
Review ariticle | DOI: https://doi.org/10.31579/2690-4861/592
1University professor, specialist in phlebology and lymphology, and Chief of the vascular surgery and phlebology service at Clínica Romagosa, Córdoba Argentina.
2A Specialist in Gynecology and President of the World Society of Cosmetic Gynecology Dallas, Texas, USA.
3Scientific Coordinator of ICAM USA, Dallas, Texas USA.
*Corresponding Author: Gustavo H Leibaschoff, A Specialist in Gynecology and President of the World Society of Cosmetic Gynecology Dallas, Texas, USA.
Citation: Romero Díaz EJ, Gustavo H. Leibaschoff, Juliana Melamed. (2024), A Prospective Clinical Trial to find the Efficiency of the Therapeutic use of a Combination of Transdermal gels Producing CO2 in Treating Varicose Ulcers that do not Respond to Primary Treatment, International Journal of Clinical Case Reports and Reviews, 20(3); DOI:10.31579/2690-4861/592
Copyright: © 2024, Gustavo H Leibaschoff. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 November 2024 | Accepted: 18 November 2024 | Published: 06 December 2024
Keywords: varicose ulcers; transdermal carboxytherapy
In this study, we evaluated 40 patients, all carriers of severe varicose ulcers. After four weeks of undergoing the same primary treatment, the progress was not as expected. We added two weekly applications, eight sessions in total, of transdermal carboxytherapy CO2-producing gels to their treatment primary regimen.
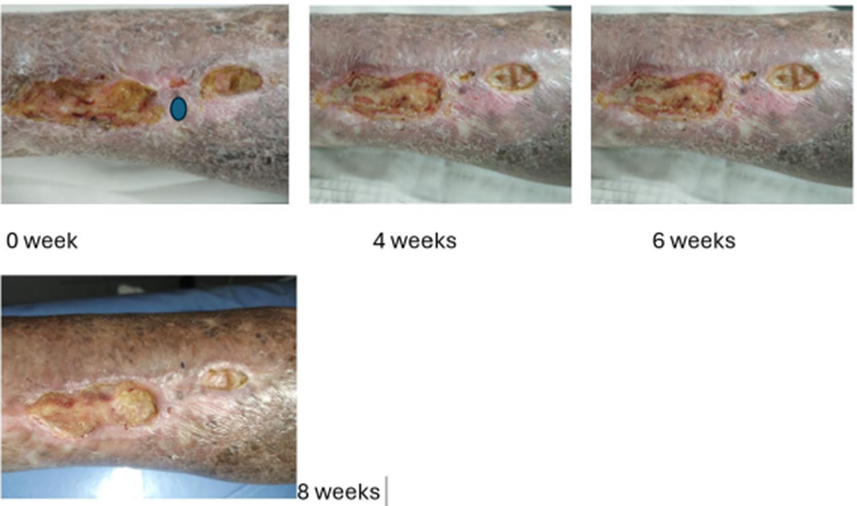
We assessed the patients through photos taken before applying the gels and after 4 and 6 weeks of the starting date.
We evaluated clinical manifestations, including the varicose ulcer's diameter and length, granulation, exudates, and pain.
The patients underwent an arterial and venous Echo Doppler before and immediately after the first application to rule out arterial involvement and to observe any changes in stroke flow at the microcirculatory level.
We measured the transcutaneous oxygen pressure (TcPO2) at a specific point for reference using a sensor before and after the first application and after the eighth application (one month later) of the gels (CO2PRO®) to see if transdermal carboxytherapy increased tissue oxygenation.
Purpose
This prospective study aims to evaluate the efficacy of a transdermal product (CO2PRO®) that, through a combination of gels, provides carbon dioxide to increase microcirculation and promote tissue oxygenation through the Bohr effect, helping to regenerate varicose ulcers.
Patients selected to enter the study were under primary ulcer treatment and were not responding as expected. The patients continued to use their primary treatment and added the combination of gels that produce transdermal CO2
Chronic venous insufficiency (CVI) frequently affects the lower limbs, secondary to valvular incompetence, venous obstruction, or post-thrombotic phenomenon.
While CVI is not a life-threatening disease, it can result in long-standing morbidity with consequent financial and social consequences. 2,3
CVI-associated microcirculatory dysfunction is secondary to a chronic, sustained inflammatory injury resulting in end-organ damage to the skin and dermis.4
In CVI, the microcirculation is diminished, resulting in skin changes and ulcer formation.
Evaluating transcutaneous partial oxygen pressure (TcPO2) can predict tissue oxygenation. 2,3 Patients with severe CVI have hyperpigmentation, lipodermatosclerosis, and eventual venous ulcer formation.
These signs of the disease are all associated with irregular fibroblast activity, excessive scar tissue formation, and the development of excessive matrix contraction.5
Compared with normal fibroblasts, venous ulcer fibroblasts have demonstrated an inability to produce collagen after stimulation with TGFb1.
This unresponsiveness is related to a decrease in TGF-b1 type II receptors.5
Factors delaying tissue oxygenation influence ulcer formation and maintenance in patients with CVI. CVI, Chronic Venous Insufficiency, is a condition affecting the veins in the lower limbs. At first, CVI causes few, if any, symptoms and can be hard to spot. However, as it continues, it can lead to symptoms and signs like pain, swelling, skin damage, and ulcers.
Satisfactory tissue perfusion and oxygenation are requirements for wound healing.
When the valves in the leg veins are affected or the veins are dilated, retrograde blood flow causes venous hypertension.
Microcirculatory venous hypertension results in the extravasation of macromolecules and red blood cells and excessive iron deposition into the dermal interstitial.
Red blood cell degradation products, iron from hemoglobin, and interstitial protein extravasation are potent inflammatory agents that create a chronic inflammatory signal.
Mechanical disturbance of the endothelial cells results in the margination and activation of white cells, which leads to insistent inflammation and oxidative stress, along with the appearance of multiple cytokines and chemokines.6
Overexpression of matrix metalloproteinases changes collagen turnover and destroys the dermal tissues and subsequent ulcer formation.7
Pericapillary fibrin restrains growth factors and diminishes oxygen diffusion, contributing to local tissue hypoxia.
The result is an open, draining wound with excessive exudate and surrounding sclerosis. The injury induces leukocyte recruitment, destruction of the extracellular matrix (ECM) dermal architecture, and venous ulcer formation.
Numerous other cytokines have been implicated in developing and healing venous ulcers.8 Studies demonstrated that ulcers have higher levels of the proinflammatory cytokines interleukin 1a (IL-1a), IL-1b, interferon g (IFN-g), IL-12p40, and granulocyte-macrophage colony-stimulating factors. 9
In summary, venous hypertension at the microcirculatory level causes abnormal fibroblast function. Fibroblast replication is broken, resulting in poor wound healing and dermal fibrosis.
Diminished replication is secondary to the development of senescence and an inability to respond to growth factors. 10 Venous hypertension causes fibroblasts to develop a myofibroblast phenotype.
Myofibroblasts raise skin tension, possibly conducting skin separation in response to an injury stimulus. Finally, leukocytes that travel to the injury site play a significant role in wound healing.
Sindrilaru et al.'s investigation demonstrated that iron overload in the dermis of CVI patients causes leukocytes to maintain an inflammatory rather than a wound-healing phenotype. 11
The CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification is an internationally accepted specification for describing patients with chronic venous disorders. 1 “The CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification is an internationally accepted standard for describing patients with chronic venous disorders. It has been used to report clinical research findings in scientific journals. Developed in 1993, updated in 1996, and revised in 2004, CEAP is a classification system based on clinical manifestations of chronic venous disorders, current understanding of the etiology, the involved anatomy, and the underlying venous pathology.”
| Stage | Symptoms |
| C0 | no visiblesigns |
| C1 | visible veins or blood vessels |
| C2 | varicose veins (protruding veins) |
| C3 | edema (swelling) |
| C4 | changes to skin quality |
| C5 | healed ulcers |
| C6 | open ulcers |
Ulcers
An ulcer is a cutaneous wound that breaks the structural and functional integrity of the skin. The target is a patient with a wound, not only the wound itself. The chronic wounds occurring in CVI patients are a growing problem, mixed arterial-venous ulcers included. They are up to 90% of all lower leg ulcers. Venous ulcers, active or healed, are present in 1% of the United States population.12 Establishing the duration for a wound to be considered chronic has been debated, with time courses ranging from weeks to months. When the four typical phases of wound healing (hemostasis, inflammation, proliferation, and remodeling) fail to follow this orderly progression of events to complete treatment, the wound cut out (frequently in the inflammatory phase). Ulcers, particularly those on the lower extremities, are chronic when they fail to heal within 4 to 6 weeks and show no tendency to do so.13
Other considerations when diagnosing a chronic wound: If the wound surface area is reduced by 50% during four weeks of standard care, it will likely heal with the same treatment in 12 weeks. If less than a 50% reduction occurs, it is unlikely to recover on this treatment, and a reassessment and difference in therapy should be considered. 14-15 Even with the best care available, 25 to 40% of leg ulcers are not fully healed after six months of treatment. Venous disease, VCI, causes 70% of leg ulcers; 20% are generally caused by arterial insufficiency or mixed arteriovenous disease, and 10% by other conditions.
Risk factors for venous leg ulcers include advanced age, female sex, a family history of venous leg ulcers, white race, deep-vein thrombosis or phlebitis, previous leg injury, chronic leg edema, a sedentary lifestyle, and prolonged standing. Bacterial infection and continuing venous hypertension influence poor wound healing in the presence of improved matrix contraction.
Hypertension influences ulcer wound healing through a mechanism known as mechanotransduction. Mechanotransduction involves adapting physical forces into biochemical signals and integrating these signals into a cellular response. Dermal fibroblasts activate transcellular receptors, stimulating intracellular signaling pathways that inhibit TGF-β1-mediated matrix contraction. Matrix contraction is fundamental for wound closure. Inhibition of this process results in prolonged wound healing. In addition, bacterial biofilm and toxic cytokines in the ulcer base and surrounding tissue inhibit ulcer wound healing. 16
Chronic wounds have an altered metabolism and modified cell reactions. Examples of these are, e.g., an increased amount of matrix
metalloproteinases (MMP) found in the locality of the wound, which is responsible for the intensified hydrolyzation of cytokines and growth factors capable of promoting wound healing, e.g., an intensified degradation of the extracellular matrix, e.g., inhibition of cell proliferation in wounds in which the exudate contains an augmented amount of inflammatory cytokines, and where increased amounts of the above-mentioned reactive oxygen species (ROS) are present. 17-18-19-20-21-22 23
Hypoxia is found in chronic wounds, which leads to tissue necrosis. 21 As a result of hypoxia, the cells at the base of the wound lack metabolic energy, particularly oxygen and, subsequently, adenosine triphosphate (ATP), essential substrates for tissue regeneration. However, the cells can regenerate and immediately begin regenerating with an acceptable oxygen supply. 24 Chronic wounds treated with oxygen or techniques that increase oxygenation heal faster and more effectively, opening new possibilities in wound care.
Oxygen acts as a substrate for cellular ATP synthesis and can also form reactive molecules (reactive oxygen species, ROS) such as peroxide, superoxide anions, and hydroxyl radicals; those are the Spartan signaling substances for the inflammatory reaction in wound healing. 25
Oxygen has a strong antibiotic effect on wounds. For adequate collagen synthesis, hydroxylases require an oxygen partial pressure of approximately 70 mm Hg. The local hypoxia of a chronic wound needs to be corrected, either by increasing blood oxygen levels or using external sources. Wound healing depends on a sufficient oxygen supply for mitochondria.
Evaluating available oxygen is crucial for determining the wound's clinical status. Hypoxia can be characterized using transcutaneous oxygen partial pressure, TcPO2.TcPO2 directly measures the tissue oxygen partial pressure and is the ultimate parameter for the diffusive provision of oxygen to the tissue cells, including the mitochondria. Also, transcutaneous oxygen (TcPO2) measurement near the wound helps assess skin perfusion pressure changes.24
Ogri et al. also measured peri-ulcer TcPO2 at 44°C in 13 chronic wounds. They noticed low values that were exceedingly significant compared to measurements in non-ulcerated lower legs. The study used Transcutaneous oximetry (TcPO2) to identify viable tissue with the best healing potential. TcPO2 can also assess chronic limb ischemia and the likelihood of ulcer healing. In advanced CVI, TcPO2 can serve as a marker of oxygenation status. The normal range for TcPO2, transcutaneous partial pressure of oxygen, is greater than 55 mmHg. 26 A value of 40 mmHg is considered critical; wound healing is reduced below that, and ischemia develops. The classification of hypoxia in all chronic wounds varied from 0 to 40 mmHg. This shows that chronic wounds are heterogeneous regarding oxygenation, both within the wound itself and between different wounds.27
Carboxytherapy
Carboxytherapy is the therapeutic use of carbon dioxide (CO2) in its gaseous state through subcutaneous injection or transdermal application using CO2-producing gels. Upon subcutaneous injection, CO2 swiftly diffuses at the cutaneous and muscular microcirculatory levels, triggering an immediate increase in microcirculatory vasodilation and a rapid improvement in blood flow through a direct action on arteriole smooth muscle cells. CO2 promotes Bohr’s effect, a crucial physiological process in the body's oxygen transport system. The Bohr effect refers to a decrease in hemoglobin's affinity to oxygen due to increased CO2, which means that extra oxygen is available to other tissues. The Bohr effect also increases the tissue pO2 at the application site. The Bohr effect explains that increased carbon dioxide in the blood within peripheral tissues leads to a right shift in the oxygen-hemoglobin dissociation curve, increasing tissue oxygenation.
98% of Oxygen is carried throughout the bloodstream and bound to a protein molecule, hemoglobin, in red blood cells. A small portion, 2%, of Oxygen in the bloodstream is dissolved directly in the plasma.
The Physiotherapeutic action of CO2:
• Increased flexibility and decreased hardness of collagen fibers at pH ≤6.5
• Reduction of divalent calcium ions
• Decreased tonus of arteries and capillaries leading to vasodilatation 28
• Increased blood flow to the injected site 29
• Improved tissue drainage due to increased tissue perfusion and lymph circulation 30
• Release of local growth factors resulting in angiogenesis, lipolysis, and skin regeneration 31-32 • Dissociation of carbonic acid to H+ and HCO3 and subsequent formation of Ca (HCO3) 2, NaHCO3, and KHCO3
The oxy-hemoglobin dissociation curve is vital for comprehending how blood transports and releases oxygen.33
At the cellular level, Carbon dioxide is produced in cells primarily through the citric acid cycle, which occurs in the cytoplasm and mitochondria. Like other molecules, carbon dioxide travels from areas where it's produced, such as the mitochondria and cytosol, through the phospholipid cell membrane and into the extracellular space. Carbon dioxide diffuses more quickly than oxygen. As cells generate carbon dioxide, it dissolves in the cytoplasm's water and accumulates until its partial pressure exceeds 40 to 45 mmHg. This accumulation creates a concentration gradient that allows carbon dioxide to diffuse.
Carbon dioxide then moves from the extracellular space into the capillaries, where it quickly equalizes, increasing the carbon dioxide partial pressure in the blood from roughly 40 mmHg on the arterial side of the capillary to between 45 and 48 mmHg on the venous side. 34
Once the venous blood returns to the lungs, carbon dioxide diffuses out of the bloodstream, through the capillaries, and into the alveoli, where it is expelled. Oxygen binds with hemoglobin and is carried back to the tissues during this process. As tissues produce carbon dioxide, the reaction is consistently pushed forward at the peripheral sites, following Le Chatelier's principle. Another key player in this process is hemoglobin, which acts as a buffer for the protons created by this reaction. Simultaneously, the bicarbonate ions move out of the red blood cells into the plasma and the serum through a special HCO3-/Cl transporter in exchange for a chloride anion. 34. 35
As blood returns to the lungs and the partial pressure of oxygen increases, the carbon dioxide dissociation curve shifts to the right (indicated by the arrow showing the offloading of carbon dioxide as oxygenation increases). This shift decreases the total carbon dioxide content in the bloodstream. During exhalation, carbon dioxide diffuses from red blood cells through capillary walls and into the alveolar spaces. Even though the partial pressure of carbon dioxide decreases from 45 or 46 mmHg on the venous side to 40 mmHg on the arterial side, the total amount of carbon dioxide in the bloodstream decreases by a much more significant percentage.36
Oxygen delivery and carbon dioxide removal are closely connected through processes described by the Bohr and Haldane effects. The Bohr effect explains that increased carbon dioxide in the blood within peripheral tissues leads to a right shift in the oxygen-hemoglobin dissociation curve, increasing tissue oxygenation. As the influx of oxygen increases hemoglobin saturation, carbon dioxide is more likely to detach and diffuse into the alveoli for exhalation, known as the Haldane effect. 37 Clinically, transportation and elimination of carbon dioxide become especially crucial in regulating the pH of the blood. The body's pH will decrease if the partial pressure of CO2 increases or decreases.38-39 In response to increased tissue CO2 and reduced pH, the oxygen hemoglobin dissociation curve shifts rightward, favoring the release of oxygen (O2) from the blood into local tissue.
Transdermal Carboxytherapy
Carboxytherapy can also be administered transdermal through a new treatment option: a topical gel (CO2Pro®, Lumisque, Inc.; Weston, FL). The kit contains two packs of gels (gel one magnesium carbonate and gel two gluconolactone). When mixed, they are activated, and the product releases CO2. The gel is then topically applied and absorbed into the skin through the superficial layers, transdermal, producing its therapeutic benefits through increased microcirculation and Bohr’s effect action in the areas where it is applied.


Several prior studies have examined the benefits of transdermal CO2 and found that transdermal CO2 produces effects comparable to those of injectable CO2. Sakai et al. reported that transcutaneous CO2 was beneficial for therapeutic purposes via increased blood flow and microcirculation, as evaluated by laser Doppler, providing evidence of the Bohr effect in vivo.40 Leibaschoff and co-workers used video capillaroscopy to assess the impact of a CO2 transdermal gel and found improved microcirculation comparable to that observed after subcutaneous CO2 injection.41 The study from Amano-Iga demonstrated that CO2 combination gels accelerated wound healing by upregulating VEGF and TGF-β and downregulating HIF-1α, IL-1β, and IL-6 in a rat skin defect model. The application of CO2 combination gels accelerated routine wound healing by improving hypoxia and angiogenesis and reducing the expression of inflammatory cytokines. 42
Study treatment
We conducted the prospective clinical study after the approval of the institutional research and ethical committee. The study was conducted at Clínica Romagosa and Centro Cecyo, Córdoba City, Cordoba, Argentina.
All patients invited to participate in the study signed the corresponding consent to add the combination of gels that produce CO2 to their primary treatment. They also agreed to follow the instructions to apply the gel at home after the first application in the clinic and to attend to the controls.
The 40 patients selected for the study were all carriers of severe varicose ulcers.
They were all undergoing the same primary ulcer treatment but were not responding as expected. After four weeks of primary treatment, they experienced delayed wound healing.
We supplemented the patients' existing treatment with transdermal CO2-producing gels. They continued their primary treatment while adding a combination of gels that generated transdermal CO2.
During the study, 40 patients used the gel-producing transdermal CO2 (CO2PRO®) twice a week for four weeks while continuing their primary
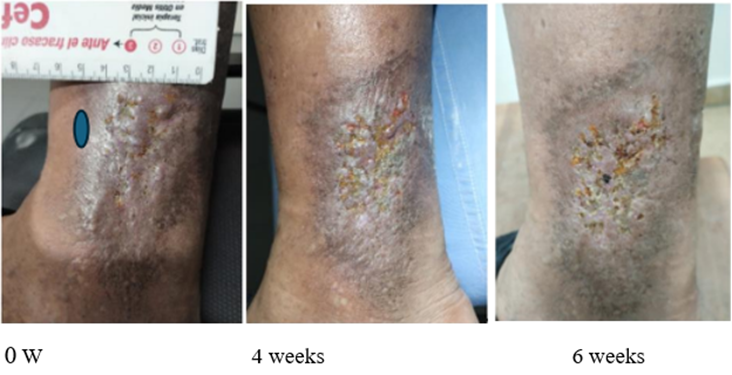
treatment. The first application was made at the study premises, while the rest were made at home. In all cases, patients cleaned their varicose ulcers with sterile saline solution (in disposable ampoules provided) and kept their ulcers covered with sterile dressings that changed twice a day. We assessed the patients through pictures taken before applying the gel and after 4 and 6 weeks of the starting date.
The patients underwent an arterial and venous Echo Doppler before and after the first application to rule out arterial involvement and to observe any changes in stroke flow at the microcirculatory level. We evaluated
clinical manifestations, including the varicose ulcer's diameter and length, granulation, exudates, and pain. Wound ulcers were analyzed before the first application and after weeks 4 and 6, when we assessed the healing based on the size of the wound in centimeters, considering the measurements of length and width, exudates (the presence or lack of exudates), granulation tissue, and wound tissue based on the score of the wound (ulcer) bed scoring.
The wound (ulcer) bed scored 0. Closed/resurfaced. The wound is covered with epithelium (new skin)
1 Epithelial tissue. For superficial ulcers, new pink or shiny tissue skin that spreads in from the edges or islands on the ulcer surface
2 Granulation tissue Pink or beefy red tissue with a shiny, moist, granular appearance.
3 Slough Yellow or white tissue that holds to the ulcer bed in strings or thick clumps or is mucinous
4 Necrotic Tissue (eschar) Black, brown, or tan tissue that adheres firmly to the wound bed or ulcer edges and may be firmer or softer than the contiguous skin. 43
We evaluated the transcutaneous oxygen pressure (TcPO2) through transcutaneous oximetry, a simple, reliable, noninvasive technique for objectively evaluating wound perfusion and oxygenation.
Patients were in supine positions. The TcPO2 value was measured on peri ulcer skin 1 cm proximal to the upper margin of the ulcer. TcPO2 was measured through a sensor before and after the first application and after the last 8th application (one month) to observe whether transdermal carboxytherapy increases tissue oxygenation.
TcPO2 was measured by an electrochemical transducer, fixed to the skin with an adhesive ring and contact liquid supplied by the manufacturer. The measuring site was cleaned carefully by a disinfectant (chlorhexidine). To improve the skin's permeability to oxygen molecules at the determining site, the transducer is heated to 44°C. A normal TcPO2 is considered around 60 mmHg, regardless of the electrode location. The higher the peri-wound TcPO2 levels, the higher the chances of wound healing. A confirmed correlation was found between TcPO2 values and various pointers of wound healing, such as a decrease in wound size, a reduction in the amount of exudate, and an improvement in wound score 44. The oxygen diffuses according to its pressure gradient from the capillary loops through the avascular epidermis towards the skin surface electrode. (dot blue in the photos before)
Patient 1:
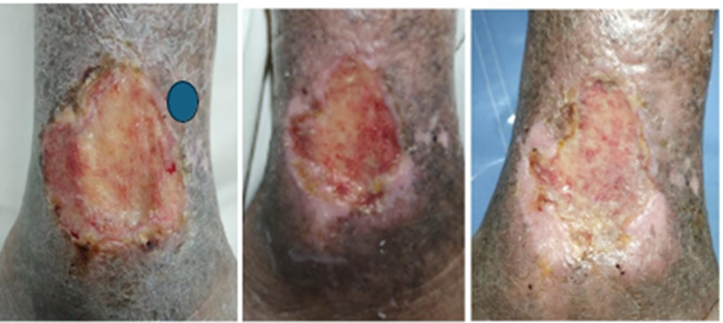
0 week 4 weeks 6 weeks
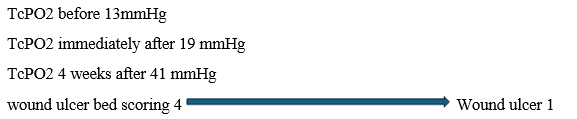
TcPO2 before 14 mmHg
TcPO2 immediately after 19 mmHg
TcPO2 4 weeks after 36 mmHg
wound ulcer bed scoring3 Wound ulcer 2
The patient with good adherence to the treatment – understands and follows the treatment as planned, with two weeklyapplications of 45 minutes of permanence – Significant improvement is observed in the ulcer bed with a reductionof exudate, the superficial nation of the same – the appearance of coarse tissue,reduction of the height and width of the same –
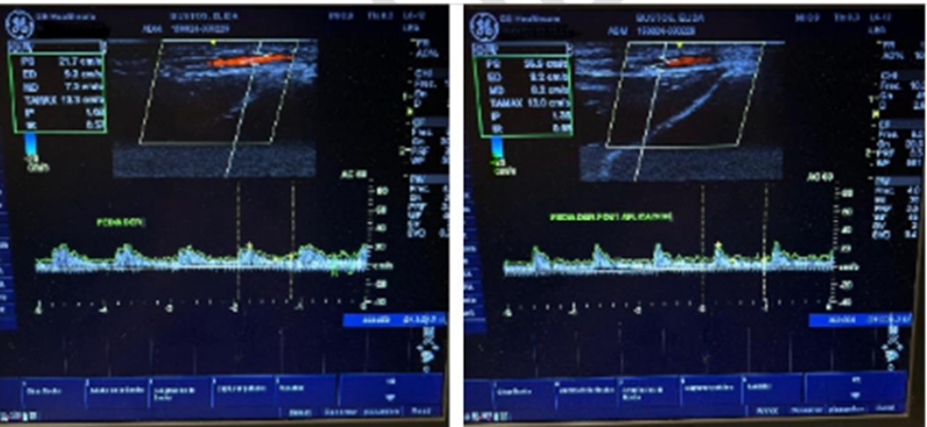
onthe other hand, the patientmanifests clear improvement in the appearance of nutrition, turgor, and elasticity of the ulcer in the skin around the ulcer. It should be noted that studies were carried out with high-resolution Doppler echo and general equipment electric versant balance, in which an increase in peak arterial flow was observed in images.
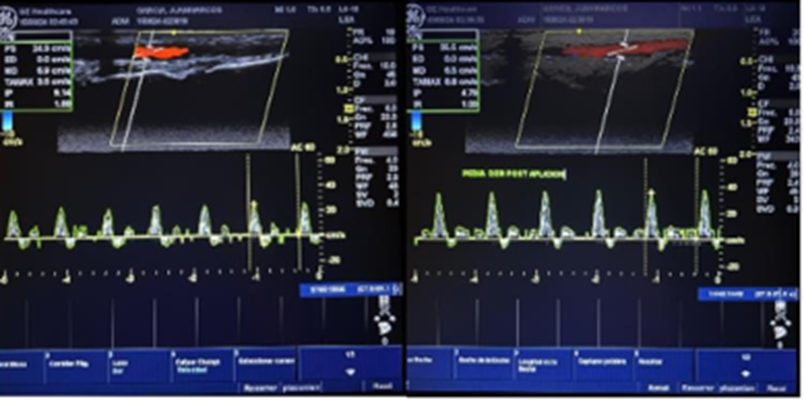
Peak systolic flow increases artery pedia by 3% immediately after the first application of the CO2 transdermal gel. “Peak systolic velocity (PSV) is an index measured in spectral Doppler ultrasound. On a Doppler waveform, the peak systolic velocity corresponds to each tall “peak” in the spectrum window.”
“Low velocity may vary based on vessel properties and pathological changes. Low resistance vessels (e.g., internal carotid artery, renal artery)
supply end organs requiring perfusion throughout the cardiac cycle. These vessels exhibit high diastolic flow and EDV 4. In contrast, high resistance vessels (e.g., external carotid artery, limb arteries) are characterized by early reversal of diastolic flow and low or absent EDV(end-diastolic velocity)” 45
Male 51 years old, obesity BMI 29, Diabetic
Ulcer 6cm length and 2 cm width clean
Pain
Positive arterial pulses
Rx metformin Diosmin pantoprazole
Local use of Collagenase cream
Patient 3:

Vascular Doppler Echo: No changes in pre-and post-velocity after the first session of CO2 gel
Female 81 years old, recurrent ulcer, overweight BMI 28, osteoarthritis (uses a cane to walk)
Rx medication losartan, rosuvastatin Diosmin.
ulcer four long, 2 cm wide, deep, clean bottom
CEAP 6
Arterial peripheral pulse present
Saphenous vein insufficiency of the right leg
Patient 4

Patients with good adherence to treatment – however, keep in mind that they are ulcers with a long history of evolution – relapsed – resistant to treatment – in overweight patients – osteoarthritis with difficulty in mobilization and stimulating to acquire postural measures that help drain the lower limb
However, the appearance of the ulcer bed and its edges have been improving, with improvement in the ulcer bed with granulation tissue and a gradual decrease in its diameter.
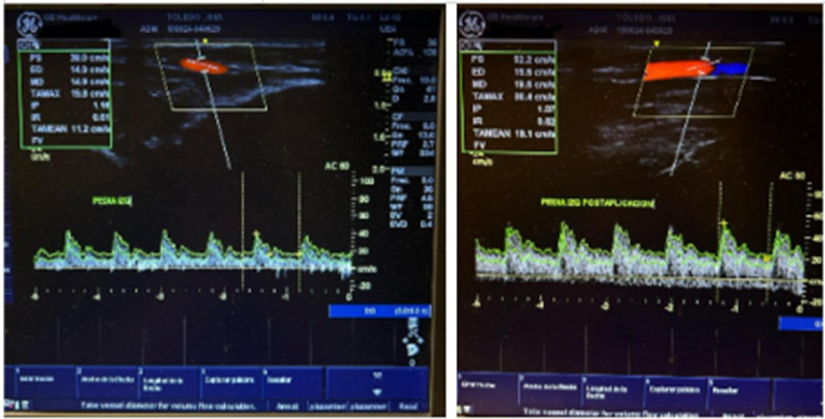
Female 76, overweight, BMI 26, hypothyroidism, arterial hypertension, ulcer 5 cm long by 1.5 cm wide, bed with fibrin, surrounded by ochre dermatitis and stiff skin. Oral medication such as Diosmin, local collagenase cream, and elastocompression are indicated. The Doppler echo report shows positive arterial pulses and a 3% increase in the systolic peak immediately after applying the gel with CO2 transdermal.
CEAP 6
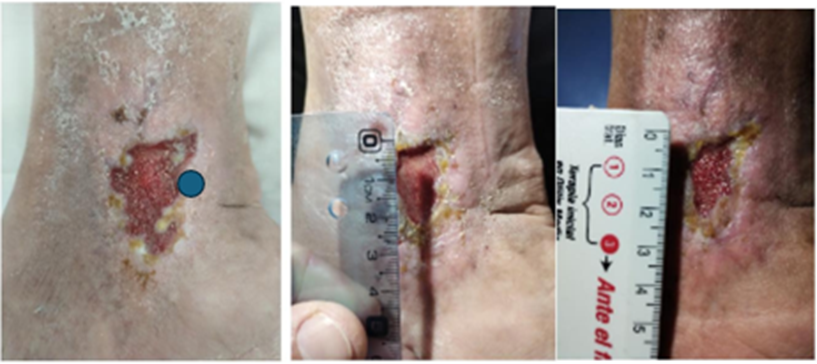
Patient 5

TcPO2 before 17mmHg
TcPO2 immediately after 21 mmHg
TcPO2 4 weeks after 38mmHg
wound ulcer bed scoring 3  Wound ulcer 1
Wound ulcer 1
This young patient - 27 years old - with a history of DVT and lupus - postphlebitic syndrome - with recurrent ulceration and complex resolution initially started once a week - she showed burning when she
applied the product - however- she saw a significant improvement; she asked to increase the dose and started with twice a week - extremely positive result - patient very adherent to the treatment.
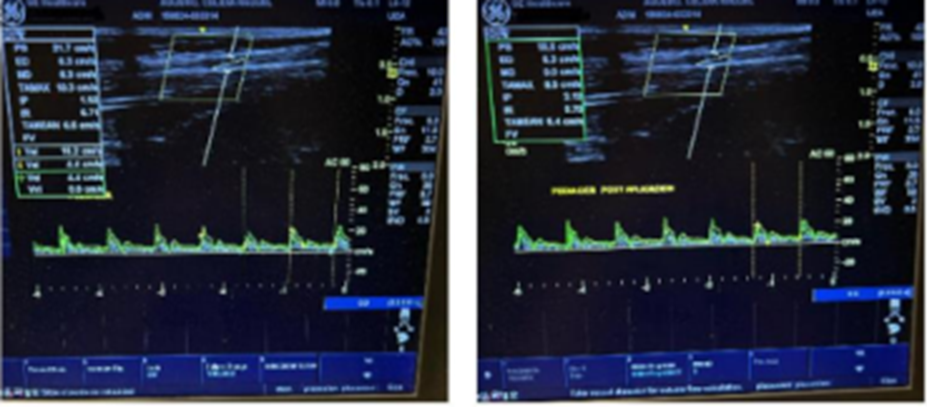
Doppler ultrasound shows the insufficiency of the postphlebitic left popliteal vein in the venous system and increased 3% arterial flow after the first application of CO2 gel.
Female 27 years old
History of previous ulcers, systemic lupus
DVT history
ulcer 3 cm long, 2 cm wide, semi-deep with granulosis bed pain in the varicose ulcer ochre dermatitis
Rx Ketorolac, collagenase cream, and elastocompression are indicated
CEAP 6
Patient 6

He is a patient who lives alone – he came into a deplorable state of hygiene – muscular scoliosis – the treatment and the ways of healing were explained in detail – the first four weeks, the improvement of both the ulcer and the skin was surprising.
76 Male
Recurrent Ulcer
Antecedent of DVT
Osteoarthritis
Ulcer Length 4 Width 4 Surface
Fibrin bed, serous oozing, edema, desquamative dermatitis
CEAP 6
Rx Diosmin collagenase elastocompression cream
Venous vascular Doppler ultrasound, popliteal vein insufficiency, left the internal saphenous, positive arterial system, and increased systolic peak (1.3%) after the first application of CO2 gel.
Patient 7
Venous ulcers are the most common type of chronic lower extremity ulcers, affecting 1% to 3% of the U.S. population.
Our study assessed 40 patients with severe varicose ulcers undergoing the same treatment, including elastocompression therapy, sterile wound dressings, and local therapies like collagenase creams.
They were also taking Diosmin. However, after four weeks, the treatment progress was not as expected, and the results were either unsatisfactory or very slow. Therefore, we decided to add Transdermal CO2 gel to their current treatment.
Patients presented ulcers from chronic venous insufficiency CVI and post phlebitis syndromes. Concomitant diseases such as osteoarthritis and overweight were found, which gave rise to difficulty in mobility.
Difficulty wounds need a multidisciplinary, insistent, and mixed approach.
Transdermal carboxytherapy was added to the primary treatment through a topical gel (CO2PRO®, Lumisque, Inc.; Weston, FL). The Application of the CO2 Pro gel is remarkably simple.
All patients were briefed on the application process. The patients and/or their family members quickly understood the information.
Most cases showed significant clinical improvement after 4 weeks of treatment (8 applications).
This included enhanced skin quality, recovering the condition of the surrounding skin, diminishing exudate, and improving granulation. In some cases, the ulcer closes within the 4-week treatment period. (Photos before and after)
In all cases, a Venous and Arterial echo Doppler were performed before and after the first application. The Venous Doppler showed different gradations or manifestations of chronic venous insufficiency, such as edema, reflux, and chronic DVT.
The Arterial Doppler done after the immediate application of the gel showed an increase in the peak stroke flow. The rise in blood flow consequently increased the oxygenation of the compromised tissue perfusion.
Peri-wound TcPO2 showed increased oxygenation immediately after the first session of CO2 transdermal and one month of treatment.
TcPO2 values may be used to expect a response to the whole treatment and have a positive link concerning wound healing.
We should note that the study focuses on patients with advanced chronic venous insufficiency (CVI) and ulcers at a public hospital in Argentina.
Throughout the survey, 30% (12) of the 40 initially enrolled patients withdrew from the study due to social, cultural, and economic reasons. We conducted telephone consultations with some patients we couldn't see in person but continued applying the gel at home. They reported feeling better and seeing the skin lesion recovering, although it wasn't technically proven.
The study's limitations include the lack of investigation into the long-term impact of transdermal CO2 gel on wound healing over 30 days and only eight CO2 Pro applications.
Most patients did not experience any symptoms after applying the gel. However, two patients reported a mild burning sensation during the application, which did not interfere with their ability to continue the treatment.
We observed positive therapeutic effects in the treatment of varicose ulcers as part of a comprehensive regimen that includes phlebotonic medication, elastocompression therapy, and transdermal Carboxytherapy Gel.
Notably, there were enhancements in the post-immediate arterial Doppler after the use of the combination of gels that produce CO2. There was an average increase in the systolic peak between 1.5 to 3%.
Also, the transcutaneous oxygen PO2 concentration significantly increased in all cases which helps reduce hypoxia in ulcers and surrounding zones. 45
Even though we could not photograph and monitor the progress of 30% of the initial 40 patients, we could rely on family information.
Of the remaining 28 patients, all showed improvement in their varicose ulcers due to the treatment. Some had complete closure within 4 weeks, while others displayed noticeable progress in photographs.
We conclude that adding transdermal CO2 gel to conventional treatment for patients presenting ulcers from chronic venous insufficiency CVI improves patient outcomes and can be a valuable and straightforward tool in managing chronic nonhealing ulcers.
After the good results, we suggest increasing the number of weekly sessions of the transdermal CO2 to 4 or 5, depending on the severity of the ulcer pathology.
Additionally, we advise using CO2 Pro with monthly maintenance and elastocompression therapy.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
