
Case Report | DOI: https://doi.org/10.31579/2690-4861/219
1 Cardiology division, Beirut Cardiac Institute, Lebanon
2 Pulmonary division, Beirut Cardiac Institute, Lebanon
3 Radiology division, Beirut Cardiac Institute, Lebanon
4 Cardiology division, Beirut Cardiac Institute, Lebanon
5 Cardiovascular surgery division, Beirut Cardiac Institute, Lebanon
*Corresponding Author: Zahra Nassereddine, Cardiology division, Beirut Cardiac Institute, Lebanon.
Citation: Nassereddine Z., Charif F., Nassar P., Khatoun H, Abbas I., Mohamad S.. (2022) Clinical Decision Making: A Rare Case of ALCAPA In Adult Asymptomatic Patient and Unusual Collateral Circulation: A Case Report. International Journal of Clinical Case Reports and Reviews. 11(5); DOI: 10.31579/2690-4861/219
Copyright: © 2022 Zahra Nassereddine, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 May 2022 | Accepted: 17 June 2022 | Published: 17 August 2022
Keywords: ALCAPA; Left to right shunt; Collateral circulation; ischemic cardiomyopathy; computed tomography coronary angiography
Anomalous Origin of the Left Coronary Artery from Pulmonary Artery (ALCAPA) syndrome is a rare congenital anomaly where the left main coronary artery arises from the pulmonary artery (PA) and the right coronary artery (RCA) originates normally from the aorta. The rapid decrease in pulmonary vascular resistance (PVR) soon after birth reverses the blood flow to the PA resulting in a left to right shunt and severe left ventricle (LV) ischemia. Left untreated, this congenital anomaly is associated with premature death. Rarely, some patients can survive to adult age due to development of collateral circulation usually from an ecstatic RCA. Most adult patients with ALCAPA die at mean age of 35 years. Very few cases were reported in the literature to survive until late 40s or 50s. We present the case of ALCAPA in an asymptomatic 54-year-old woman who found to have unusual collateral circulation justifying the absence of significant symptoms. Our patient underwent surgical correction with good results. We also review cases of ALCAPA that has been reported in the literature and we summarize treatment strategies.
Learning objective: recognition of ALCAPA as one of coronary anomalies in adults even in asymptomatic individuals and recognition of the best diagnostic modality and the optimal management according to available literature.
ALCAPA is a rare congenital abnormality that affects one of every 300 000 live births and account for 0.25 to 0.5 Percent of congenital heart defects [1, 2]. It is usually an isolated defect but can be associated with other congenital heart disease in 5 Percent of cases. In patients with ALCAPA, the left main common coronary artery (LCA) arises from the PA while the RCA originates normally from the aorta. After birth, the PVR decreases substantially and causes blood flow reversal from abnormal LCA to the PA resulting in left to right shunt. The ensuing coronary ischemia leads to left ventricle infarct and dysfunction, functional mitral regurgitation, arrythmias and ultimately death [1,2,3]. The diagnosis is usually made at 1 or 2 months of age. If left untreated up to 90 Percent of affected infants die within 1 year [3]. In rare cases, patients are diagnosed in childhood or adolescence.
We present the case of a 54- year-old lady who was referred by her primary care physician to cardiology division because of abnormal electrocardiogram during a routine medical examination. At presentation, she denied any serious symptoms of chest pain or dyspnea besides some episodes of shortness of breath during emotional stress. Her past medical history and her family history are insignificant. She had good general status and her physical examination was unremarkable. Her electrocardiogram showed sinus rhythm with nonspecific repolarization abnormalities. On echocardiogram, she had hypokinesia of the left ventricular anteroseptal wall with preserved global systolic function. Mitral valve was normal in structure and function, and the right ventricle was normal in size and function. The patient was referred for coronary angiography that failed to opacify the left main coronary artery origin despite the use of multiple transradial and transfemoral catheters. While, a huge tortuous RCA originating normally from the right coronary cusp is visualized. This big dominant artery bifurcates and terminates in collaterals that communicate to and allow retrograde filling of the left coronary artery (fig 1).
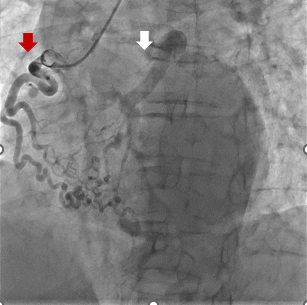
Figure 1: Coronary angiography, the injected RCA appears ecstatic and tortuous (red arrow) with collaterals to left coronary artery (white arrow), visualized by retrograde opacification.
Subsequent cardiac computed tomography coronary angiography (CTCA) showed the left main coronary artery arising abnormally from the pulmonary trunk, and the big dominant RCA was identified again terminating distally in a network of collaterals connecting to the left coronary system (fig 2). Furthermore, a high suspicion of vascular connection between a dilated bronchial artery and the left coronary system via small branches was raised but not well visualized because of limited window (see video), this finding was confirmed later intraoperatively. Due to high risk of sudden cardiac death even in asymptomatic patients and in light of previous recommendations, we decided to adopt the option of surgical correction over conservative management after discussion with the patient.
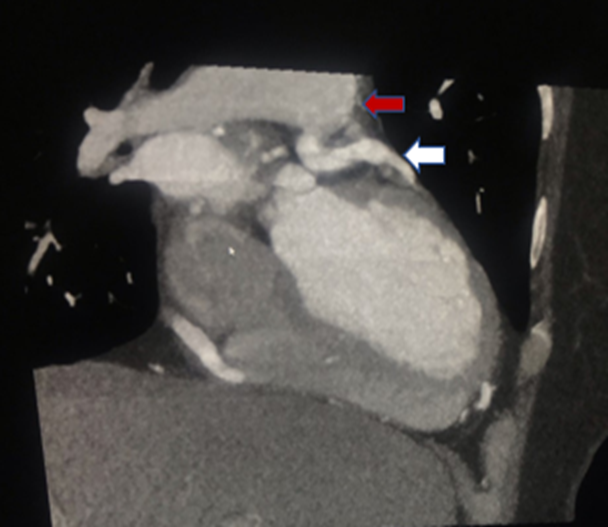
Fig 2: CTCA showing the LCA (white arrow) arising from the pulmonary trunk (red arrow).
After median sternotomy, the cardiopulmonary bypass circuit was obtained with aortic and vena cava canulation and cardioplegia infusion was started. The coronary reimplantation surgery deemed technically impossible, therefore the option of left coronary ligation with coronary artery bypass grafting (CABG) was considered. Importantly, the surgical team noted continuous and significant blood flow despite cardioplegia. Cardiac arrest was never complete. There was a high suspicion of another source of blood flow to left coronary system in addition to collaterals arising from RCA, likely originating from the bronchial arteries. The surgeon identified and ligated the abnormal LCA origin in the pulmonary trunk, and the ostium is closed using a pericardial patch (fig 3). Then, the surgery is continued classically by doing end to end anastomosis using left internal mammary artery to left anterior descending artery and right internal mammary artery to marginal coronary artery. The postoperative course was smooth and she was discharged on day 5 with recommendations of close cardiac follow up. She was completely asymptomatic on follow up visits during the following 9 months.
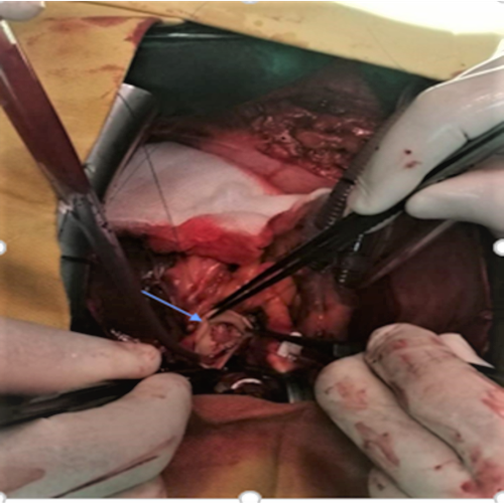
Fig 3: Intraoperative picture: Suturing the LCA ostium (arrow) in the pulmonary artery.
ALCAPA is diagnosed usually in early post-natal period. In the infantile type, there are no collaterals to the abnormal LCA and most infants die without surgical correction. The echocardiography is essential for the diagnosis and shows ischemic cardiomyopathy and functional mitral regurgitation in addition to direct visualization of the coronary ostia. In adult type, a collateral circulation connects a big RCA to left coronary system and minimizes myocardial ischemia. Hence, patients may be asymptomatic or mildly symptomatic until childhood or adolescence according to the presence and extent of intercoronary collateral circulation. Most patients experience various degree of symptoms ranging from palpitations to arrythmia and sudden death. Rarely, some patients are asymptomatic until late adult life (after 50s). The protective mechanism in this age is usually due the presence of ostial LCA stenosis attenuating the steal phenomenon or very rarely due to communication between LCA and enlarged systemic arteries namely bronchial arteries, in addition to RCA collaterals [4]. The diagnosis is made mainly by computed tomography coronary angiography that confirm the abnormal LCA arising from the PA. All adult cases have collaterals to left coronaries originating from a big ecstatic RCA [1,5]. These patients are prone to arrhythmias due to myocardial scarring or ischemia. The risk of sudden death is significant, up to 90 Percent at the age of 35 years [3]. It is the first presentation in some cases. Once ALCAPA is diagnosed, surgery should be performed immediately [3,6,7]. There are 4 main surgical options described in literature: simple ligation of ALCAPA, coronary artery bypass grafting, channel repair (Takeuchi surgery) and coronary artery reimplantation. The last technique is the ideal option for ALCAPA and is more feasible in neonates due to vascular flexibility, but the coronary artery bypass grafting is the most commonly used in adults worldwide [5]. A comprehensive review of 151 adult patients from 1908 to 2008 done by JM Aui et al. [8] showed that minority (14 Percent) were asymptomatic and most of the patients underwent successful surgical correction, furthermore, the risk of sudden death was elevated in these patients especially at younger age, and decreased with age. The authors suggest that conservative treatment is preferred in older patients aged more than 50 years due to elevated surgical risk in favor of lower sudden cardiac death risk [8]. Other small series of ALCAPA in adults were published in recent literature, most of them underwent surgical correction with good final results few months later [6]. Few cases are reported individually; most of them are females, aged between 20 to 50 years [3,9], rarely after 50 years and extremely rare cases older than 75 years. The majority of young patients had symptoms of palpitations and exertional dyspnea while the presentation in older patients is more benign; in some cases, they are completely asymptomatic and had incidental diagnosis. A substantial number of young patients are diagnosed after tachyarrhythmias or sudden death during exercise, most of them had ICD implantation for secondary prevention. Almost all patients less than 50 years had surgical correction with different techniques: reconstruction, reimplantation, or CABG with good results on follow up. Even though there is no evidence that surgery abolish the risk of arrythmias, the risk appears much lower after surgical correction. The ventricular arrythmias can be due to local ischemia or reentrant circuit around a scar or due to electrical instability in the fibrotic myocardium. ESC guidelines 2021 recommend ICD implantation in adult’s patients with congenital heart disease after aborted sudden death due to ventricular fibrillation or ventricular tachycardia after exclusion of reversible causes [10]. In absence of specific recommendations, ICD implantation decision should not be mandatory in all individuals for secondary prevention undergoing surgery as a reversible etiology can be eliminated by surgery especially in older patients, unless high risk features on clinical and imaging studies. Furthermore, in surgically treated high risk patients, a carefully evaluation for ICD implantation for primary prevention purpose could be helpful. A subcutaneous ICD seems an attractive option with lower risk of infection.
Our case represents a rare presentation of ALCAPA in a 54-year-old asymptomatic patient and unusual collateral circulation to left coronary artery from bronchial arteries in addition to RCA collaterals explaining the complete absence of symptoms at this age. The patient underwent successful surgical correction with good final results. Indeed, the surgery should be offered to all patients when diagnosis is made except for those asymptomatic individuals aged 75 years or more. Such patients could be evaluated individually and decision is made after discussion with the patient. The chosen surgery depends on age and technical feasibility.
Ms. Lina Hneineh, her effort in images collection and arranging patient follow up is valuable.
The authors declare that they have no conflict of interest.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
