
Research Article | DOI: https://doi.org/10.31579/2768-2757/021
*Corresponding Author: Yansong Xu, Emergency department, the first affiliated hospital of guangxi medical university, Nanning city, China.
Citation: Y Xu, Z Liang. (2021) A novel model for predicting the death risk of severe traumatic brain injury during hospitalization. Journal of Clinical Surgery and Research. 2(3); DOI: 10.31579/2768-2757/021
Copyright: ©2021 Yansong Xu, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2021 | Accepted: 22 July 2021 | Published: 26 July 2021
Keywords: traumatic brain injury; death risk; prediction model
BACKGROUND: Patients with severe traumatic brain injury (sTBI) often presents with extracranial injuries, which may contribute to fatal outcome. The aim of this study was to construct the best death prediction model for sTBI and provide a feasible basis for early prognosis.
METHODS: A retrospective study from the First Affiliated Hospital of Guangxi Medical University from January 2012 to September 2020 was performed. Relevant risk factors at admission and record survival were collected at discharge. Logistic regression was used to establish a death prediction model. The performance of the model was predicted by fitting goodness test and calculating the area under the ROC curve (AUC). The DCA curve was used to show the net benefit rate of patients.
RESULTS: Of the 190 patients with sTBI, 91 died during hospitalization, with a mortality rate of 47.8 percent. Pupillary dilation, occipital lobe injury, SAH, cerebral hernia, and APACHE II score could predict the probability of death alone, with AUC of 0.636, 0.595, 0.611, 0.599 and 0.621 respectively. The AUC of death prediction for patients with sTBI was 0.860, and its sensitivity and specificity were 88.60% and 81.60%. The calibration and decision curve analysis (DCA) were conducted to validate the performance and clinical value of the novel model.
CONCLUSIONS: The clinic-radiomic model incorporating both clinical factors and radiomic signature showed good performance for mortality risk prediction of sTBI. The predictive model can identify sTBI with high sensitivity and can be applied in patients with sTBI.
TBI is a critical global public health problem. The incidence of TBI is increasing, and it ranks the first in the morbidity and mortality after injury [1-3]. In particular, sTBI has high mortality and disability rates, which has been the focus of clinical attention not only on treatment but also on adult death risk prediction [4]. Moreover, accurate determination of the prognosis is crucial for the practitioners, in order to optimize and personalize treatment strategies. There is a degree of uncertainty in clinicians' expectations of patient outcomes,and prognostic models can help improve these expectations by providing probabilities of specific outcomes. Compared with the experience of physicians to judge the prognosis of patients, objective prognostic models would be able to give more accurate projections about specific variables such as number of hospitalizations and deaths. At present, the predictors of mortality modules used are Glasgow Coma Scale (GCS), APACHE II and Sequential Organ Failure Assessment (SOFA) scores. And in our view, such estimates introduce a methodological innovation, whereby deaths among untreated patients are used to estimate the risk of death for the treated group if they had remained untreated. GCS provides an objective recording of the state of consciousness of a person, which is the only variable referring to brain function in the APACHE II score. APACHE II score was primarily designed to predict mortality in ICUs. SOFA is originally created for sepsis, but their quality is now used in other medical conditions. The famous models: the IMPACT model and the CRASH model were weighted towards mixed TBI (moderate and severe TBI) [5, 6]. But these models mainly used postoperative parameters to evaluate the prognosis of patients; Moreover, all the above models lack imaging parameters. Therefore, there is a strong need for prognostic signatures which are more efficient, more and easier to calculate for clinicians and preoperative patients in emergency department. Patients with mild to moderate TBI often had inaccurate GCS scores due to sedation and labor medications. Therefore, patients with sTBI were selected as the research objectives. The author works in the emergency department of the largest general hospital in Guangxi province, and undertakes prehospital and in-hospital emergency rescue, but our hospital had not yet formed a set of sTBI death risk prediction model. Risk models are important to help clinicians to provide reliable information to patients and relatives. Due to the differences in economic reasons and social concepts, the vast majority of people find it is difficult to accept that patients still cannot live on their own after several months of treatment. In China, the family members of patients are more concerned about whether the patients can have a high-quality survival, because the lack of self-care ability will consume more family income and increase the pain of family members. It is particularly important to construct a risk model of death from traumatic brain injury suitable for emergency department, which can not only assess the risk of death of patients in advance, but also help doctors to allocate medical resources equitably. To this end, this study systematically analyzed the relevant risk factors at admission, and expected to establish a novel model to more accurately predict the risk of death.
Study population from 2012 to 2020, the basic information of patients with sTBI were obtained through our hospital's HIS system, and the imaging results were inquired according to the PACS system. The study was approved by the ethics committee of First Affiliated Hospital of Guangxi Medical University. Informed consent from patients were waived for this retrospective study. The inclusion criteria are as follows: ① Patients with sTBI over 18 years of age. ② Patients suffering from sTBI without other injuries. ③ GCS score<8 at the time of admission. ④ Patients were diagnosed by CT or MRI in emergency department. ⑤ The survival status at discharge.The main outcome was inpatient mortality. Subjects who meet any of the following exclusion criteria will be excluded from participation in the study. ① A death occurring within 24h of admission. ② Patients did not suffered from hypertension, heart disease and diabetes at admission. ③ Those patients with incomplete clinical information. ④ Forgoing medical care for economic reasons.
Baseline characteristics including age, sex, GCS,endotracheal intubation or not, etc.; The vital signs were recorded at the time of admission, such as temperature, pupillary dilation, respiratory rate, heart rate, systolic blood pressure, etc.; After admission, blood samples were obtained within 24h, including creatinine, white blood cell count (WBC), platelet count (PLT), hematocrit (HCT), etc.; In addition, the APACHE II score (within 24h of ICU admission) were registered. Outcome in hospital was recorded as dead or alive at discharge.
Nomogram model performance was validated using internal validation by examining calibration. Final model was internally validated using bootstrapping resampling of the construction data set (with 1000 bootstrap samples per model) to obtain optimism corrected discrimination via the concordance index for survival data and calibration plots. In internal calibration plots, points parallel to the reference line would indicate similar predicted effect of the nomogram covariates in the development set. DCA was used to evaluate the clinical usefulness of the models.
Baseline characteristics
After rigorous screening, a total of 190 patients were enrolled, including 154 males and 36 females. The mean age was (46.2±18.0) years. Ninety-one of these patients died, with a mortality rate of 47.8 percent.
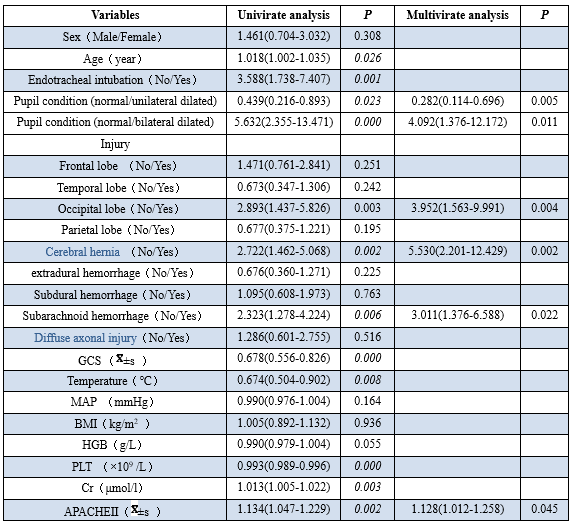
Univariate and Multivariate logistic regression analysis
This study identified the following parameters impacting survival: Age(p=0.026), Endotracheal intubation( P=0.001), GCS(P=0.000), Temperature (P=0.008), PLT( P=0.000), CR(P=0.003), Pupillary dilation(P=0.000), occipital lobe injury( P=0.003), SAH( P=0.002), cerebral hernia( P=0.006) and APACHE Ⅱ score (P=0.002) (Table 1). Next, all the factors with a p value less than 0.05 were involved in multivariate logistic analysis. Finally, pupillary dilation, occipital lobe injury, SAH, cerebral hernia and APACHE Ⅱ score retained their statistical influence on survival (all p<0>
SPSS 26.0 software and R 3.1 language were used to calculate the independent factors affecting death The predicted risk of mortality for each patient was calculated according to the following equation: Logit(P)=- 2.053- 1.736 x (unilateral pupillary dilation) to 3.088 x (bilateral pupillary dilation) + 1.364 x (occipital injury) + 1.663 x (cerebral hernia ) + 1.112 x (SAH) + 0.150 x (APACHE Ⅱ score). Graphic interpretation (The basic data of the patient no. 5): SAH (No), cerebral hernia (Yes), occipital lobe injury (Yes), dilated pupil (bilateral), APACHE (15 points). Each parameter corresponds to a point at the top of the graph, the sum of all points corresponds to the total score at the bottom, and finally corresponds to the risk probability at the bottom column (Figure 1). The AUC of death warning score predicting the death of critically injured patients was 0.860. The sensitivity and specificity of the model were 86.6% and 81.6% respectively (Figure 2). The AUC of critically injured patients predicted death by death warning score was the largest, which was significantly higher than the predictive value of other indicators (Table 2). Moreover, calibration plots indicated that in comparison with an ideal model, the nomogram had a similar performance (Figure 3). DCA was applied to evaluate the performance of predicting mortality risk of sTBI (Figure 4). The novel model had greater net benefit than individual indicators at any probability.





Figure 4: The DCA curve.
sTBI involves complex pathophysiological mechanisms, which is unquestionably the leading cause of mortality in China [7]. It is estimated that half of the world's population will live with one or more TBIs in their lifetime [8]. Early management of patients with sTBI has always been a thorny issue. Patients with sTBI received active surgical treatment in time, but the high mortality rate made doctors and patients' families dissatisfied. Overall, present studies strengthen -ed the idea that patients with sTBI had poor prognosis and high mortality. A recent multicenter cohort study demonstrated that the overall mortality of sTBI was 27% [9], which was similar to the reported rates in Europe and North America [10, 11]. And most deaths after sTBI were due to withdrawal of lifesupporting measures, often based on perception of unfavorable chances of meaningful neurologic recovery [12, 13]. Therefore, how to make a scientific judgment on the prognosis of this kind of patients is particularly important. The results of this research supported the idea that there were many factors affecting the prognosis of patients with sTBI. 21 clinical variables were included in this study, and the results showed that the pupillary dilation (including the unilateral and bilateral), occipital lobe injury, SAH, cerebral hernia and APACHE Ⅱ score were the independent factors of death in patients with sTBI. The death risk model had an AUC of 0.860, which was significantly higher than the predictive value of any indicator. According to the analysis of the model, doctors take timely measures which can effectively and quickly reduce secondary brain injury. APACHE Ⅱ score related observation index (heart rate, breathing, red blood cell pressure, etc.), may help reduce the mortality. There is a certain relationship between pupil condition and consciousness disorder, which can judge the prognosis of patients. Pupillary dilation was a major factor of decision making. Dilated pupils on one side or dilated on both sides indicate a critical condition, for these patients, mannitol treatment was used as a control of osmotic pressure. No reduction of bilateral pupil after mannitol injection indicated severe brain stem compression and poor prognosis. The GCS score remains a valuable tool to indicate prognosis and especially for most well-validated index of overall neurologic injury severity [14, 15]. With a GCS>4 score, pupil dilation was an important basis for stratification, with dilated pupil on one side accounting for 81.2% and dilated pupil on both sides accounting for only 47.4%, indicating that the change of pupil was related to death [16]. APACHE Ⅱ scoring system is now the most commonly used in critical care clinical scoring system, which has certain value for the forecast of trauma patients died. In critically ill patients, APACHE Ⅱ score < 10> 14.5, the mortality rates closed to 50%, but the death rate was as high as 80% when the APACHE Ⅱ score > 20 points. APACHE Ⅱ scoring system is very complex and affected by many factors. The admission APACHE II model, as with other ICU scoring systems such as the APACHE III model, needs an accurate diagnosis to accurately predict the hospital mortality. Especially, history-taking in the early phase of sTBI patients was typically difficult. The scoring system records the worst clinical test data, it is affected by a variety of factors and is difficult to carry out, hence using APACHE II score to predict the prognosis of patients will be more difficult in the emergency department. GCS might be a most significant indicator in APACHE II scoring. It has been reported that the APACHE II score was more accurate than the GCS score for predicting late mortality of patients with sTBI, although the APACHE II score may be less accurate than the GCS score to predict early mortality, which was similar to this finding[17]. The complex pathophysiological process after TBI and its precise regulatory mechanism has not been fully understood, however, it is assumed that the process of TBI can be divided into primary brain injury and secondary brain injury. After CT era, due to its ability to demonstrate the nature, sites, and multiplicity of TBI [19]. Hence, it provides an objective and invaluable evaluation of structural brain damage following head injury. Similar to other results [20], several individual CT features, such as occipital lobe injury, SAH and cerebral hernia were associated with adverse outcomes after sTBI in this study. Multivariable logistic regression model of this research found that Characteristic of single CT to predict death probability was unsatisfactory, the risk factors to predict the AUC of death were: 0.636 (pupil dilation), 0.595(occipital injury), 0.599 (subarachnoid hemorrhage) and 0.611 (cerebral hernia) and 0.621 (APACHE Ⅱ) respectively. The optimization prediction probability model AUC was 0.860, which significantly improved the sensitivity and specificity. It should be noted that although predictive tools can assist clinicians in determining patient prognosis, predictive tools cannot completely replace clinicians' judgment. In the process of using the prediction tool, accurate judgment should be made according to patients' specific conditions and doctors' own experience. The strengths of the study included the in-depth analysis of the risk of death in patients with sTBI, which provides a theoretical basis for further treatment decision and medical resource allocation. A number of limitations need to be noted regarding the present study: 1. The neurological function and self-care conditions that patients were most concerned about need to be further improved. 2. This study is a retrospective study, with certain design deviation, which needs to be further analyzed through prospective data. 3. Clinical physical examination can partly reflect the severity and prognosis of the disease, but the deterioration or improvement of micro-circulation in vivo will first be reflected in the change of some biochemical indicators. Due to limited conditions, relevant data such as cell metabolites and serum markers were not collected for inclusion in the model in this study. 4. This study tested the internal authenticity of the model, but lacked the verification of external authenticity. We know that good clinical benefits need to be demonstrated through a comprehensive evaluation of interventions, preferably by designing multicenter RCTs. It intends to further collect data to verify the applicability of the model. After continuous improvement, the early prediction model for the prognosis of sTBI has achieved relatively high prediction ability and accuracy. Although no universally applicable clinical guidelines have been formed, it has been able to provide great help for emergency departments, neurosurgeons and patients' families in treatment decision-making.
From this retrospective study, the predictive model can identify sTBI with high sensitivity and can be applied in patients with sTBI. However, a good clinical prediction model requires external validation and RCTs. We intend to gradually improve the above work in the next step Funding: None. Ethical approval: Not needed.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
Yansong Xu proposed and wrote the first draft. All authors contributed to the design and interpretation of the study and to further drafts.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
