCT)thorax findings and symptoms, later on after CTPA was diagnosed to have complex PAVM which showed clinicoradiological improvement following pulmonary vascular plugging. This case shows clinical scenario, diagnostic & management methods and differential diagnosis to be discussed in similar clinicoradiological pattern and peculiarity of PAVM despite advanced age.
Abbreviations: PAVM- Pulmonary arterio venous malformation, CTPA- Computed Tomography Pulmonary Angiography, CECT -contrast enhanced computed tomography, HHT- hereditary haemorrhagic telangiectasia
Pulmonary arteriovenous malformations (PAVMs) are rare abnormalities of the pulmonary vascular system [1] which are characterized by an abnormal communication between the pulmonary artery and vein, which result in a low resistant right-to-left shunt. The disease was first described at an autopsy in 1897 and first diagnosed during life in 1939 [2]. approximately 70% of PAVMs are associated with hereditary haemorrhagic telangiectasia (HHT), and about 15-30% of individuals with HHT have a PAVM. Multiple PAVMs are mostly associated with HHT. PAVM may develop later in life in hepatic cirrhosis and hepatopulmonary syndrome, schistosomiasis, mitral stenosis, trauma, actinomycosis, metastatic thyroid carcinoma, and chronic inflammatory condition such as bronchiectasis [3]. PAVM is of two types –simple and complex. Simple type is defined by the presence of single feeding artery and single draining vein. Complex type has two or more feeding arteries or draining veins. Around 80% of cases of PAVM are of simple type. Most important complications of PAVM result from intrapulmonary shunt which includes stroke, brain abscess, and hypoxemia. Local pulmonary complications of PAVM are PAVM rupture leading to life-threatening haemoptysis or hemothorax. The screening test for PAVM is transthoracic contrast echocardiography (TTCE) but Computed Tomography Pulmonary angiography (CTPA) has become the gold standard test to establish the presence of PAVM. The treatment of choice is endovascular occlusion of the feeding artery. Herein we discuss one such unique case of PAVM, its diagnosis, management and clinicoradiological improvement on follow up.
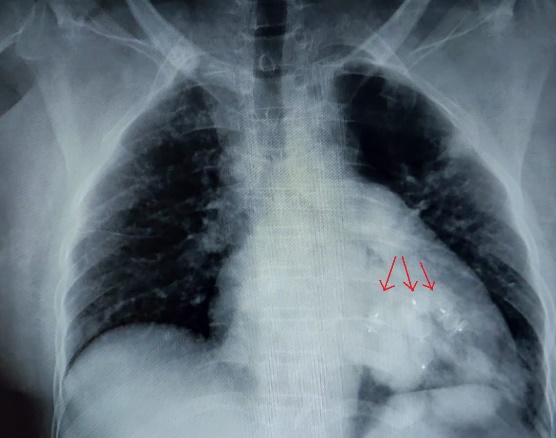
A 51-year-old lady presented with dyspnea on exertion corresponding to Modified Medical Research Council (MMRC) grade1and chest pain for 2 months duration. Past medical history revealed a cerebrovascular accident with left hemiparesis 9 years back, now resolved. Patient had previous history of 2-3 episodes of epistaxis. Patient had no significant past and family history. General examination showed grade 3 clubbing, Pulse rate of 97 /min, blood pressure of 130/80mmHg, respiratory rate of 20 per minute and pulse oximetry saturation of 52 % on room air. She had oxygen resistant hypoxemia; with oxygen saturation (SpO2) on bag and mask ventilation of 80 %( supine). She also had orthodeoxia with improvement in saturation in supine as compared to upright position. Respiratory and other systemic examination was within normal limits. Patient was evaluated with chest radiography showing retro cardiac nodular lesion (Figure 1).

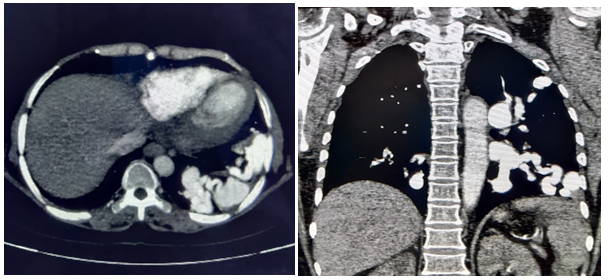
Arterial blood gas (ABG) analysis on room air revealed hypoxemia (Partial pressure of arterial oxygen (PaO 2) 46 mm Hg, oxygen saturation (SaO2) 52%). Computed tomography pulmonary angiography (CTPA) showed bilateral serpiginous dilated vascular channels suggestive of complex pulmonary arteriovenous malformation (figure 2).
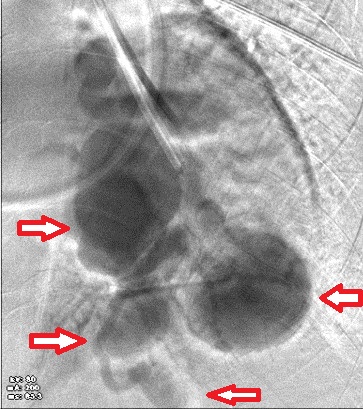
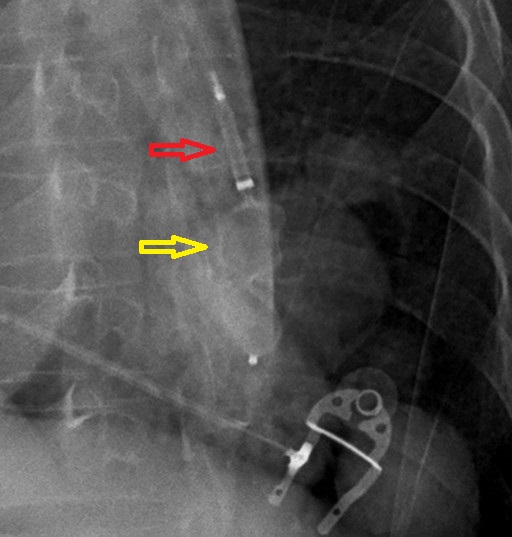
Doppler echocardiography was carried out to diagnose intracardiac right-to-left shunt which was normal and gave a strong suspicion for extra cardiac right to left shunt. The CT brain and ultrasonography abdomen was done which were normal. Patient underwent pulmonary vascular plugging done. Selective cannulation of left lower pulmonary artery performed showing a large AV fistula by three major supplying arteries forming multiple aneurysms. Selective cannulation of each supplying branch was performed & multiple Amplatzer plugs of 8mm, 10mm and 14mm was deployed in each of the supplying vessels. Post endovascular plug deployment, complete embolization of the AV fistula was seen with good diversion of flow seen in the rest of the lung (Figure 5a, 5b, 5c, 5d). Post procedure patient’s oxygen saturation improved to 90% on room air. No immediate post procedure complications were observed. Post procedure CXR (figure 3).



A repeat contrast enhanced computed tomography(CECT) scan was done one week later which showed complete thrombosis of arteriovenous fistula in the lateral basal segment and partial thrombosis of arteriovenous malformation in anteriobasal segment of left lower lobe( figure 4).On one month follow up patient symptomatically improved with oxygen saturation increased to 95% on room air. Since then, the patient has been asymptomatic without recurrence of the symptoms till now.
Pulmonary arteriovenous malformations (PAVM) are the pulmonary vascular abnormality caused by abnormal direct communications between pulmonary arteries and veins without an intervening capillary bed. Incidence of PAVM is around 2-3 per 1 lakh population. Most of the cases present during the first three decades of life. The first pulmonary AV malformation was described at autopsy in 1897. Since then, it has been given various names including cavernous angiomas of the lung, pulmonary arteriovenous fistulae, and pulmonary arteriovenous aneurysms. It can be congenital or acquired. Most of the congenital cases are related to hereditary hemorrhagic telangiectasia (HHT) whereas acquired causes include trauma, liver cirrhosis, tuberculosis, post-surgery, schistosomiasis and metastatic thyroid carcinoma. Most common location of PAVM is bilateral lower lobes, left more than right, and followed by right middle lobe and right upper lobe. Majority of cases are unilateral, only 8% to 20% of cases are bilateral. Increased blood flow and pressure in lower lobes and hydrodynamic forces causing subsequent stretch may be responsible for lower lobes to be commonly involved.
PAVM is of two types –simple and complex. Simple type is defined by the presence of single feeding artery and single draining vein. Complex type has two or more feeding arteries or draining veins. Around 80% of cases of PAVM are of simple type. Pulmonary arteries form the feeding arteries for most of the PAVMs; rarely systemic arteries like phrenic, intercostal and bronchial arteries can also provide feeders. Similarly, venous drainage is mainly through pulmonary veins.Only a few cases are diagnosed in neonates. Most of the cases will be asymptomatic till fourth decade of life. Patients can be completely asymptomatic or they can present with dyspnea (platypnoea/orthodeoxia), hemoptysis or chest pain, epistaxis, headache, TIA, CVA.Physical examination may reveal the presence of clubbing, cyanosis, hypoxemia, telangiectasia, and bruit /thrill. Main complications of PAVM occur from intrapulmonary shunt which includes stroke, brain abscess, and hypoxemia and pulmonary complications include PAVM rupture which can lead to life-threatening haemoptysis or hemothorax. Typical PAVMs appear on radiographs as rounded well-defined nodular lesions of varying size typically of 1–2 cm diameter with branching afferent feeding and dilated efferent draining vessel. However, mostly, the radiographic appearances are quite subtle with less obvious feeding and draining vessels [5]. The sensitivity of chest radiograph alone is 70% in diagnosing PAVM [6].
In our patient, the chest radiography and High resolution Computed Tomography of thorax showed bilateral nodular lesions suspicious for tumour which created a diagnostic dilemma. CT angiography is considered the ‘gold standard test’ for the diagnosis of PAVM with sensitivity over 97% [7]. Our case also confirms this observation. Pulmonary angiography is to be done before embolotherapy or surgical intervention, to document number and location of all lesions. Contrast echocardiography should be done to confirm the presence of right-to-left shunt and shunt fraction can be measured by the 100% oxygen method or by radionuclide perfusion lung scanning.
In our case, diagnosis of HHT had been made based on Curaçao’s diagnostic criteria. The 2011 Guidelines Working Group Consensus criteria recommend the use of the Curaçao criteria for diagnosing HHT. These clinical criteria provide probability score for HHT which is based on the presence of recurrent and spontaneous epistaxis, mucocutaneous telangiectasia at typical sites (lips, oral cavity, fingers, nose), spinal or gastrointestinal telangiectasia (with or without bleeding),visceral AVMs (pulmonary, cerebral, hepatic) and a family history, especially a first-degree relative with HHT (or genetic mutation). Presence of three or more of the above criteria confirms the diagnosis [8]. All symptomatic PAVMs and asymptomatic PAVMs larger than two cm, or if feeding arteries are larger than two mm, should be treated with surgery or embolotherapy because of the risk of paradoxical embolism [8, 9]. The treatment of choice in patients with multiple or bilateral PAVM is trans catheter embolotherapy with balloons or stainless-steel coils, and vascular plugs. In our case trans catheter embolotherapy with vascular plugs was performed. Post procedure patient improved clinically with arterial blood gas analysis showed increase in PaO2 to 60mmHg and SaO2 of 90%.
In this case, a repeat contrast enhanced computed tomography scan was done one week later which showed complete thrombosis of arteriovenous fistula in the lateral basal segment and partial thrombosis of arteriovenous malformation in anteriobasal segment of left lower lobe.On one month follow up patient symptomatically improved with oxygen saturation increased to 95% on room air.Our case is a challenging example of complex multiple PAVM which showed clinicoradiological improvement after pulmonary vascular plugging and it also prevented the patient from developing various complications which the patient is prone to including cerebral complications like stroke, brain abscess, Transient Ischemic Attacks(TIA),& other like haemoptysis& hemothorax. Hence it is highly recommended to undergo possible interventions like vascular plugging, in PAVM. Following treatment, collateralization and recanalization of PAVM can occur, and therefore long term clinical and imaging follow-up is required to assess PAVM enlargement and PAVM reperfusion.4Thenon-specific clinicoradiological presentations, which was much more suggestive of lung cancer in our case explain the diagnostic difficulties of PAVM.PAVM should be considered as differential diagnosis for cases with refractory hypoxemia where other aetiologies like pulmonary parenchymal diseases, congenital heart diseases, and pulmonary hypertension are ruled out and diagnosis and treatment of PAVM should be started as soon as possible as they increase with age and can increase the respiratory and neurological complications associated with PAVM [10].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
