
Case Report | DOI: https://doi.org/10.31579/2690-4861/817
1Consultant Radiologist and Assistant Professor, Department of Radio diagnosis, SGT Hospital and Medical College, Gurugram, Haryana, India
2Junior Resident, Department of Radio-diagnosis, SGT Hospital and Medical College, Gurugram, Haryana, India
*Corresponding Author: Bhavya Kataria, Consultant Radiologist and Assistant Professor, Department of Radio diagnosis, SGT Hospital and Medical College, Gurugram, Haryana, India.
Citation: Bhavya Kataria, Akshansh Singh, (2025), A Rare Case of Obstructed Hemivagina with Ipsilateral Renal Agenesis and Uterine Anomaly in an Adolescent: A Variant of Herlyn-Werner-Wunderlich Syndrome, International Journal of Clinical Case Reports and Reviews, 26(4); DOI:10.31579/2690-4861/817
Copyright: © 2025, Bhavya Kataria. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 June 2025 | Accepted: 09 June 2025 | Published: 13 June 2025
Keywords: ohvira syndrome; herlyn–werner–wunderlich syndrome; müllerian anomalies; renal agenesis; adolescent gynaecology
Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome, also known as Herlyn–Werner–Wunderlich syndrome, is a rare congenital Müllerian anomaly typically characterized by the triad of uterine didelphys, obstructed hemivagina, and ipsilateral renal agenesis. However, variants involving atypical uterine configurations and vaginal septa may occur, complicating diagnosis and management. We report the case of a 14-year-old adolescent girl who presented with recurrent lower abdominal pain a few months after menarche. Clinical evaluation revealed no palpable mass, but pelvic ultrasound showed the absence of the right kidney and two separate uterine cavities. MRI confirmed the presence of a bicorporeal uterus with two endometrial cavities and two cervical canals, a longitudinal non-obstructing vaginal septum, and a transverse obstructing vaginal septum. The obstruction resulted in hemato-trechalos and bilateral hematometra. The anomaly was classified as U3C2V1 under the ESHRE/ESGE classification. The patient underwent exploratory laparotomy with resection of the transverse vaginal septum and drainage of retained blood. Postoperative recovery was uneventful, and the patient was counselled regarding reproductive implications. This case represents a rare and complex variant of OHVIRA syndrome. Dual vaginal septa are uncommon, and their presence, along with bicorporeal uterus, underscores the diagnostic complexity. MRI proved invaluable in delineating anatomy and guiding management. Literature supports early diagnosis and timely surgical correction to prevent complications like endometriosis and infertility. This case highlights the importance of considering Müllerian anomalies in adolescents with post-menarche cyclical pain. MRI facilitates accurate diagnosis, and early surgical intervention can optimize clinical and reproductive outcomes.
Müllerian duct anomalies (MDAs) are congenital malformations that result from defective development, fusion, or resorption of the paramesonephric (Müllerian) ducts during embryogenesis. Among these, Obstructed Hemivagina and Ipsilateral Renal Agenesis (OHVIRA) syndrome—previously described as Herlyn–Werner–Wunderlich syndrome—is a rare but clinically important variant. It is defined by the classical triad of uterine didelphys, unilateral obstructed hemivagina, and ipsilateral renal agenesis [1–3].The estimated incidence of OHVIRA syndrome ranges from 0.1% to 3.8%, although the true prevalence is likely underreported due to frequent misdiagnosis and lack of awareness [4,5]. This anomaly results from disrupted development of the Müllerian and Wolffian ducts, particularly during the 10th to 12th weeks of gestation, leading to uterine duplication and vaginal septum formation depending on the level of fusion failure [2,4,6].OHVIRA syndrome is typically diagnosed during adolescence, usually after menarche, when the obstruction of menstrual outflow leads to symptoms such as cyclical lower abdominal pain, pelvic mass, or hematometra. Complications may include hematocolpos, endometriosis, infection, and future infertility if not diagnosed and treated promptly [1,3,5]. While uterine didelphys with complete obstructed hemivagina is the most common variant, other atypical forms involving bicorporeal uterus, longitudinal or transverse vaginal septa, and varying degrees of obstruction have also been documented, adding to the diagnostic complexity [3,6].Imaging modalities like ultrasound and magnetic resonance imaging (MRI) are essential for accurate anatomical delineation and surgical planning. In light of the embryological relationship between the genital and urinary systems, several authors recommend screening for Müllerian anomalies in girls with prenatally detected renal agenesis—even in the absence of gynecological symptoms [4]. We report a rare and complex case of a 14-year-old adolescent female who presented with recurrent lower abdominal pain shortly after menarche and was ultimately diagnosed with a variant of OHVIRA syndrome involving bicorporeal uterus, double cervix, a longitudinal non-obstructing vaginal septum, and an obstructing transverse vaginal septum causing hemato-trechalos and bilateral hematometra, along with right renal agenesis. This case underscores the importance of early recognition of Müllerian anomalies and timely surgical intervention to prevent long-term complications.
A 14-year-old female, presented to the outpatient department with complaints of recurrent lower abdominal pain, described as waxing and waning in nature. She had attained menarche in November 2024 and reported a history of regular menstrual cycles since then. However, the persistence of abdominal pain raised concerns.
On clinical evaluation, mild abdominal tenderness was noted without any palpable mass. An initial pelvic ultrasound was performed, which revealed absence of the right kidney and the presence of two separate uterine cavities, suggestive of a congenital uterine anomaly. For further evaluation, magnetic resonance imaging (MRI) of the abdomen and pelvis was advised.
MRI pelvis revealed the presence of a bicorporeal uterus with a wide fundal cleft and two separate endometrial cavities diverging at an obtuse angle. There were two distinct cervical canals continuing into two separate vaginal canals. (Figure 1) A thin transverse hypointense band was identified at the junction of the right distal endocervical canal and proximal vaginal canal, likely representing a transverse vaginal septum. This resulted in upstream accumulation of blood (hemato-trechalos) within the right cervical canal, which appeared dilated, measuring approximately 7.9 × 4.7 × 4.4 cm, and showed signal intensities consistent with blood products of varying ages. (figure 2) This dilated cervical segment caused significant mass effect with posterior displacement of the left endocervical canal and anterosuperior displacement of the uterine horns and urinary bladder.

Figure 1: SAGGITAL T2WI showing hemato-trechalos with a transverse thin vaginal septum (red asterisk and arrow).
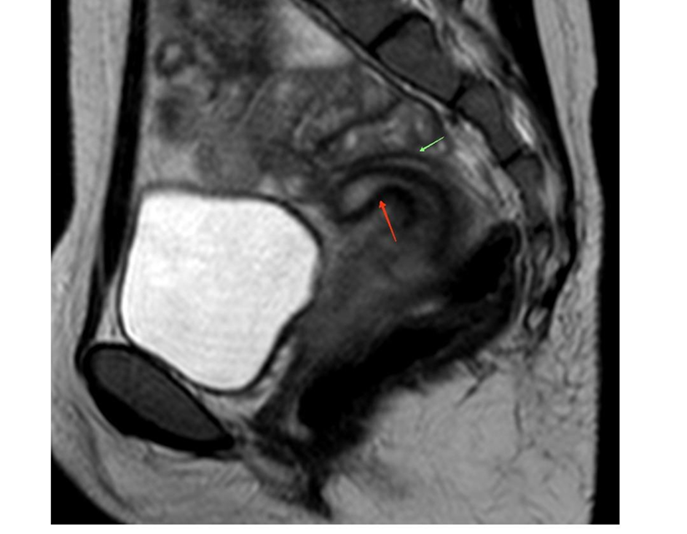
Figure 2: T2W sagittal image showing hemato-trechalos (red arrow) and displaced cervical canal (green arrow).
Bilateral endometrial canals were distended, measuring 13.67 mm in the right horn and 11.1 mm in the left horn, consistent with bilateral hematometra, more marked on the right side. Two vaginal openings were visualized at the perineum, separated by a longitudinal non-obstructing septum. Both vaginal canals were otherwise patent, with no significant blood collection noted. The bilateral ovaries were normal in size and signal intensity, with preserved follicular architecture. No free fluid or lymphadenopathy was noted. Screening sections of the upper abdomen revealed right renal agenesis, with a compensatorily enlarged but structurally normal left kidney. (Figure 3) The above findings were consistent with a complex Müllerian anomaly, classified as U3C2V1 under the ESHRE/ESGE classification system. Although not a classical presentation, the overall features were suggestive of a variant of Herlyn-Werner-Wunderlich syndrome (OHVIRA). The patient underwent exploratory laparotomy, during which the obstructing transverse vaginal septum was resected and the collected blood was evacuated. The postoperative course was uneventful. She was discharged in stable condition and counselled regarding the nature of the congenital anomaly, its reproductive implications, and the need for long-term follow-up.

Figure 3: Coronal T2WI showing single enlarged left kidney (green arrow) and two diverging uterine cavities (red arrow
Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome, also known as Herlyn–Werner–Wunderlich syndrome, is a rare congenital anomaly resulting from defective development and fusion of the Müllerian and Wolffian ducts. It is classically defined by the triad of uterine didelphys, obstructed hemivagina, and ipsilateral renal agenesis. However, anatomical variations such as bicorporeal uterus or the presence of both longitudinal and transverse vaginal septa, as observed in our case, are increasingly being recognized and reported.
Our patient, a 14-year-old adolescent girl, presented with cyclical lower abdominal pain a few months following menarche, consistent with the typical presentation window of OHVIRA syndrome. Literature reports that symptomatic presentation often occurs between 12 and 16 years of age when menstrual blood accumulates behind an obstructed vaginal canal, resulting in hematometra or hematocolpos [7-11]. Similar to our case, many patients initially present with nonspecific complaints such as dysmenorrhea or abdominal pain, making early diagnosis challenging and frequently delayed.
MRI in our patient revealed a bicorporeal uterus with two separate endometrial cavities and cervices, a non-obstructing longitudinal vaginal septum, and an obstructing transverse vaginal septum leading to hemato-trechalos and bilateral hematometra. This constellation of findings is classified as U3C2V1 under the ESHRE/ESGE classification and represents a rare and complex variant of OHVIRA syndrome. Similar anatomical variants have been reported in literature, such as the case described by Gungor Ugurlucan et al., where MRI helped in identifying the extent and nature of obstruction, guiding surgical planning [3].
While the classical form of OHVIRA involves a unilateral obstructing longitudinal vaginal septum, our case is unique in demonstrating dual septation—longitudinal (non-obstructing) and transverse (obstructing). This rare variation has been highlighted in the systematic review by Kudela et al., which analyzed 734 cases and documented multiple anatomical variants, including transverse septa causing obstruction [4].
The management of OHVIRA depends on the type and location of obstruction. In our patient, laparotomy was performed to excise the obstructing transverse vaginal septum, and the accumulated blood was drained. This approach aligns with the fertility-sparing principles advocated in the literature, where surgical correction of obstruction is the mainstay to prevent complications such as endometriosis, infection, pyocolpos, and future infertility [12-14]. Early intervention is critical, as delay in management has been associated with severe complications including hematosalpinx, pelvic inflammatory disease, and tubal damage [9,12,15].
Kimble and Kimble's study underscores the diagnostic utility of prenatal sonography for early detection in asymptomatic prepubertal patients with renal anomalies [16]. However, in postpubertal patients, especially those who are menstruating, presentation is commonly due to symptomatic obstructive outflow and may require detailed MRI evaluation, as in our case [2].
The use of imaging, especially MRI, has been well supported by Han et al. and other authors as the gold standard for defining Müllerian anomalies and planning individualized surgical treatment [6]. Moreover, imaging-guided and minimally invasive surgical techniques such as vaginoscopic septal resection, hysteroscopy, or laparoscopy have shown excellent outcomes while preserving hymenal integrity in adolescent girls who have not been sexually active [17-19].
In terms of long-term reproductive outcomes, early surgical correction improves fertility prospects significantly. Studies by Candiani et al. and Zhu et al. report high pregnancy rates and favourable obstetric outcomes in women who underwent timely septal resection [20,21]. Similarly, Heinonen et al. concluded that women with uterus didelphys generally have good reproductive potential provided early diagnosis and management are achieved [22].
This case highlights a rare and complex variant of OHVIRA syndrome presenting with dual vaginal septa and bicorporeal uterus. It reinforces the importance of early imaging, especially MRI, in adolescents presenting with cyclical pelvic pain post-menarche. Surgical correction through excision of the obstructing septum remains the mainstay of treatment. Early diagnosis and appropriate intervention are vital in preventing complications and preserving reproductive health. This is consistent with findings by Moufawad et al., who provided a comprehensive overview of diagnostic approaches and surgical strategies in OHVIRA syndrome [23].
Limitations: Being a single case report, generalisability is limited. Long-term follow-up to assess reproductive outcomes was not available. Furthermore, genetic studies were not performed to evaluate any syndromic associations due to resource constraints.
Recommendations: Early imaging, particularly with MRI, should be considered in adolescent girls presenting with cyclical abdominal pain post-menarche. Clinicians must maintain a high index of suspicion for Müllerian anomalies in the presence of renal agenesis. Multidisciplinary care involving radiologists, gynaecologists, and paediatric surgeons is crucial to ensure timely diagnosis and fertility-preserving intervention
This case illustrates a rare variant of OHVIRA syndrome with dual vaginal septa and a bicorporeal uterus, presenting with post-menarche cyclical pain. MRI leads to accurate diagnosis, and timely surgical resection of the obstructing septum led to symptom relief and preservation of reproductive potential. Early recognition and intervention are essential to prevent complications and ensure favourable outcomes.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
