
Case Report | DOI: https://doi.org/10.31579/2690-4861/224
1 Chief interventional cardiologist, Vivekananda hospital, durgapur .
*Corresponding Author: Arnab Ghosh Chaudhury, Ex-assistant professor of cardiology, sri jayadeva institute of cardiovascular sciences & research., bangalore. (Currently working as consultant cardiologist at Vivekananda hospital, Durgapur)
Citation: Arnab G. Chaudhury, (2022) A rare case of dual left anterior descending arteries arising from left main coronary artery and right sinus of Valsalva. International Journal of Clinical Case Reports and Reviews. 11(3); DOI: 10.31579/2690-4861/224
Copyright: © 2022 Arnab Ghosh Chaudhury, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 May 2022 | Accepted: 27 May 2022 | Published: 10 June 2022
Keywords: dual left anterior descending artery; coronary anomaly
Duplication of left anterior descending (LAD) artery is an uncommon coronary anomaly. Type IV dual LAD is the rarest variety where short LAD arises from left main stem and long LAD arises from right coronary artery or right sinus of Valsalva. I present a case of 60-years-old lady with dilated cardiomyopathy with incidental detection of type IV dual LAD during coronary angiography. The patient was treated conservatively
Coronary anomalies are uncommon. Incidence ranges from 0.6% to 1.3% in various case series [1,2]. Duplication of left anterior descending artery (LAD) is rare [3]. TYPE IV dual LAD [4] is the rarest variety where short LAD arises from left main coronary artery and long LAD arises from either right coronary artery (RCA) or right sinus of Valsalva. I report a case of TYPE IV dual LAD detected incidentally in a patient of dilated cardiomyopathy (DCM) during coronary angiography.
A 60-years-old female patient, known diabetic and hypertensive on medications, presented with exertional dyspnoea for last 6 months with New York Heart Association (NYHA) class II severity. Electrocardiogram (ECG) was normal with sinus rhythm. Echocardiogram revealed dilated left ventricle with global hypokinesia with ejection fraction of 30%. Diagnosis of dilated cardiomyopathy (DCM) was made. Coronary angiography (CAG) was performed to rule out associated coronary artery disease. CAG revealed: in the left coronary system, left main artery trifurcated into a short left anterior descending (LAD) artery, a ramus intermedius branch and non-dominant left circumflex (LCX) artery (FIGURE 1, FIGURE 2). The short LAD gave rise to few small septal branches and terminated in anterior interventricular sulcus (AIVS) well before reaching the left ventricular apex (FIGURE 1, FIGURE 2). The right coronary system revealed the right coronary artery (RCA) was dominant and normal (FIGURE 3). Another long artery was arising from the right sinus of Valsalva near the origin of RCA, it reached the AIVS, gave rise to numerous diagonal and septal branches and terminated in left ventricular apex (FIGURE 3). So, this artery was identified as dual LAD type IV (FIGURE 3). All coronary arteries were normal in calibre without any flow limiting lesion. CT coronary angiography was advised to further delineate the course of anomalous long LAD and its relation to great arteries. But the patient was not willing for further investigations. Patient had the final diagnosis of nonischaemic DCM with stage C heart failure with normal coronaries with diabetes and systemic hypertension. Patient was treated conservatively and she is doing well with regular follow up visits.
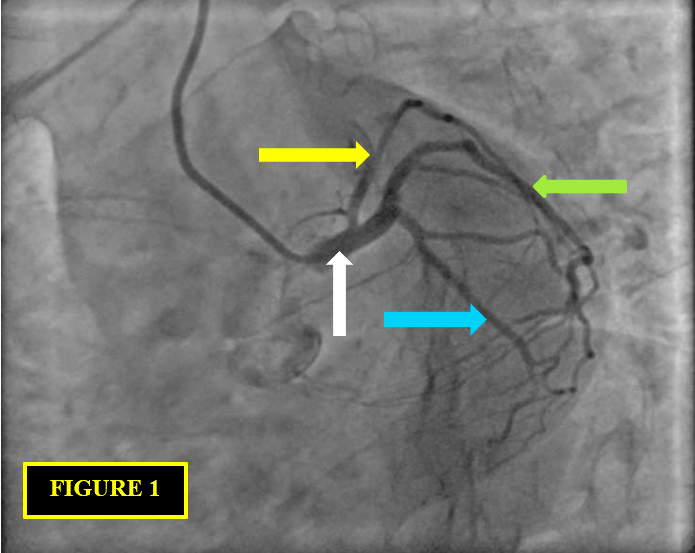
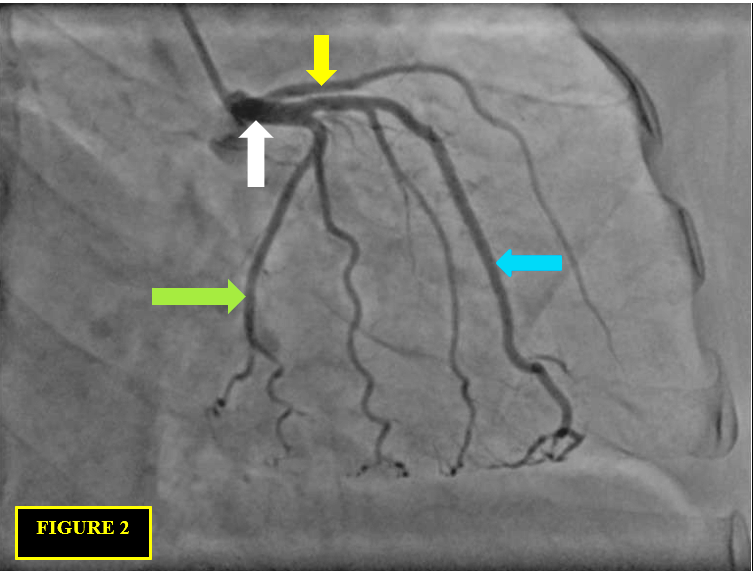

LAD has the most constant course among all the coronary arteries. Dual LAD consists of two branches [4] which supply the usual distribution of the LAD. One branch (short LAD) terminates in the proximal aspect of the AIVS. A second, longer branch has a variable course outside the AIVS and returns to the AIVS distally. Spindola-Franco et al. [4] first described and classified dual LAD into four types based on the origin, course and termination of the long and short LAD. The classification is as follows: Type I: The short LAD runs in the AIVS and is generally the source of all major proximal septal perforators. The long LAD also runs in the AIVS, descending on the left ventricular side of the AIVS, re-entering the distal AIVS to reach the apex. Type II: The short LAD is the same as in type 1, but the long LAD descends over the right ventricular side before re-entering the AIVS. Type III: The short LAD is consistent with that in types 1 and 2. The long LAD travels intramyocardially in the ventricular septum. Type IV: The short LAD originates from the LMCA. The major septal perforators and the diagonal branches originate from this vessel. The long LAD arises from the RCA. It is extremely rare among the four types. In my case, the short LAD was arising from left main coronary artery and was terminated in AIVS before reaching the left ventricular apex (FIGURE 1, FIGURE 2). The long LAD originated from right sinus of Valsalva near RCA origin, reached AIVS, gave multiple septal and diagonal branches and terminated at left ventricular apex (FIGURE 3), fulfilling the criteria of type IV dual LAD as per the description of Spindola-Franco et al. (4). With newer anomalies being reported dual LAD was reclassified into six types by Lee et al (5) (TABLE 1). In this newer classification [5] types IV, V, and VI have one of the LADs arising from the right coronary circulation. CT coronary angiography is essential to subclassify right sided origin long LAD as per Lee et al [5] because it describes the relation of long LAD with RVOT and aortic root. Unfortunately, in our case we could not do the CT imaging as the patient was not willing.

Most of the coronary anomalies are benign and do not necessitate any form of intervention [6]. In my case, there was no flow limiting lesion in coronaries. So, the patient was treated conservatively. Type IV variant of dual LAD is very rare and can be missed on angiography [7]. In acute coronary syndrome situations, in presence of flow limiting lesions, proper assessment of the angiogram and knowledge of the coronary anomalies is required during percutaneous coronary interventions and surgical revascularization.
I would like to thank my wife, Dr Debsmita Roy, DM Gastroenterology, for her constant support and encouragement. Thanks to my cathlab team for their active participation: Abhirup Mukhopadhyay, Riju pal, Suman saha, Augustine Karthik, Subham das, Bulbul adhikary. My sincere thanks to CMD Mr Sujit dutta, MD Mrs Basabdutta dutta, TD Mr sumanjit dutta, CMS Dr Durgadas roy, CMO Mrs Antara ganguly, for their support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
