
Case Report | DOI: https://doi.org/DOI:10.31579/2690-4861/235
1 Consultant, Department of Nephrology, Dispur Hospitals,
2 Medical officer, Department of Nephrology, Dispur Hospitals
3 Junior Resident, Department of Radiology, Dispur Hospitals
*Corresponding Author: Tauhidul Alam Choudhury, House no-16, Raj Path, Hatigaon, Guwahati, India.
Citation: Tauhidul A. Choudhury. Abhishek Debnath A. , Sudhir R. Prasad, Neha Singh (2022). A Rare Anatomic Variant of The Superficial Palmar Branch of The Radial Artery Used for Arteriovenous Fistula Creation. International Journal of Clinical Case Reports and Reviews. 11(4); DOI:10.31579/2690-4861/235
Copyright: © 2022 Tauhidul Alam Choudhury, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 June 2022 | Accepted: 25 June 2022 | Published: 12 July 2022
Keywords: case report; anatomic variant; superficial palmar branch; radial artery; arteriovenous fistula
Anatomical knowledge regarding the variant branching patterns of the radial artery is considerably crucial for interventionalists, vascular, and plastic surgeons. We report a case of a rare variant branching pattern where the superficial palmar branch of the radial artery originated from the radial artery in the forearm instead of the wrist with a subcutaneous course in a 52-year-old patient with diabetic end-stage kidney disease who required haemodialysis initiation. This variant branch was used as inflow for the creation of the arteriovenous fistula for haemodialysis access.
The vascular access of choice for patients receiving haemodialysis is the radiocephalic fistula where radial artery is used as inflow. The radial and ulnar arteries form a superficial and deep palmar arch that provides arterial blood supply to the hand. Many clinically significant anatomical variations of the radial artery in its origin, branching, and course have been reported.
The radial artery arises from the bifurcation of the brachial artery in the antecubital fossa. The artery distally runs on the radial and anterior parts of the forearm. The artery winds laterally around the wrist after giving a superficial palmar branch and enters the anatomical snuff box before reaching the proximal end of the first interosseous space to form the deep palmar arch [1].
The superficial palmar branch of the radial artery (SPBRA), after passing the carpus, pierces through the thenar muscles to unite with the ulnar artery to form the superficial palmar arch [2]. Many variations in the origin, branching, and course of SPBRA have been reported [3]. However, the proximal origin of SPBRA at the forearm is rarely reported. To the best of our knowledge, thus far, no case report on the creation of the arteriovenous fistula (AVF) by using SPBRA as inflow is available.
Herein we report a case of the anatomic variant of SPBRA where it arose from the radial artery in the forearm and was used for the construction of the AVF in a patient with diabetic end-stage kidney disease.
A 52-year-old man who was recently diagnosed as having end-stage kidney disease due to diabetes was evaluated for AVF creation for vascular access. He required immediate initiation of dialysis due to the presence of uremic symptoms.
On the visual inspection (Day 0) of the hand (left), pulsation over the skin just proximal to the wrist was observed. On palpation, the pulse was felt over a 4–5-cm length, and the pulse rate was 78/min. We believed it to be a radial artery pulse. The result of the preoperative Allen test was negative.
After making a skin incision, we identified a superficial artery. Although we initially considered it to be a vein, pulse and flow pattern confirmed the presence of an artery. Furthermore, after dissecting medially, the radial artery was identified (Figure 1). The radial artery was deep and on the radial side of the forearm with normal course. The distance between them was approximately 1.0–1.5 cm at the level of anastomosis. The diameter of both the arteries was the same. The result of the intraoperative Allen test was negative for both the arteries.

The superficial branch was traced proximally and distally. An AVF was successfully created with the superficial artery as inflow and cephalic vein as outflow (Figure 1). Doppler ultrasonography of the fistula on day 1 demonstrated the proximal origin of SPBRA with a superficial course with the presence of iatrogenic AVF with a cephalic vein showing normal patency and flow. The deep branch was normal in its course and pattern (Figure 2). Haemodialysis was initiated on day 1 via a temporary venous catheter and then performed twice in a week.

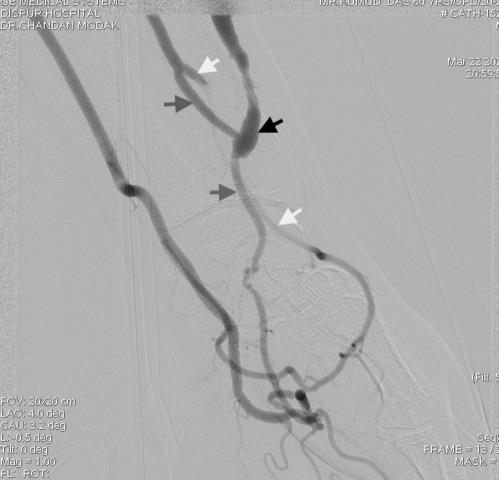
Selective angiography using minimum volume of contrast (16 ml) was performed on Day 5 to demonstrate the aberrant variations of distal radial artery and palmar arch.
The angiography revealed the proximal origin of SPBRA with a superficial course and functioning AVF with SPBRA as inflow (Figure 3). SPBRA originated from the radial artery 8 cm proximal to the wrist. SPBRA contributed to form the superficial palmar arch with the ulnar artery. Deep palmar arch was normal in course and pattern. Poor opacification of the radial artery was observed beyond the take-off of the superficial palmar branch, presumably related to altered haemodynamics related to the fistula. There was no evidence of stenosis, thrombosis and arterial dissection. The course of SPBRA and its relationship with the radial artery are shown in Figure 3.
Variations in the origin, branching pattern, and course of radial arteries are not uncommon. Appropriate detection of these variations is crucial in several clinical procedures in different fields (e.g., radial artery catheterisation for percutaneous coronary interventions, various endovascular procedures, AVF construction for vascular access, and radial artery harvesting).
High origin of the radial artery from the brachial artery is one of its frequent anatomical variations, and its prevalence was 14.26% in cadaveric studies and 9.75% in angiographic studies [5]. Low origin of the radial artery is a rare anatomical variation, with the incidence estimated at 0.2%.
Aberrant variations observed in distal radial arteries are the division of the radial artery into palmar and dorsal branches in the forearm and the anomalous course of the radial artery in the region of the anatomical snuff box. In a cadaver study [4], division of the radial artery into palmar and dorsal branches at the distal half of the forearm was observed in 10% of specimens, and the palmar branch bifurcated into a superficial and deep branch. In this study, 2% specimens showed the origin of SPBRA 12.2 cm proximal to the radial styloid process, which superficially continued to the flexor retinaculum and thenar muscles to form a part of an incomplete superficial palmar arch.
The superficial radial artery is another variant in which the radial artery passes superficially to the tendons of the anatomical snuffbox. In human cadaver studies [6,7], the incidence of this variation ranged from 0.5% to 1%.
Tagil et al [2] described one variant course of SPBRA that ran superficially to and in contact with the flexor retinaculum and ran transversely to join the ulnar artery without reaching the thenar muscles. Another variation of SPBRA was reported by Singer et al [8] where it ran a superficial course over thenar muscles, causing pain. In this case report, he described the absence of superficial palmar arch and large calibre SPBRA.
To date, the proximal origin of the superficial palmar branch of the radial artery at the forearm is rarely reported.
In our patient, SPBRA originated in the forearm and ran a superficial course, which was incidentally detected during AVF construction. SPBRA originated 8 cm proximal to the wrist and contributed to form a superficial palmar arch by the ulnar artery (Figure 3). Herein the early bifurcation of the radial artery into SPBRA and deep branch was observed at the forearm. The deep branch ran the usual course as that of the radial artery.
The superficial arteries often pose iatrogenic complications because they are often mistaken for veins during intravenous injections [7,9]. This may lead to complications such as hematoma, thrombosis, arterial injury, and digital ischemia. These complications, along with the variant branching of the radial artery, may cause difficulty and unsuccessful catheterisation of the artery by interventionalists or vascular surgeons. The variations may also result in hand ischemia if overlooked during harvest. Appropriate detection of superficial arteries is crucial for plastic surgeons particularly during the elevation of forearm flaps [10].
In a previous case report, the superficial radial artery was used as inflow for the construction of AVF for vascular access [11]. This is the first case to use the anatomic variant SPBRA as inflow to create the AVF.
Identification of and knowledge regarding superficial arteries in the wrist are crucial for surgeons because it may be mistaken as a vein. After dissecting the cephalic vein, we found the superficial palmar branch of the radial artery that arose early from the radial artery in the forearm. The AVF was successfully created with inflow from the SPBRA and cephalic vein as outflow in the distal forearm.
Proximal origin of the superficial palmar branch of the radial artery at the forearm is a rare anatomical variant branch of the radial artery. Knowledge regarding the anatomic variant of the radial artery is crucial for interventionalists or vascular surgeons to prevent inadvertent complications.
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
The study was carried out in accordance with the Declaration of Helsinki and approved by the Institutional Ethical Committee.
The author(s) received no financial support for the research, authorship and/or publication of this article.
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
