
Research Article | DOI: https://doi.org/10.31579/2692-9406/056
*Corresponding Author: Thomas T.H. Wan, Professor emeritus of Health Management and Informatics at the University of Central Florida, USA.
Citation: Thomas T.H. Wan, V Gurupur, Bing L Wang, S Matthews. (2021) A Patient-Centric Care Approach to Facilitate the Design of an Artificial Intelligence Application in Geriatric Care Management of Heart Failure Readmissions. Biomedical Research and Clinical Reviews. 3(5); DOI: 10.31579/2692-9406/056
Copyright: © 2021 Thomas T.H. Wan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 05 March 2021 | Accepted: 24 March 2021 | Published: 26 March 2021
Keywords: artificial intelligence research; human-factor principles; self-care management of chronic conditions; low case for geriatrics; Heart Failure; restfulness; healing environment; nutrition
The examination of human factors’ role in moderating medical interventions and hospitalizations and/or rehospitalization of heart failure (HF) patients.
Objectives: The primary purpose of this study is two-fold: 1) to show relevant human factors influencing the rehospitalization of persons with heart failure by developing a systematic algorithm generated from the cited randomized trials; and 2) to examine how the self-care principles, such as choice/efficacy, restfulness, healing environment, activity, trust, interpersonal relationships, outlook, and nutrition, may reduce heart failure readmissions.
Methods: The meta-analytic approach generated a theoretically relevant and empirically validated self-care management decision support protocol for HF. Statistical modeling of the effects of eight human factors for the reduction of HF readmissions was presented.
Findings: The systematic review and meta-analysis approach documents the results of randomized clinical trials that affect heart failure hospitalization by selected human factors. A patient-centered decision support system was developed to facilitate the self-care management of heart failure.
Discussion: Our research generates systematic knowledge about the importance of human-factor principles in the provision of geriatric care for heart failure. Using shared decision-making strategies under the population health management approach could enhance the quality of care and reduce costly readmissions of heart failure, particularly for elderly patients.
Avoidable hospitalization or readmissions emerged as a critical issue in achieving better quality and lower cost of care, particularly related to older patients with chronic conditions [1]. A concerted effort has been made by the Centers of Medicare and Medicaid Services in the United States to encourage the identification of differential risks in readmissions due to chronic conditions such as heart failure. Similarly, care management strategies have been implemented in acute care hospitals for enhancing the delivery of integrated care. Therefore, care management for chronic conditions can be extremely critical in shaping the process of disease management and outcome improvement activities for the elderly [1]. However, little empirical evidence exists in the scientific literature that shows what works and what does not work for patients with these conditions. Artificial intelligence applications with machine learning may be a source for identifying workable solutions, but its development is plagued by the critical issue of lack of theoretical guidance in framing pertinent research questions or testable hypotheses. Thus, the reliance on an inductive or problem-solving approach offers little generalizability or conclusive evidence to achieve sustainable solutions for chronic disease management. This study contributes to the body of knowledge-centered in patient-centric factors or human-factor principles within the Population Health Management Framework that may directly or indirectly affect hospitalization and rehospitalization of heart failure patients.
Objectives of the Study
The human factors may play a moderating or a mediating role influencing HF hospitalization or rehospitalization. However, no clinical trial studies for HF have examined the relevance of human factors as major effects or intervention factors that may be potential enhancers for better HF outcomes. The purpose of this study is two-fold: 1) to design the algorithm through performing regression analysis of both main effects and interaction effects of selected human-factor principles on the propensity for HF hospitalizations, and 2) to examine how the self-care principles, such as choice/efficacy, restfulness, healing environment, activity, trust, interpersonal relationships, outlook, and nutrition, may reduce heart failure (HF) readmissions. The systematic review and meta-analytic approach are used to generate a theoretically relevant and empirically validated self-care management decision support protocol for HF.
Related Research
Population Health Management Approaches
In an era of healthcare delivery value-based system is critical. Additionally, there is a greater need for containing avoidable hospitalization or readmission. Henceforth, as corroborated by Nielsen et al, [2] population health management emerges as a practical approach to improve quality and reduce costly hospitalization of the chronically ill patient population [2]. The general principles may include the following, as cited in the book entitled “Population Health Management for Poly Chronic Conditions: Evidence-Based Research Approaches [1]:
The relevance of Human-Factor Principles in Predicting HF Readmissions
Eight human factors principles are commonly believed to affect health care outcomes of heart failure patients. They are also considered as enhancers for better patient care outcomes. However, no randomized controlled trial (RCT) studies have considered the human factors as intervention factors in the investigation of clinical outcomes [6].
Research Questions
Three research questions formulated under the population health management framework with an emphasis on the human-factor principles are stated as follows:
Question 1. What is the specific human-factor principles observed in the literature to contribute to the variability in HF readmissions?
Question 2. What are the important main effects and interaction effects of these human-factor principles in the analysis of the readmission risk?
Question 3. What is the relative importance of each human-factor principle that could be incorporated into risk reduction strategies for enhancing self-care management of heart failure?
Material and Methods
Systematic Review and Meta-Analysis Procedures
The literature review coupled with meta-analysis is a powerful and efficient approach to summarize the results. This is also called the approach of employing the epidemiology of results for determining the relevance of predictor variables for readmissions. By following the report procedures specified by Moher et al. [12], a systematic review and meta-analysis of HF hospitalizations were performed. The study team selected appropriate keywords relevant to the 1) independent variable of hospitalization and treatment, 2) the moderating variable of care management principles, 3) the dependent variable of readmission, and 4) the disease of HF to conduct searches in nine databases. Databases searched included CINAHL, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, ERIC, MedLine, PubMed, PsycInfo, Science Direct, and Web of Science. Only prospective studies associated with HF hospitalization and readmissions, published in English, Chinese, Spanish, and German journals between January 1, 1990, and August 31, 2015, were included in the systematic review. Data were extracted from the studies by use of a machine learning algorithm. In the meta-analysis, data were collected from studies that measured HF readmission for individual patients.
Statistical Analysis and Modeling
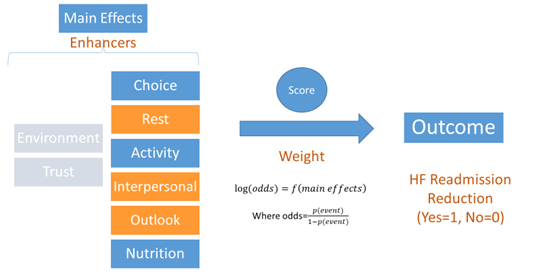
Figure 1 presents a logistic regression model with eight specific human-factors or principles as predictor variables or major effects for HF hospitalization (dependent or outcome variable).
Interaction effects of these eight factors are also empirically examined in the analysis. Detailed regression parameter estimates are openly available upon request from the corresponding authors.
Decision Support System Design and Validation
Given the present scenario of data acquisition and its transformation into information, knowledge, and wisdom; it is important to note that care management can be considerably improved using electronic data collection implemented using different methods. One of the key challenges here will decipher the most needed critical information from different data sources available on the cloud and through other means. It is important to note that this data will be available in different formats such as natural language text, relational database records, semi-structured data available as XML and JSON, and many other such formats. This implies that any research conducted must identify the nature of information along with the associated variables needed for research [13]. Here it is important to mention that this is the first key challenge in the design and validation of the required intervention.
The 2nd key challenge will be the development or synthesis of required decision support algorithms that will use the data gained. It is important to note that the application of ontologies might be critical in representing information that presents a myriad of complexities. In this strategy, we follow the rule stated by Herbert Simon [14] that complexity takes the form of hierarchy. While using an algorithm for decision support the stakeholders must also consider the inherent bias that can result from original sources as described by Gurupur and Wan [15]. Using appropriate knowledge structures to represent the recommendations made by the decision support system is also a necessary matter that needs thorough assessment. When using machine learning methods, the stakeholders must take into consideration the fact that knowledge structures can be constantly improved with the emergence of newer forms of knowledge.
Results
What are the specific human-factor principles as observed by care management enhancers in the available literature to contribute to the variability in HF readmissions?
A systematic review and meta-analysis of clinical trial studies on heart failure hospitalization have yielded positive proof of the beneficial effect of specific care management strategies that may alter patients’ knowledge, motivation, attitude, preventive practice, and outcomes. Figure 2 summarizes the numbers of selected review articles that identify important contributing human-factor principles to explain the variability in HF rehospitalization.
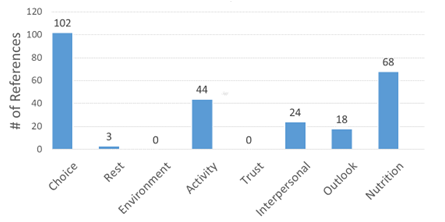
The relevance of human-factor principles (i.e., the eight factors such as choice, restfulness, healing environment, activity, trust, interpersonal relation, outlook, and nutrition) influencing HF readmissions has been examined by a systematic review of clinical trial studies that appeared in scientific journals. Of the total of 259 RCT studies reviewed, the frequency of human-factor principles cited is presented in Figure 2. The largest number (102) of RCT heart studies is involved with choice or self-efficacy, followed by nutrition (68) and activity (44). Two principles such as outlook and healing environment are not found from the review of RCT studies. The possible reasons for the lack of citations for these two factors are related to 1) a limited attention to outlook and healing environment as enhancers in care management or clinical studies; and 2) clinical studies centered in medical procedures or therapeutics, not on health educational interventions in earlier RCT studies.
What are the important main effects and interaction effects of these human factor principles in the analysis of readmission risks?
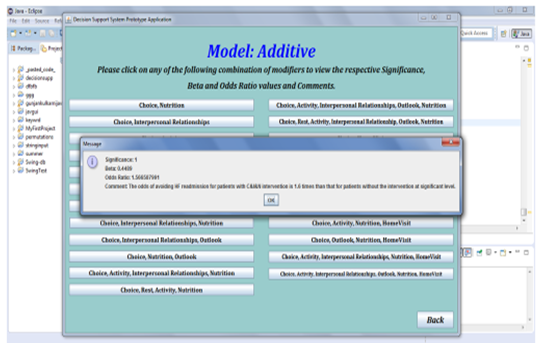
The regression analysis results indicate that an intervention involving six of the eight human factor principles may lower an individual HF patient’s probability of not being readmitted. Participants in interventions involved with human factors that incorporated single or combined principles were 1.4 to 6.8 times less likely to be readmitted. Interpersonal Relationships and Outlook Interventions have no statistically significant effect on the reduction of HF readmission. Furthermore, an additive model with the application of choice, interpersonal relationship, and nutrition together would yield a regression coefficient of 0.442, with an odds ratio of 1.566 (Figure 3).
Interaction effects are also examined in the analysis. Statistically significant interaction terms include 1) choice* interpersonal relationships*nutrition, and 2) choice*outlook*nutrition can significantly reduce the risk for HF readmission.
What is the relative importance of each human-factor principle that could be incorporated into risk reduction strategies for enhancing self-care management for heart failure?
The logistic regression analysis of the risk of being readmitted for heart failure to a hospital reveals that not all care management or self-care enhancers have an equal amount of influence on readmissions. For instance, rest intervention can significantly reduce HF readmission. The odds of reducing HF readmission with rest intervention is about 13 times more than that without rest intervention. Detailed statistical estimation results and algorithms could be obtained from authors at the request.
Discussion
The systematic review-meta-analysis approach to HF readmissions has helped identify the relevance of six out of eight human-factor principles as enhancers for reducing the risk of HF readmissions. In descending frequency order, choice or self-efficacy, nutrition, activity, interpersonal relationships, outlook, and restfulness are among the self-care principles identified while healing environment and trust were not identified in any of the 259 studies reviewed. A regression analysis of the human factors singly and in combination supported a 1.4 to 6.8 reduction in risk of HF readmission and revealed that not all self-care principles are of equal influence.
These results could be used to develop focused shared decision-making strategies to enhance the quality of care and reduce costly readmission of HF. As such, based on the odds ratio computation in logistic regression results, we may design a clinical decision-support system to guide the implementation of human-factor principles. Evaluation research is then designed coupled with the cloud-based data collection system to enhancing clinical practices for reducing HF readmissions.
Implications, Limitations, and Future Research
Implications and Contributions
Specific contributions of this study include the following:
Limitations
It is important to note that there are three specific limitations of the patient-centric strategy employing only human-factor principles in the population health management approach. First, potential biases may be generated by a disciplinary focused investigator who will solely rely on personal determinants of healthcare for artificial intelligence and research [15]. Alternatively, a transdisciplinary approach that incorporated both micro-and macro-level predictors in the design of predictive analytics may help to identify synergistic effects of personal, organizational, and ecological factors on care management improvement in the future. Second, a healing environment and design in healthcare may be an essential part of the care plan and assessment development. Thus, heart failure readmissions as a global health problem can be better examined and understood from an integrated perspective to guide the design and evaluation of artificial intelligence applications for chronic care. Third, the current measure of each human-factor principle is based on a binary or dummy variable. Thus, the intensity of the human-factor principle cannot be ascertained. Thus, the variability in employing a human-factor principle cannot be demonstrated by a dichotomized predictor variable.
Future Research
For solidifying the theoretical import of the eight human-factor principles, we need to develop more precise and quantitative measurements for these principles. Ideally, the adoption of an analog scale with a potential range from 1 to 100 points for each theoretical construct is imperative for measuring the degree or intensity of a human factor's influence on the variability in care management. Furthermore, it is desirable to form multiple indicators to reflect their relevance to a latent variable.
In the future, a practical patient decision support system could be redesigned and improved that is based on important human-factor principles, as part of patient-centric care, coupled with a cloud-data system to capture future observations of the effects of intensity and dosage of each self-care management intervention for HF patients (Figure 4). Furthermore, the research has uncovered how the risk-reduction approach is feasible and sustainable for artificial intelligence-based applications that will incorporate a shared decision-making approach. Furthermore, new data collected could be used to validate the risk reduction estimates generated from the prior investigation. By employing variant multivariate modeling techniques (e.g., artificial neural-network analysis, support vector regression, and other deep learning methods), the clinical decision support system could be further evaluated and amended (16).

Conclusion
Based on the principles of population health management for chronic conditions [1], clinical interventions with human-factor principles are suggested that may reduce readmissions among HF patients. The risk-reduction strategies for readmissions could be formulated and empirically validated in regression analysis. For the future investigation of HF hospitalization or rehospitalization, an integrated perspective, encompassing micro-and macro-determinants of healthcare outcomes for heart failure as noted in previous research [1], is a promising theoretical framework to guide the development of predictive analytics and the implementation of a viable and practical decision support system for enhancing care management for HF. Ideally, a comprehensive system framework, encompassing factors such as the governmental readmission policy [17], use of health information exchange [18], organization change strategies [19], implementation of practice guidelines [20] and application of behavior change interventions [21], could be used to conduct predictive modelling of determinants of hospital readmissions. Furthermore, the design and evaluation of patient-centric care coupled with a cloud-based data collection mechanism may enable us to conduct a large-scale prospective study on human factors influencing care management and outcomes. Furthermore, multivariate modeling techniques, such as multi-level analysis, could help delineate the relative effects of personal and contextual predictors on the rehospitalization of HF patients. By identifying a high-risk patient group and applying relevant human-factor principles as care management enhancers for heart failure or other targeted chronic conditions, the population health management and research could generate systematic information and knowledge about important determinants of health [23] and healthcare differentials [24]. The shared decision-making strategies [25] coupled with the use of artificial intelligence research [26] under the population health management approach could then be developed and implemented to enhance the quality of care and reduce costly readmissions of heart failure.
Author Notes: Conceptualization, T.W. and V.G.; methodology, T.W., B-L.W; software, V.G.; data processing and modeling, B-L.W and S.M.; systematic review, T.W., V.G., B-L.W; writing, T.W., V.G.; editing and proofreading, T.W., V.G., B-L.W., S.M. All authors have read and agreed to the published version of the manuscript.
Acknowledgments: The authors sincerely thank the editor and reviewers who have contributed to the fruition of this article.
Declaration of conflict interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding: None.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
