
Case Report | DOI: https://doi.org/10.31579/2694-0248/068
*Corresponding Author: Suresh Kishanrao, MD, DIH, DF, FIA, FIPHA, FISCD, Family Physician & Public Health Consultant Bengaluru, India, Tel: 919810631222, 918029571102.
Citation: Suresh. K. (2023), A Rare Case of Long TNS following Caesarean Section under Spinal Anaesthesia, J Clinical Orthopaedics and Trauma Care, 5(3); DOI: 10.31579/2694-0248/068
Copyright: © 2023, Suresh. K. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 August 2023 | Accepted: 14 August 2023 | Published: 23 August 2023
Keywords: general anaesthesia; regional anaesthesia; neuraxial anaesthesia; spinal anaesthesia; transient neuronal loss (TNS)
The first regional anaesthetic technique performed was spinal anaesthesia, and the first operation under spinal anaesthesia was in 1898 in Germany by August Bier. Spinal anaesthesia (SPA) is in common use worldwide for surgical procedures involving the lower abdomen, pelvis, perineal and lower extremities. It is beneficial for procedures below the umbilicus. Currently more than 50% global surgical patients undergo spinal anaesthesia every year. It is estimated that in USA 50 million individual were given spinal anaesthesia in 2022 and in India 60% of surgeries were performed under RA in 2021 as per a recent survey.
Benefits of Spinal anaesthesia include prompt recovery, early return of normal functions, low chances of a blood clot following surgery and has less incidence of sickness, vomiting, when compared to a general anaesthetic for similar procedure. While acknowledging the benefits of SPA, Anaesthetists should be aware of and must inform clients of common side effects like acute back pain after spinal injection, that resolves with simple measures, Nausea, vomiting, headache and hypotension and Low-frequency hearing loss.
One of the rare complications called Transient Neurologic Symptoms (TNS) with symptoms of, exclusive pain in buttocks, thighs, legs, few hours to ~ 1 day, lasting up to 10 days. After initial pain patient may notice numbness usually in left buttock area and weakness in gluteal muscles involved, that may prolong for 6 months to a year. The incidence India is quoted as 10-12 cases per lakh spinal anaesthesia procedures mainly caesarean sections.
This article is of one such case the author is managing since a month. A 26-year-old lady primigravida, underwent caesarean section for the delivery 2 months ago. She was more concerned about the premature baby’s feeding challenges, but coincidentally brought to author’s notice. She has been put on a few o lower limb and abdominal muscle strengthening exercises and supplemented Tablet Neurobion (vit B12) forte one tablet a day. As of 22 /08/23 she has improved muscle power (20%) able to sit up with the support of upper and Numbness has also improved a bit.
Material & Methods: One rare case of TNS, clinical diagnosis, management, Physiotherapy, Literature review and case report studies.
The development of regional anaesthesia started with the isolation of Cocaine the first local anaesthetics. The first regional anaesthetic technique performed was spinal anaesthesia, and the first operation under spinal anaesthesia was in 1898 in Germany by August Bier. The term neuraxial anaesthesia refers to the placement of local anaesthetic in or around the CNS. Spinal anaesthesia is a neuraxial anaesthesia technique in which local anaesthetic is placed directly in the intrathecal subarachnoid space [1]. The drugs currently used for spinal anaesthesia include Lidocaine (5%), (onset of action occurs in 3 to 5 minutes with a duration of anaesthesia that lasts for 1 to 1.5 hours), Bupivacaine (0.75%- most widely used- onset of action is within 5 to 8 minutes, with a duration of anaesthesia that lasts 90 to 150 min.), Lidocaine 5%, Tetracaine 0.5%, Mepivacaine 2%, Ropivacaine 0.75%, Levobupivacaine 0.5% and Chloropropane 3% [1].
Spinal anaesthesia (SPA) is in common use for surgical procedures involving the lower abdomen, pelvis, perineal and lower extremities; it is beneficial for procedures below the umbilicus. Currently more than 50% global surgical patients undergo spinal anaesthesia every year. It is estimated that in USA 50 million individual were given spinal anaesthesia in 2022 and in India 60% of surgeries were performed under RA in 2021 as per a survey [2].
Benefits of Spinal anaesthesia include prompt recovery, early return of normal functions, low chances of a blood clot following surgery and has less incidence of sickness, vomiting, when compared to a general anaesthetic for similar procedure. It is a very essential component of anaesthetic practices towards safer anaesthesia and should not be undermined as an option. While acknowledging the benefits of SPA, Anaesthetists should be aware of, and must inform clients of common side effects like acute back pain after spinal injection, that resolves with simple measures, Nausea, vomiting, headache and hypotension and Low-frequency hearing loss. Hypotension after spinal anaesthesia is a physiological consequence of sympathetic blockade. SPA has been commonly linked to low back aches especially in patients who have had a caesarean section.
It is common to experience itchiness and numbness around the C-section scar, caused by damage to the nerves during your operation. In some women, numbness begins to improve after 4-8 weeks, whilst for other women, their scar remains numb for long or even lifetime. Rare Neurological complications include subdural haematoma, cerebral uncus herniation, intracranial haemorrhage, paresis of cranial nerves, pneumocephalus, visual disturbance and sensory and motor deficit at and below the level of Dural puncture. While usually a single nerve is affected, giving a numb area on the skin or limited muscle weakness, total spinal nerves damage is a rare complication of spinal or epidural injection.
Transient neurologic symptoms (TNS) after spinal anaesthesia (SPA) are defined as back pain with radiation or dysesthesia in the buttocks, thighs, hips, and calves, occurring within 24 h after recovery from otherwise uneventful SPA. These effects are usually temporary with full recovery occurring within days or a few weeks rarely taking months. Transient Neurologic Symptoms (TNS) include, exclusively pain in buttocks, thighs, legs, with no dysfunction, occurring few hours to ~ 1 day, after SPA and lasting up to 10 days. After initial pain patient may notice numbness usually in left buttock area and weakness in muscles involved., that usually lasts for 6 months or more with slow improvement. Based on personal experiences two of aesthetic friends put the incidence of TNS around 12 per 10,000 SPA they have done over 20-30 years. Indian studies report an incidence of 10-12 cases per 100,000 SPAs. More than a decade ago 125 consecutive caesarean section patients were studied in a facility that documented TNS were in 12 (10%) patients [7]. In another systematic analysis of 14 trials, reporting 1,349 patients, 117 (8.7%) developed transient neurologic symptoms. The use of lidocaine for spinal anaesthesia increased the risk of developing TNS {8}
This article is based on a recent case of TNC seen last month in a young Primigravida undergoing caesarean section 2 months ago and continued TNC on left side, followed by literature review.
Just last week a close friend of mine in our apartment complex called asking for consultation for breast feeding problem of his grandson born 2 months ago. When I visited the mother and the baby on 09/08/23 and addressed the baby’s attachment and suckling problems. At the end of the half an hour counselling the mother of the baby, a young lady of 26 years, Primi-gravida slowly opened and complained that she feels numbness on the left gluteal region and some radiating pain from gluteal region to feet on the left side 2-3 times a day for 10-20 minutes. To assess the sensory loss, I did first the pinprick and skin pinch test that were almost normal. Further detailed physical examination confirmed loss of cold and fine touch sensation over left gluteal region. There was no haematoma at the SPA site. The muscle power in limb raising and lateral upward movement was much less on left side when compared to the right side, though she was able to lift almost to 600 angles. She was unable to sit from sleeping position on both sides even with upper extremity support. Straight propping up in prone position was also not possible. The history revealed that she had undergone caesarean section under spinal anaesthesia and was advised to rest for the first fortnight. As precaution after coming home after the delivery she had not made any active exercise efforts. Suspecting post-spinal anaesthesia Transient Neuron loss, I put her a few exercises to lower limb and abdominal muscle exercises and supplemented Tablet Neurobion (vit B12) forte one tablet a day. the exercises included i) Squats ii) Clam: lie on your side with your knees bent and feet together. Lift your top knee up as high as you can, squeezing your glutes.
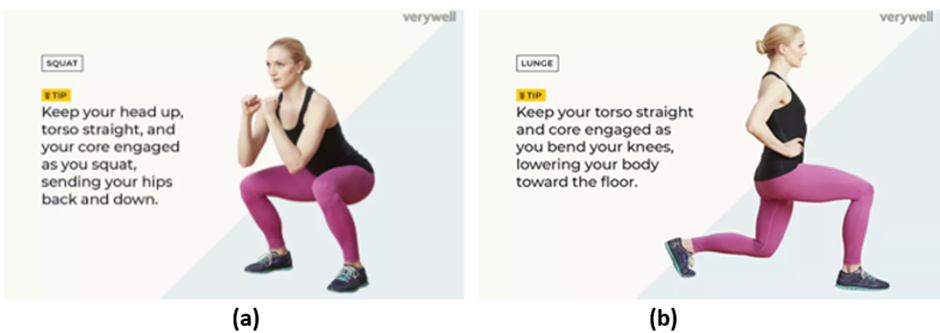
Figure 1: (a) Squats; (b) Clam: lie on your side with your knees bent and feet together
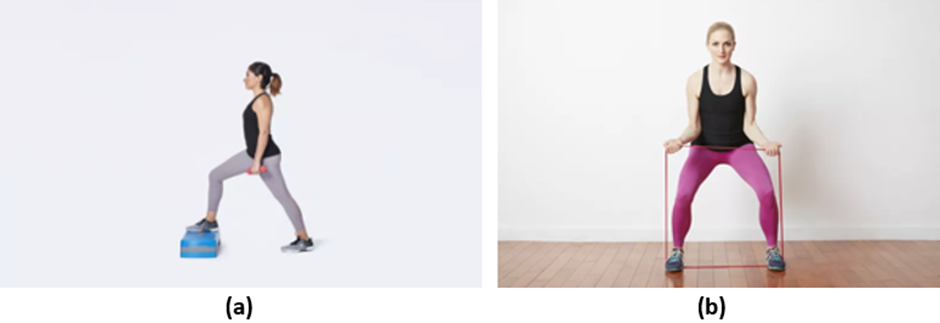
Figure 2: (a) Step-ups; (b) Sidestep squats with Resistance
Lateral banded walks-by placing a resistance band around the legs, just above the knees iii) Curtsy lunge iv) Step ups v) Sidestep squats with resistance, vi) Hip extension.
As of 22 /08/23 she was able to sit up with the support of upper extremities and muscle power improved by 20%. Numbness has also improved a bit.
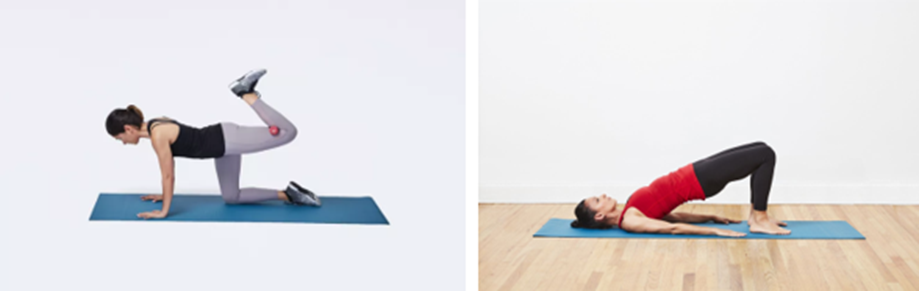
Figure 3: (a) Hip Extension; (b) Bridge.
Patient safety, improved quality of care, and better patient satisfaction and functional outcomes are currently the topmost priorities in regional anaesthesia (RA) in recent times. Ultrasonography-guided central neuraxial and peripheral nerve blocks, intra-cluster and intra-truncal injections, fascial plane blocks, diaphragm-sparing blocks, continuous local anaesthetic wound infiltration are of clinical interest.
Transient Neuronal Sensory loss (TNS) is experiencing some numbness after an epidural, which is caused by the aesthetic, and it typically goes away within several hours, potentially up to four to six hours. To avoid injury, the patients are advised to remain resting until this numbness subsides. Left buttock area is the commonest site. Pinprick and cold are the earliest most lost sensation and are used for diagnosis as I did in our care. Mechanical stimuli such as touch, skin pinch, pressure and gas jets can be used to test. Generally, loss of sensation to cold occurs before pinprick, and both before touch, each stage correlating with inhibition of C, Aδ and Aβ fibres respectively.
All local anaesthetics can cause TNS. The incidence of TNS following lidocaine was 1:7 (13%). The relative risk of TNS when using lidocaine (versus bupivacaine, mepivacaine, prilocaine, or procaine) is 4.35, based on an analysis of 14 studies including 1347 patients [6]. Twenty-four neurological complications attributable to spinal anaesthesia were found in a series of 20,000 consecutive spinal anaesthetics, an over-all incidence of 0.12 per cent [6].
Nausea and vomiting occur significantly more frequently during spinal anaesthesia for caesarean section compared to non-obstetric surgery and are primarily caused by hypotension. Acute hypotension reduces cerebral perfusion, induces transient brainstem ischemia, and activates vomiting centres.
The sequence of return of neurological activity following tetracaine subarachnoid block is sympathetic nervous system activity, pinprick sensation, somatic motor function followed by proprioception in the feet. Autonomic fibres are blocked first, followed by sensory loss to touch/pinprick, followed by loss of proprioception, and lastly motor loss [5]. The return will also be in the same order. Some patients may have residual numbness lasting more than 6 months, and some cases feel better within 6 months after surgery.
In contrast in lumbar disc herniation patients, pain and numbness of the lower extremities are the typical symptoms, which disturb walking ability and limit their activity of daily living.
Spinal cord has 31 spinal nerve roots, each providing sensory innervation to a dermatome or a specific area of skin. A sensory block that extends from the sacral dermatomes to T4 is needed for caesarean delivery as afferent nerves supplying abdominal and pelvic organs accompany sympathetic fibres that travel in the sympathetic trunk (T5 to L1). For caesarean section delivery T4-6 spinal level is chosen for injecting local anaesthetic. To administer spinal neuraxial anaesthesia, a needle is inserted through the ligaments between the vertebrae and a one-time injection of medication of 1 to 2 mL of local anaesthesia without an opioid is placed into the subarachnoid space. Local anaesthetics work by bathing the nerve roots of the spinal cord, inhibiting sodium channel transmission to block pain signals to the central nervous system. The commonly used local anaesthetics for neuraxial anaesthesia are lidocaine, bupivacaine, and ropivacaine. Single spinal injections generally last 60 to 150 minutes.
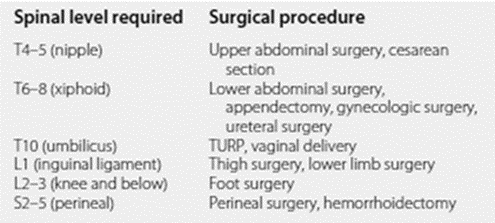
Figure 4: Spinal anaesthesia levels - based on Surgical Procedures.
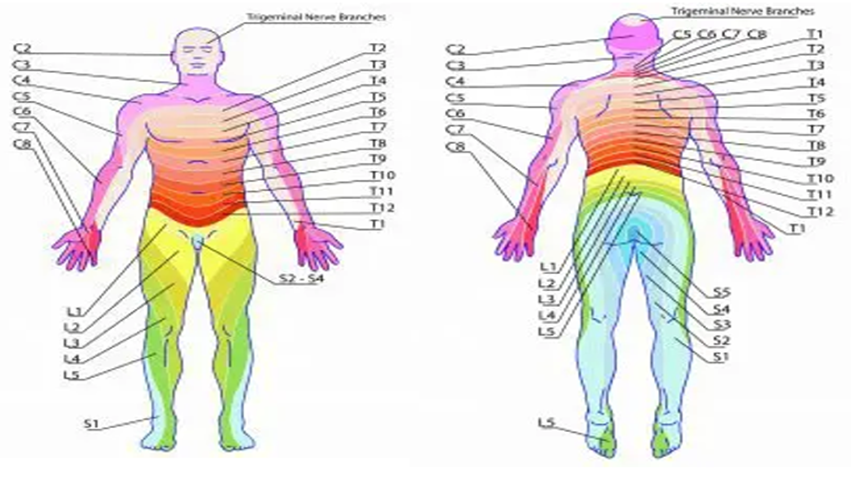
Figure 5
In a year 2121 survey of anaesthetists, they reported preferred position of the patients among 2141 responder’s anaesthetist in a span of 4 months (1 January 2021 to 30 April 2021) as Lateral- 26.6%, patients’ comfort- 26.6% and sitting-46.7. Incidence of post-dural puncture headache was reported to be Less than 2% by 1881 (88.7) anaesthetists, 2%-5% byc208 (9.8) anaesthetists and more than 5% in 30 (1.4%). Perineural catheters for post-operative analgesia was used in 492 (23.5%) patients. Post anaesthetic complications seen were: i) Haematoma= 588 (28.2), ii) Need of IV injection for hypotension management-540 (25.9), iii) LAST= 343 (16.4), iv) Nerve injury= 232 (11.1) and none= 829 (39.8) [2]. Epidural catheters were commonly used by 89% of the respondents, However, peri-neural catheters for post-operative analgesia were not that commonly used (23.5%) by the responders {2].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
