
case report | DOI: https://doi.org/10.31579/2692-9392/119
1 Fourth-year medical students, California Northstate University College of Medicine (CNUCOM), Elk Grove, California, USA
2 Assistant Clinical Professor, CNUCOM, Elk Grove, California and Emergency Physician, St. Agnes Medical Center, Fresno, California, USA
3 Radiologist, St. Agnes Medial Center, Fresno, California, USA
4 Medical scribes, St. Agnes Medical Center, Fresno, California, USA
5 Professor and Director of Emergency Medicine Clerkship, California Northstate University College of Medicine (CNUCOM), Elk Grove, California, USA
*Corresponding Author: Ranasinghe L, Professor and Director of Emergency Medicine Clerkship, California Northstate University College of Medicine (CNUCOM), Elk Grove, California, USA.
Citation: Dang R, Eggleton J , Habibe M, Alhadi S, Kessler M. et all (2022) A Rare Case of Mastoiditis in an Adult Patient. J. Archives of Medical Case Reports and Case Study, 5(5); DOI:10.31579/2692-9392/119
Copyright: © 2022 Ranasinghe L, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 March 2022 | Accepted: 15 April 2022 | Published: 22 April 2022
Keywords: mastoiditis; pediatric
Mastoiditis is more commonly seen and easily recognized in children. However, adults are more likely to present with complications requiring emergency medical treatment. One of the challenges in the management of mastoiditis is recognizing symptoms and beginning treatment with antibiotics early to prevent progression of disease and potential surgical management. This case report details an unusual case of a 41-year-old woman whose indolent symptoms went unrecognized for three weeks before presenting to the emergency department with unilateral ear pain and hearing loss. Imaging revealed coalescing mastoiditis with erosion of the medial cortex into the jugular foramen and enhancement suggestive of meningitis. This report can assist practitioners in recognizing and managing mastoiditis and its associated complications in the emergency setting.
Background
Mastoiditis is an infection or inflammation of the mastoid air cells that most often results from the contiguous spread and progression of an acute or chronic otitis media (OM) infection [1]. Before diagnosis of mastoiditis, patients tend to have more than one visit to physicians with reports of unilateral otalgia, swelling, erythema over the mastoid bone, fever, and hearing loss. There is a risk of progression into intratemporal and intracranial complications that may be deadly such as prolonged latent mastoiditis, intracranial abscesses, meningitis, sigmoid sinus thrombosis, or otogenic hydrocephalus if not treated promptly [2,3]. Otitis media is a common childhood disorder with a peak incidence between 6 months and 2 years of age [4,5]; however the average age of patients presenting to the emergency room with complications of OM is 37 years of age. [6] While the incidence of mastoiditis overall has declined significantly with the routine use of antibiotics for OM, some studies have shown that the incidence of mastoiditis in adults has remained consistent [2,7]. This report is significant, as most of the literature on this topic is based on pediatric cases. This case report details an unusual case of a 41 year old woman on initial presentation to the emergency room with minimal symptoms which ultimately proved to be advanced mastoiditis complicated by osteomyelitis of the mastoid bone.
The patient was a forty-one year old female with a past medical history significant for asthma, gastriculcers, endometriosis, and more than ten packyears of smoking history, presenting to the emergency department complaining of left ear pain for three weeks. The pain was rated a constant 10/10 on the pain scale and described as “dull with aching” in quality. This pain was reported to be minimal to start, but progressed gradually over three weeks with similar discomfort radiating up the left jaw. The pain was initially responsive with use of over-the-counter pain medications, but she eventually presented to the emergency department when they no longer relieved or controlled the pain. Associated with the ear pain was hearing loss of the left ear that progressively increased in severity over three weeks. Other associated symptoms included yellow drainage from the left ear, which self-resolved one week prior to her initial presentation to the emergency department, left-sided neck swelling, and mild nasal congestion. The patient denied right ear pain, changes in right-sided hearing, fever, nausea, vomiting, headache, or dizziness. She did not seek medical attention prior to her visit to the emergency department. She had no further reported chronic medical conditions and she took no medications regularly at home. The rest of the review of systems was unremarkable.
The patient’s vital signs upon arrival to the department indicated that she was afebrile at 36.6° Celsius, normal tensive with a BP 132/88 mmHg, heart rate of 99 bpm, respiration rate of 16 breaths per minute, and saturating at an SPO2 of 100% on room air.
Upon physical exam, the patient was a well-appearing female in mild distress due to her left ear pain. There was tenderness, slight swelling, and erythema located behind the patient’s left ear. The tragus and auricleof the left ear were extremely tender.There was also significant tenderness at the left mastoid.
Using the otoscope, the ear canal was noted to have mild swelling with a normal-appearing ear drum, with minimalerythema of the external auditorymeatus. There were no abnormalities seen on the physical exam of the right ear or the throat. There was no significant neck swelling. Patient had a regular rate and rhythm with cardiac auscultation. Lungs were clear to auscultation without labored breathing. Patient had normalspeech with baseline movement of all four extremities.
During ENT consultation, the left tympanic membrane was dull with signs of middle ear effusion visualized. The left pinna was displaced forward with marked tenderness along the mastoid bone. There was moderateedema of the extra-auditory canal.Sound lateralized to the left ear with Weber testing.
As part of the emergency medicine workup, the following labs were ordered: CBC, CMP, lactate, b-HCG. The CBC revealed leukocytosis with 19,000 cells/mcL and a high neutrophil percentage of 78.1%. The remaining lab values were non pertinent to management or diagnosis. While in the ED, the patient received the following as part of management: Unasyn 3g x1, Vancomycin 1250mg x1, Norco 5mg/325mg x1, Morphine 6mg x 1, Zofran 4mg x 1, Ibuprofen 600mg x1. The case was discussed with the inpatient medicine team and the ENT surgical team. Patient was admitted to the inpatient team for intravenous antibiotics and surgical intervention. Admitting diagnoses included abscess, encephalitis, meningitis, and leftmastoiditis.
Blood cultures and ear cultures were collected. Patient’s wound indicated 1+ growth of streptococcus pneumoniae. No strict anaerobes were isolated.
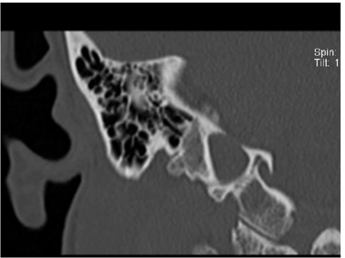
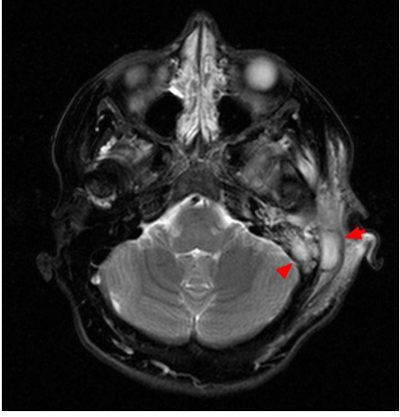
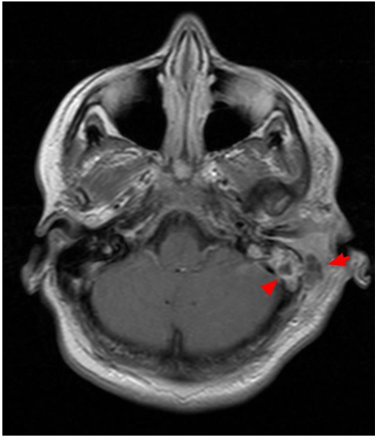
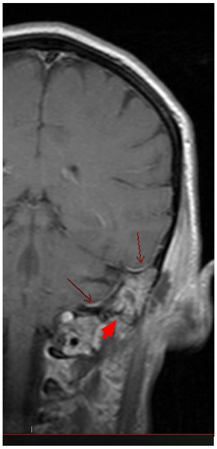
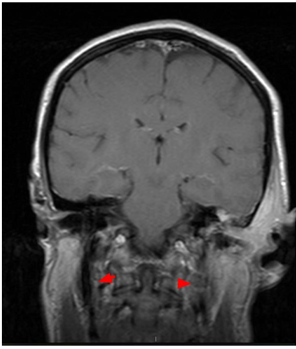
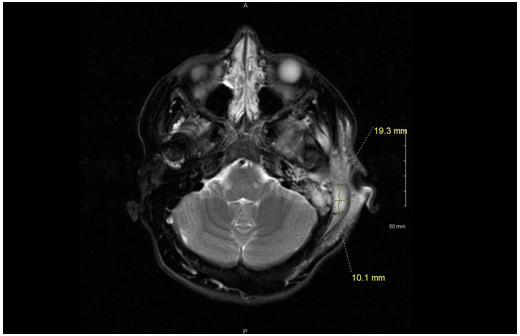
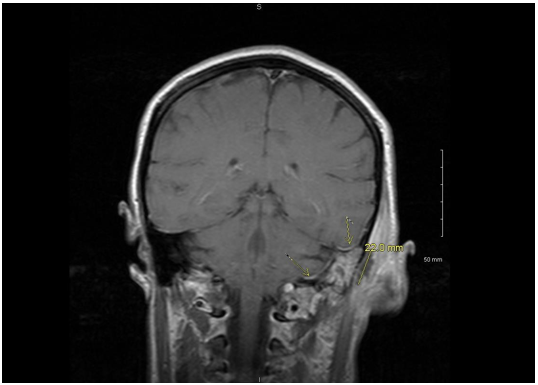
A noncontrast CT scan of the temporal bones and an MRI of the brain with and withoutcontrast were also orderedin the ED. The CT scan showed extensive periauricular soft tissue swelling and absorption of several septae of the mastoid air cells with erosive changes of the medial wall indicative of coalescent mastoiditis and concern for intracranial extension. Additionally, fluid could also be seen within the middle ear cavity; however, the ossicles remained intact. The contralateral ear and mastoid air cells were normal. On the MRI, a 1.9 x 1.0 x 2.2 cm fluid collection was seen in the periauricular tissues demonstrating restricted diffusion and peripheral enhancement, compatible with an abscess. Fluid signal and enhancement of the mastoid air cells, as well as septae absorption and medial cortical wall erosion, again confirmed the diagnosis of coalescent mastoiditis.
Intracranial extension of the infection was confirmed with thickening and enhancement of the meninges and possible diffusion restriction along the outer cortex of the adjacent cerebellar hemisphere. No definitive flow void was seen in the distal sigmoid sinus and jugular vein raising concern for venous compression with possible thrombus. Images with captions/descriptions included at the end of this publication.
During her first twelve hours of admission on antibiotics, the patient reported feeling considerably better. Dexamethasone sodium phosphate 4mg/mL 1mL q8h x 3, Piperacillin/Tazobactam 4.5g q6h IV, and Ondansetron 2mg/mL 2mL q6h prn nausea/vomiting were added to the patient’s medications. In preparation for surgical intervention with ENT in the morning, she was kept NPO. There were no further documented changes in condition throughout the night.
After evaluation of the patient and imaging, ENT deemed that the patient needed to undergo a tympanomastoidectomy. The CT and MRI imaging were indicative of coalescent mastoiditis with abscess formation overlying the mastoid bone, extending to the jugular bulb. Erosion of the tegmen overlying middle fossa, as well as evidence of meningitis with significant inflammation of the meningeal of the middle fossa, was reported. Additionally, there was soft tissue opacification of the middle ear cavity, as well as multiple entire left mastoid air cells. Patient was presented with all treatment options, with all the risks, benefits, and possible outcomes discussed. She understood and agreed to follow through with the operative route.
The operative procedures performed include: left tympanomastoidectomy with facial nerve monitoring using NIM nerve monitor and left myringotomy with tube placement. The operation was successfully performed with no complications and minimal blood loss (>20mL). During the procedure, evidence of a large abscess pocket overlying the mastoid bone extending over the temporalis fascia were noted. There was also evidence of cortical erosion of the mastoid, approximately 3 cm above the tip of the mastoid, and tegmen erosion that overlined the middle fossa of the sigmoid portion of the jugular bulb with total exposure. Additionally, some tissue granulation and mucopurulent fluid were noted throughout the mastoid air cell, as well as thickened granulated and polyploid tissue within the middle ear cavity with mucopurulent fluid, dehiscence and exposure of the meninges of the middle fossa. The surgical site was appropriately closed and a Penrose drain was placed for drainage purposes. The middle ear cavity was infused with ofloxacin through the myringotomy tube and an Otowick was then placed overlying the Gelfoam and was expanded with ofloxacin drops. The patient was then awakened, extubated safely, and transferred to the postanesthesia care unit in stable condition, breathing unassisted. The patient was sent to the post-anesthesia care unit after completion of previously noted procedures. Pain postoperatively was manageable. She was continued on broad spectrum IV antibiotics, including Vancomycin.
Outcome and Follow Up
After a five-day hospital course and an extensive work-up, the patient was found to be safe for discharge home on the fifth and final day. The patient’s last obtainable vital signs at the time of discharge indicated the following: afebrile with a body temperature of 37.0 degrees Celsius, pulse rate of 60, blood pressure at 104/76, and SPO2 at 100% on room air. She also reported a pain level that was improved from previous assessments at 5/10 on the pain scale. During the patient’s final physical examination, the Penrose drain was removed. This physical exam was notable for decreased hearing in the left ear. Otherwise, there were no focal strength deficits or sensory deficits found, Kernig’s sign was negative, and the patient's neck had a completely normal range of motion.
The patient was prescribed a fourteen-day course of clindamycin, 400 mg to be taken orally every 8 hours in addition to Oxycodone-Acetaminophen, 5 mg/325 mg, to be taken every 6 hours or as needed for pain management. This patient was instructed to follow up with her ENT surgeon in approximately one week for reassessment and reevaluation.
This patient did not however return for follow-up with her ENT surgeon a week after her discharge from the hospital admission, though she did return to the emergency department several months later with a chief complaint of right sided otalgia. At that time, the patient was seen and assessed by an advanced provider, whose physical exam found that the patient was overall not ill appearing. Her neck had full normal range of motion and no signs suggestive of meningismus. Further examination of the patient’s right ear indicated that her right tympanic membrane appeared macerated and was possibly bulbous with mild tenderness to palpation to the right preauricular area, right tragus, and right pinna. There was no
apparent swelling or discharge noted. The physical exam of this patient’s left ear, including the tympanic membrane, external auditory canal, tragus, and pinna was unremarkable. The patient denied further complaints or symptoms in relation to the left ear, including left sided otalgia, hearing changes or persisting decreased hearing, pinna displacement, swelling, or discharge. No lab work is available from this visit, though records indicate that she was eventually found to be appropriate for discharge from the emergency department with a diagnosis of right otitis media. The patient was given two prescriptions for treatment of the infection and management of her discomfort - a course of Augmentin, 125 mg to be taken every 8 hours, and Hydrocodone-Acetaminophen 5 mg/325 mg every 6 hours or p.r.n. for pain.
Demographics
Due to the rarity of mastoiditis in adults overall, there are fewer case studies and overall research on the demographic, pathogenesis, and treatment of adult mastoiditis. Acute otitis media (OM) is classically seen as a childhood disorder with most incidents occurring in children between 6 months and 18 months of age [8]. One retrospective analysis using the NEDS data from 2009-2011 is consistent with this trend, noting that most patients who presented to the emergency department for OM were pediatric cases with an average age of approximately 10 years old. although OM is largely considered a childhood disorder, a significant portion of these emergency department visits (20.1%) was composed of adults with an average age of 37 years [6]. Furthermore, adults make up the larger proportion (75.9%) of complicated OM cases such as acute mastoiditis, labyrinthitis, and facial paresis (top three in that order). Though the causation of this trend in adults is likely multifactorial in nature, one suspicion is the presence of underlying adult comorbidities— such as diabetes mellitus, cholesteatoma, or chronic otitis media— which can increase the likelihood of developing complications secondary to OM [9]. Among adults, the incidence of complications from OM, including intratemporal or intracranial processes, is relatively rare, occurring in less than 0.5% of cases [10][11]. Given the rarity of this worsening progression in adults, data is particularly limited in regards to further data as most of the literature surrounding OM discusses the pediatric age group. While some studies have claimed the overall incidence of acute OM has decreased in various parts of the world [12][13][14], there is some debate as to the actual cause. A common posited possibility that increased vaccination to pathogens such as S. pneumo and H. influenzae may play a role, while others believe the stricter diagnostic criteria for acute otitis media has decreased incidence [15].
Presentation
The majority of cases of mastoiditis are preceded by an episode of acute OM with or without cholesteatoma or with chronic recurrent OM [16][17]. Many patients are seen on an initial visit, either by a primary care provider or in the emergency setting typically with complaints that include a preceding upper respiratory tract infection, unilateral otalgia, and/or reduced or muffled hearing. Pain, while often severe in children, may vary from mild to severe in adults. Initial clinical suspicions of OM should be confirmed with an otologic exam revealing a bulging tympanic membrane and reduced mobility of the membrane with pneumatic pressure. If caught at this initial stage and treated appropriately, the risk of complications is reduced drastically [3]. However, as seen in this case, patients may not present initially with OM to a provider making prior visit history unavailable. This allows time for further progression of the infection which can lead to progressive destruction and coalescence of air cells and eventual medial sinus wall erosion. Mastoiditis rarely presents in this latent form seen in our patient with no prior acute episodes or recurrent history of OM [7]. Additionally, unique to this patient is the lack of risk factors and comorbidities that may increase a physician’s suspicion of mastoiditis. The patient’s history of tobacco use and childhood asthma increase the likelihood of OM, but she did not have documented comorbidities that existing literature identifies as increasing likelihood of severe complications secondary to OM, such as diabetes mellitus, chronic otitis media, cholesteatoma, craniofacial deformities, or immunosuppression [8][18].
Not only did our patient present with clinically advanced disease on initial presentation, but she also had minimal complaints compared to what would be expected for her clinical severity. Mastoiditis typically presents with otalgia, fever, dizziness/vertigo, otorrhea, posterior ear pain, retroauricular rubor, edema of the pinna, and a posteriorly displaced auricle [1][19]. Patients may also demonstrate leukocytosis and elevated CRP, though these findings are unreliable as current research shows contradictory evidence that suggests this may be related to the causative pathogens [2][4]. In latent mastoiditis, as with this patient, we may also see symptoms of rapid clinical deterioration and progression of the infection into complications with their own clinical findings such as meningitis, facial palsy, septic thrombosis of the sinus tract, subdural empyema or brain abscesses with focal neurological findings [4][7][20]. By contrast, this patient had a fairly benign clinical presentation. She was non-toxic, afebrile, without headache, neck stiffness, or erythema. She presented with unilateral, progressive otalgia and hearing reduction, with leukocytosis seen on labs. Physical examination was significant only for mild erythema with displacement of the auricle.
What can be reasonably inferred given the available literature, however, is the significance of this
patient’s case given her remarkable presentation and progression. Firstly, there is the surprising severity of her complications given her relatively benign complaints and physical examination upon her initial
assessment in the emergency department. More noteworthy still is that this 41-year-old patient’s progression from acute otitis media was complicated not only with coalescing mastoiditis. In addition, in her case further convoluted from this point leading to getting a MRI which indicated not only mastoiditis, but the presence deep ear abscess and additional incidental findings that were consistent with meningitis. Unlike most cases with complications relating to OM, this patient required not only broad spectrum intravenous antibiotics, but required admission to medicine and surgical intervention via a left sided myringotomy with Penrose drain placement, as well as a complete tympanomastoidectomy on the affected side.
Imaging
The patient’s minimal clinical symptoms brings up concerns about how to determine when imaging is indicated. What type of imaging to order and whether imaging is clinically indicated for acute otitis media/mastoiditis is a point of much debate within the current literature. It is widely accepted that a computed tomography (CT) with contrast of the head imaging performed when mastoiditis is suspected based on clinical symptoms [19][21][22]; however, some sources say imaging should be reserved for prolonged or complicated cases [23][24]. Both of these circumstances describe our patient as she had unilateral otalgia and hearing loss characteristic of OM or mastoiditis, and her symptoms were prolonged for more than three weeks despite not having any prior medical visits to reflect this. While a CT is the best initial image of choice due to speed and availability, typical findings such as fluid in the mastoids are nonspecific and thus should be correlated with clinical and microbiology findings [16]. There is conflicting data about when Magnetic Resonance Imaging (MRI) should be utilized. While many sources recommend that MRI should always be obtained, others state recommend MRI if there is suspicion of intracranial processes (ex. intracranial abscesses or sinus thrombosis). MRI will give a better view of the soft tissue components and intracranial changes that may not be visualized by CT [2][16][22][25]. MRI findings should be utilized in combination with clinical presentation as up to 82% of patients with mastoiditis on radiology reports (increased fluid signal intensity in the mastoid air cells on MRI) did not have clinical otologic disease [26]. Due to this conflicting data, this area seems to be one where further research is needed. Overall based on the current information available, it is recommended that early imaging be performed with CT at a minimum, and MRI when available. Imaging must be evaluated in correlation with clinical presentation and microbiology findings. Imaging can be crucial as intracranial complications may be clinically silent or have insidious onsets that may otherwise be missed without imaging. This idea was supported by our case in which the patient had a clinically mild case without fever or neurologic changes, but imaging revealed serious complications including coalescing mastoiditis with erosion into the jugular foraminal space, meningeal enhancement, and an intracranial abscess.
Risk Factors
Risk factors for pediatric acute or recurrent otitis media include allergy/atopy, upper respiratory infections, and snoring. Risk factors for pediatric chronic or recurrent otitis media include second hand smoke and low social status [27]. Other noted risk factors are immunosuppression and craniofacial abnormalities [28]. While most studies of risk factors have focused on pediatric populations, many pediatric risk factors are similar and have been extrapolated to the adult population [29]. Further research to confirm these risk factors can help better guide clinical management and risk of recurrence. A majority of mastoiditis cases are secondary to acute otitis media [30]. In the pre-antibiotic era, 20% of acute otitis media cases progressed to acute mastoiditis. After the implementation of antibiotics, mastoidectomies, and vaccinations against causative organisms such as the PCV-7 vaccine, the progression rate has dropped drastically with only 0.002% of children progressing to mastoiditis. Data for adult progression is limited due to the rarity of the presentation.
Of note, our patient had a past history of smoking and asthma. Both smoking and secondhand smoke have been associated with acute otitis media and therefore mastoiditis. One possible cause for increased acute otitis media in smokers and smoke exposure is that there is an association between smoking and an increased risk of pneumococcal colonization, a primary cause of acute otitis media. [31] Attempts to establish similar findings for H influenzae risk and smoking have not been as conclusive. In the past, there were reported cases of damage to the middle ear structures and impairment of valsalva due to smoking, but attempts to confirm such a theory have been inconclusive. [32][33][34] This association requires further evaluation as smoking may present the need for more aggressive screening for acute otitis media and mastoiditis such as imaging or surgical evaluation. While the connection between allergies and acute otitis media has been well-established, connections of asthma have not been as clearly highlighted. Pediatric studies have shown correlation between asthma predicting acute otitis media later in life and vise versa but it is unclear if these trends extend past adolescence. [35]
Management
As previously mentioned, mastoiditis presents often as a complication of acute otitis media. It often occurs in the setting of untreated acute otitis media or in cases of antibiotic resistance. Patients who do progress to mastoiditis often do so after having been treated with antibiotics initially for acute otitis media. Antibiotic choice should cover the most common causes of acute otitis media including S. pneumoniae, H. influenzae, and M. catarhallis. AAFP recommends first line treatment dosage for acute otitis media as amoxicillin 80 - 90 mg/kg per day in two divided doses. Amoxicillin-clavulanate 90mg/kg per day of amoxicillin with 6.4 mg/kg per day of clavulanate in two divided doses may be considered if the patient has received amoxicillin in the last thirty days or have otitis/conjunctivitis syndrome [36].
Patients can often be treated on antibiotics for five to seven days if infection is mild/moderate. In the cases of severe infection, a ten day course of antibiotics is recommended. Supplementary workup including middle ear fluid cultures, blood cultures, and IV antibiotics may be indicated for severe presentations. Failure to respond to first line antibiotics may benefit from a change to a second line antibiotic choice such as a cephalosporin(ex. ceftriaxone) or fluoroquinolone(ex. levofloxacin or moxifloxacin). Evaluating antibiotic sensitivity of previous middle ear or blood cultures may help to guide therapeutic decisions but is often not necessary unless the patient is unresponsive or severely ill.
Most cases of acute otitis media may have subclinical mastoiditis. If initial acute otitis media is left untreated or antibiotic treatment is unsuccessful, progression to complications such as mastoiditis can occur. In such a scenario, evaluating the sensitivity of cultures is important to determine if the patient is receiving an appropriate antibiotic choice for the identified pathogen. As discussed above, indications for imaging including CT/MRI with or without contrast vary depending on clinical severity of the patients presentation. Surgery is indicated for patients with abscess formation or infected tissue evidenced on imaging in the middle ear or mastoid. Surgery may also be beneficial in maintaining the anatomical contour for acoustics or restoration of tympanic/mastoid aeration [37][38]. The most common surgical options include myringotomy, tympanoplasty, or mastoidectomy. Mastoidectomy is the most invasive of the procedures mentioned and focuses on removing infected tissue while preserving the middle ear and skull anatomy. There are multiple surgical approaches to mastoidectomy including intact canal wall and canal wall down approaches but no controlled prospective studies are currently available to compare complications or success rates. Along with surgical debridement, tools such as Penrose drains and Otowicks can assist with postsurgical management to improve drainage and topical antibiotic application respectively.
Postsurgical management often includes inpatient expectant management for complications of surgery. The patient should have the Penrose drain removed on postoperative day number two. Mastoid dressings should be changed daily until discharge and the patient is to be instructed to remove dressing two to three days after discharge for a total of five days of compression. While inpatient, patient should received continued appropriate antibiotics and be sent home with a prescription of oral levofloxacin, amoxicillin with clavulanate, or clindamycin for a fourteen day course Care should be placed in keeping the surgical site dry for a few days following discharge. It may be recommended that the patient have a second tympanoplasty with ossiculoplasty to evaluate the middle ear anatomy and any need for possible revision [39].


Mastoiditis is most often a complication of acute otitis media. If left untreated, the incidence of mastoiditis secondary to acute otitis media is 50%, however, the incidence has been estimated by some studies to have decreased to 0.4% with the introduction of antibiotics [40]. Without treatment, complications resulting from mastoiditis encompass findings such as abscess formation, labyrinthitis, meningitis, thrombosis, facial nerve dysfunction, hearing loss, and sinus occlusion [41]. Abscess formation tends to be a typical complication of coalescent mastoiditis. Bezold’s abscess is a highly uncommon deep neck/infratemporal abscess that can originate from organisms such as Streptococcus. This organism was also cultured from the intracranial abscess that required surgical intervention in our patient. While it is rather uncommon for the formation of Bezold’s abscess to occur, given the efficiency of modern-day antibiotics, reports of the abscess were more prevalent among adults with a 55.6% of documented cases, and males, 61% of documented cases [42]. Thrombosis of the sigmoid sinus, lateral sinus, and internal jugular, and facial nerve paralysis/dysfunction are both exceedingly rare complications, with almost no case reports found in adults since the initiation of antibiotics. [43] One of the more severe complications of mastoiditis is meningitis as seen in our patient’s case. We could find no other cases within the literature of meningitis developing secondary to mastoiditis, with the same demographics or presentation of our patient. Of the 4 cases referenced, 2 of the individuals were significantly older (73 y/o F and 70 y/o M), one of which had been suffering from chronic mastoiditis [44/45], and the other 2 cases describe individuals who were significantly younger than our patient (11 y/o M and 25 y/o M). All of the cases described had either chronic mastoiditis or presented with severe toxic or neurologic complications such as presenting with altered levels of consciousness. Our patient was afebrile, nontoxic, and with no neurologic findings despite having coalescent mastoiditis with an abscess and meningeal inflammation seen on imaging, making this case unique within the current literature.
Bacterial Pathogens
Bacterial cultures obtained during surgical management of the patient in our study grew S. pneumoniae with pan-sensitivity. With the development of antibiotic regimens and preventative measures such as S. pneumniae and H. influenza vaccines, the general incidence of acute otitis media declined in the last few decades. Other studies, however, have claimed that overall incidence has not changed but rather the epidemiology seems to have shifted. Proportions of causative pathogens continue to shift and include more resistant or non-typable strains of these bacteria. [46/47/48] Pediatric cases of acute otitis media were more often due to S. pneumoniae, H. influenzae, and M. catarrhalis. Pathogens involved in acute otitis media in adult cases had more variety. Some studies showed high prevalence of S. pneumoniae and H influenzae similar to pediatric populations. [49] The limited adult studies have seen H. influenzae, S. aureus (including resistant strains), and S. pyogenes as the predominant bacteria isolated. [2/50/51] Pathogens identified in adult cases of acute otitis media compared to adult acute/latent mastoiditis were similar. [2] The anaerobic bacteria Fusobacterium necrophorum has also recently been implicated in an increased proportion of pediatric acute mastoiditis although data is limited and implications for adult cases have not been pursued. [52] Pediatric studies have also seen a correlation between P. aeruginosa and recurrent acute mastoiditis. [53] These studies highlight the changing epidemiology of these disorders and continued need for research into changes in microbiological causes of acute otitis media and mastoiditis in order to guide management.
While otitis media and mastoiditis is less common in adults, cases that present often do require more aggressive treatment or surgical intervention. Because these cases are less common, patients may not know the possible risks of not treating otitis media appropriately. Key focuses for this case as well as other adult cases of mastoiditis should address presentation of symptoms, at-risk demographics, diagnostic workup/imaging, appropriate antibiotic coverage, and possible need for surgical intervention. Complications, while rare, should be considered and discussed with patients. Further studies identifying changes in common pathogens causing otitis media or mastoiditis may be beneficial.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
