
Case Report | DOI: https://doi.org/10.31579/2690-1897/113
1 Department of General Surgery, Sapthagiri Institute of Medical Sciences & Research Center, Bangalore.
2 Department of Pharmacy Practice, Sri Adichunchanagiri College of Pharmacy, Adichunchunagiri University, B G Nagara.
*Corresponding Author: Manisha H M, Department of Pharmacy Practice, Sri Adichunchanagiri College of Pharmacy, Adichunchunagiri University, B G Nagara.
Citation: Ashok V Kulkarni, Sreenivas M Doddasamiah, Melkote J Avinash, Ramesh M Tambat, Suhas Pandarinath, Manisha H M. (2022). A Rare Case of Giant Cell Tumor of The Extensor Hallucis Longus Tendon Journal of Surgical Case Reports and Images 5(3); DOI: 10.31579/2690-1897/113
Copyright: © 2021, Manisha H M. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 04 May 2022 | Accepted: 20 June 2022 | Published: 02 July 2022
Keywords: giant cell tumor; extensor hallucis longus tendon sheath; synovial cyst; giant cell tumor; nuclear magnetic resonance
Giant cell tumor is a benign tumour of the extremities that is more prevalent in the upper limbs and less common in the foot and ankle region. We present a case of a patient with a lobulated lesion on the dorsum of the foot that turned out to be a giant cell tumor of the extensor hallucis longus tendon sheath. The likelihood of treatment success is increased by doing a differential diagnosis of a "synovial cyst" in the foot and ankle, completing sufficient surgical planning, and using imaging tests such as nuclear magnetic resonance. Giant cell tumor of tendon sheath involving the foot and ankle region is a rare clinical entity, and good results can be expected after surgical excision
tissue tumors and were originally known as giant cell tumors of the tendon sheath, nodular tenosynovitis, or pigmented villonodular synovitis. They are more common in women (F:M = 2:1), afflict individuals between the ages of 30 and 50, and are usually benign [1]. It's a locally aggressive but mostly benign tumor that affects joints, tendon sheaths, and bursae [2,3].
Multinucleate large cells, siderophages, foam cells, and inflammatory cells are all present in these lesions. They have at (1,2) translocation involving the colony-stimulating factor 1 gene (CSF1) and, most commonly, the COL6A3 gene, which codes for collagen type 6, Chain alpha-3. The elevated amount of CSF1 caused by this translocation is hypothesized to influence the inflammatory infiltrate seen in these tumors [4,6]
There are three types of lesions: nodular, diffuse, and focal and malignant—each with its own set of biological characteristics [7]. The most abundant large cells are found in the nodular form, which is often a well-circumscribed nodule in the digits. The diffuse form, on the other hand, has infiltrative borders and can be intra-articular. It most usually occurs in major joints (e.g., knee, wrist, foot) or surrounding soft tissue (e.g., thigh). The fibularis brevis, flexor hallucis longus, extensor hallucis brevis, extensor hallucis longus (EHL), Achille’s tendon, and Tibialis posterior have all been implicated in the foot. Increased mitotic count and nuclear dysmorphism are seen in the malignant form; these tumors are likely to contain other genetic abnormalities (other than the COL6A3-CSF1 translocation) that drive disease progression. Malignant TGCTs can spread to the lungs and lymph nodes. These are uncommon tumors, according to a recent Dutch registry [8].
According to the study, diffuse TGCT has a global incidence of 4 cases per million, nodular TGCT has a global incidence of 10 cases per million, and digit TGCT has a global incidence of 29 cases per million [8].
Although endoscopic resection for mild and well-located foot injuries has been recorded, open surgical therapy is the most generally used and recommended treatment. Nodular tumors have a recurrence rate of 10% to 20%, but diffuse-type tumors have a recurrence rate of 18% to 50% [8].
The aim of this study was to describe a rare case of a patient who presented to our general surgery out-patient department with an extensive lesion on the dorsum of the foot, which was demonstrated by MRI and had the characteristics of a TGCT, affecting the entire length of the EHL, and the difficulty of resecting it without causing neurovascular and functional deficits in the patient [8].
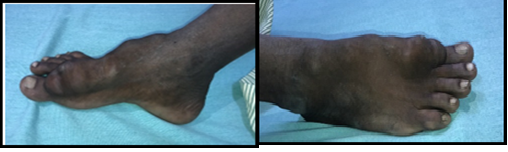
A 26-year-old male patient complained of swelling across the dorsum of his right foot for the past three years, with significant growth in the previous four months and concomitant pain for four months. four years ago, the place was reported as having a history of trauma.
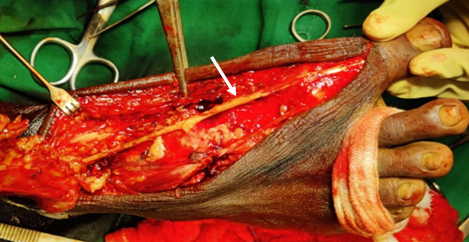
On examination, a 14x4x4 cm swelling over the dorsum of the right foot was detected, extending from the head of the proximal phalanx of the great toe up to 2 cm distal to the ankle joint, with varying consistency (firm-hard) and restricted mobility. The affected foot has no functional limitations or neurovascular deficits (Figure 1).
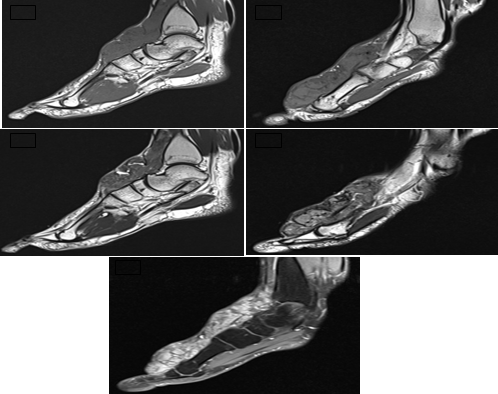
The EHL tendon was encased by a very well-defined extra-articular variegated hyperintense heterogeneous soft tissue lesion measuring 14.8x3.8x3.4 cm (APxCCxTR) on MRI, raising suspicion of a TGCT throughout the EHL. The needle biopsy result coincided with the above-mentioned diagnosis.
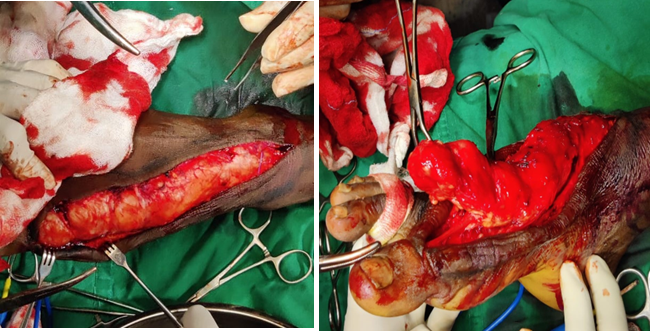
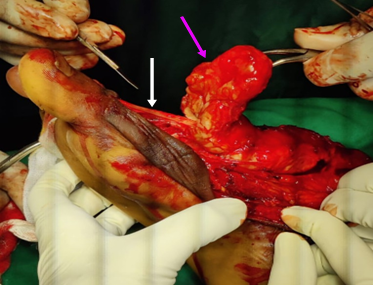
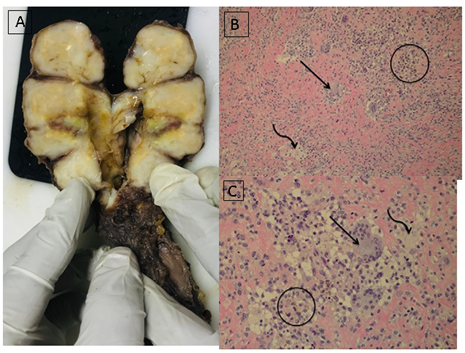
In this case, an 18-20 cm S-shaped curvilinear incision was made from the right hallux's distal interphalangeal joint to the proximal anterolateral ankle region (Figure 3). The deep peroneal nerve's medial and intermediate dorsal cutaneous branches, as well as the dorsalis pedis artery, were dissected. There was a tumor covering the entire EHL sheath (Figure 4), as well as multilobulated, soft, yellowish brown tumor tissue with TGCT features (Figure 5). The lesion was completely excised beneath the extensor retinaculum at the ankle, without the need to expose the extensor retinaculum and without causing any damage to the neurovascular systems or the EHL (Figure 6). The diagnosis of diffuse tenosynovial giant cell tumor (or pigmented villonodular tenosynovitis) was confirmed when the tumor was excised and sent for histological testing (Figure 7). The histological findings shows that specimen consists of grey white to grey brown linear mass. External surface was nodular. Cut surface was grey white to grey yellow solid with nodules. Tendon consists of grey white to grey brown nodular tissue bits measuring 3×1×1cm. Cut surface grey white. Tumor was composed of sheets of mononuclear cells around to polygonal in shape. Also hemoseridin laden histocytes scattered osteoclast like gaint cells admixed with sclerotic stroma. The final diagnosis was Gaint cell tumor.
Regular follow-up is required due to the high rates of recurrence, and a third month follow-up performed on an outpatient basis indicated no evidence of relapse. The patient's wounds were healing well and he had no neurofunctional deficits in his foot (Figure 8 & Figure 9).



GCT-TS is a benign tumour of the extremities that is more prevalent in the upper limbs and less common in the foot and ankle region [9], despite being the second most common site [10].It is thought to come in two forms: diffuse and localized [11,12], with the latter accounting for 88 percent of cases in the hands and feet10. After ganglion cysts, plantar fibroma, epidermal inclusion cysts, lipoma, and rheumatoid nodules, GCT-TS is the sixth most frequent benign tumour of the foot.13 In 207 instances, Ushijima et al found a 5% rate of GCT-TS in the foot and ankle [14].
Although the exact cause of this illness is unknown, it has been linked to an inflammatory or neoplastic process, as well as the existence of clonal abnormalities under microscopy [10,14]. The role of past trauma as a cause of the lesion is debatable [13,14].
Histological results reveal a well-differentiated lesion with multinucleated large cells and destructive proliferation of synovial-like mononuclear cells with villonodular architecture, collagenized stroma, hemosiderin pigments, and inflammatory cells [14].
The tumour normally appears as a painless, palpable, solid, well-defined mass with or without mobility, and depending on its location or proximity to the joints, it might cause discomfort when walking or impede movement of the foot and ankle [13,15]. Only 15% of the patients have a visible tumor [13].
On T1 scans, iso- or hypointense pictures with uneven contours and hypointense foci appear on MRI. The extensive collagen stroma12 and the paramagnetic action of hemosiderin are responsible for these properties.
Desmoid tumour, fibroma, cavernous haemangioma, ganglion cyst, fibrosarcoma, chondroma, or gouty tophus are all possible diagnosis. None of these organisms, however, contain hemosiderin [9].
The recurrence rate of GCT-TS ranges from 0% to 33% [11,14], with some studies reporting values as high as 44% [12,13]. High recurrence is linked to incomplete excision, cellularity, and mitotic activity of the tumour, as well as the existence of bone erosion [14].
The open routes used to remove the tumour completely, allowing direct sight of the lesion and surrounding structures [10-12,16]. The endoscopic approaches best used when the lesion is small and well-localized, which necessitates the use of a skilled arthroscopy specialist to avoid injury to nearby tissues or insufficient tumour removal [14,17].
To prevent recurrence, some authors utilize adjuvant local therapy, such as hydrogen peroxide or radiotherapy [12,15].
We infer that understanding the anatomy of the foot, as well as a thorough resection of vast lesions with high relapse rates, such as GCT-TS, are essential for effective treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
