
Research Article | DOI: https://doi.org/10.31579/jcitr.2018/002
*Corresponding Author: Ostap Espel, Department of Radiology, Ukraine.
Citation: Ostap Espel. A New System for Outcome Measure of Atelectasis in Studies of Cardiac Surgery, J. Stem cell Research and Therapeutics International. Doi: 10.31579/jcitr.2018/002
Copyright: © 2018 Ostap Espel. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 03 August 2018 | Accepted: 14 August 2018 | Published: 20 August 2018
Keywords: Atelectasis, cardiac surgery, cardiopulmonary bypass, chest x-ray, outcome measures
Background: Pulmonary atelectasis is common following sternotomy for cardiac surgery. The degree of atelectasis present on chest x-ray has been used to assess efficacy of interventions designed to reduce atelectasis, however radiological atelectasis scoring systems used may exaggerate the clinical effect of atelectasis in these patients. We have produced an alternative scoring system that seeks to correct this problem and this study aimed to evaluate this.
Methods: Following ethics approval we retrospectively selected 50 consecutive patients admitted to the intensive care unit following cardiac surgery. Electronic copies of chest x-ray taken on return to the intensive care unit, on day 1 and day 3 postoperative were obtained and corresponding details of oxygenation were collected from patient records. Anonymised chest x-rays were scored, using both the old and new scoring system, by a radiologist blinded to the clinical data. Chest x-ray scores were compared with oxygenation indices at the time of chest x-ray. Day 1 scores were also assessed for their ability to reflect day 3 oxygenation indices and supplemental oxygen requirement.
Results: The new score demonstrated better ability to detect atelectasis on chest x-ray and better specificity than the old score when comparing the chest x-ray findings with the clinical oxygenation status of the patients. The new score also performed better at predicting day 3 oxygenation status from the day 1 chest x-ray.
Conclusions: This new scoring method performed better as an outcome measure for atelectasis in studies of patients following cardiac surgery. It may also better identify patients who require ongoing administration of supplemental oxygen on postoperative day 3.
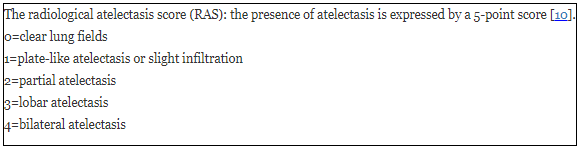
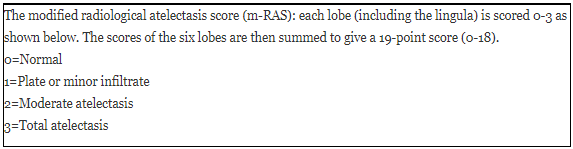
Postoperative complications following cardiac surgery increase mortality, morbidity and costs [1]. One major cause of postoperative respiratory complications is atelectasis [2]. The development of atelectasis following general anesthesia and cardiac surgery is almost inevitable [2,3] and has been described as present in most patients with an incidence of around 90% of cardiac surgical patients [4,5]. Atelectasis impairs oxygenation, worsens lung compliance, augments the development of lung injury and increases pulmonary vascular resistance [6]. It may also be associated with postoperative infective complications such as pneumonia, [7] and may be resistant to simple techniques employed to improve lung function such as patient positioning, physiotherapy and incentive spirometry [3]. Ensuring adequate oxygenation and respiratory support is vital in the postoperative period; however there is little published evidence to guide clinicians in the objective selection and use of oxygen delivery devices [8]. We are conducting a large scale randomised controlled trial to assess the effect of prophylactic nasal high flow oxygen therapy (NHF) using the Optiflow™ system (Fisher & Paykel Healthcare, New Zealand) on postoperative oxygenation in cardiac surgical patients [9]. In order to evaluate the hypothesis that NHF can improve pulmonary function and reduce atelectasis we required a validated atelectasis scoring system. Currently there are few scoring systems for reporting atelectasis from chest x-rays [10-12]. The Radiological Atelectasis Score (RAS) has been used to describe the degree of atelectasis in postoperative patients [10]. We felt this score may over-emphasise subtotal atelectasis in the lower lobes and furthermore it does not attribute any extra weight if there is additional atelectasis in the middle or upper lobes. Therefore we have designed a new scoring system to differentiate the severity of atelectasis in patients with multi-lobar involvement.
The aims of this study were to evaluate a proposed atelectasis scoring system against a previously published scoring system in a group of patients following cardiac surgery; to assess the ability of the two scores to reflect the oxygenation at the time the chest x-ray (CXR) was taken; and to assess the ability of the two scoring systems to reflect oxygenation indices on subsequent days.
Fifty consecutive patients' clinical records were selected for retrospective review. These patients were selected by the principal investigator and were admitted to the intensive care unit (ICU) during the month of January 2010. Inclusion criteria were: aged 18 years or more, received median sternotomy for cardiac surgery with cardiac bypass, weaned from mechanical ventilation and extubated within eight hours post-op, length of stay in ICU less than 24 hours, and only required simple nasal prongs or face mask for oxygen delivery following extubation. Ethical approval for the study was obtained from the Northern X regional ethics committee. Due to the retrospective observational nature of the study, the need for informed consent was waived.
Oxygenation indices
Clinical details of oxygenation on post-operative day 1 and 3 were obtained from the patients' records and electronic copies of anteroposterior CXR taken on return to ICU (baseline), day 1 (d1) post-operative and day 3 (d3) post-operative were downloaded and stored on compact disc for review by the radiologist.
On day 1 all patients had arterial blood gas measurements available and the partial pressure of oxygen (PaO2) and fraction of inspired oxygen (FiO2) closest to the time the CXR was taken were recorded, along with pulse oximetry readings. Arterial blood gas measurements were not available on patients on day 3, so pulse oximetry was used to measure peripheral oxygen saturation (SpO2) value. Oxygen requirement at time of CXR was recorded. From these data the PaO2/FiO2 (P/F) and SpO2/FiO2 (S/F) ratios were calculated. An S/F ratio of 445 was selected as a binomial outcome to distinguish patients either requiring oxygen or with SaO2 or SpO2<94% versus those with an SaO2 or SpO2≥94% on air.
Atelectasis scoring
The x-rays were scored using both the radiological atelectasis score (RAS) and a modified radiological atelectasis score (m-RAS) system by a single radiologist (Author DM) who was blinded to the oxygenation data and to the order in which the x-rays were taken by obscuring the date the CXR was taken (see box 1).
Data analysis
Data analysis was undertaken using STATA12 (StataCorp LP, Texas, USA) and Statistical Package R (R Development Core Team (2010). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0. For both the old and new scores the day 1 and day 3 CXR scores were also compared with oxygenation indices (P/F or S/F ratio) at the time of CXR. Day 1 scores were also assessed for their ability to characterize day 3 S/F ratios below 445 (An S/F ratio of <445 equates to any requirement for supplemental oxygen or SpO2<94% on air).
Fifty patients were included in this study. Baseline demographic data is presented in (Table 1).

On post-operative return to the ICU, 43 patients (86%) were determined to have some degree of atelectasis using both scoring systems. By day 1 the overall incidence of atelectasis was 86% using RAS and 98% using m-RAS. The incidence on day 3 was 98% using RAS compared with 96% using m-RAS. (Figure 1) shows the degree of atelectasis at return to ICU, day 1 and day 3 for the group. There was an approximately linear relationship between the RAS and m-RAS scores, but with m-RAS demonstrating a greater range of scores.
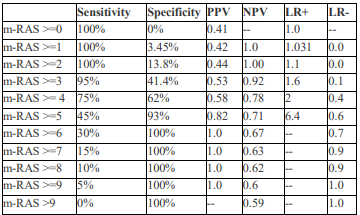
When comparing the scoring systems' ability to predict oxygenation status at day 3 from the changes seen on the CXR taken on day 1, the m-RAS performed better than the RAS; both scoring systems were more accurate in reflecting day 3 oxygenation status from changes seen on the day 1 CXR than on the day 3 CXR. The ability of day 1 x-ray to predict day 3 oxygenation is shown in (Table 2). This was the only significant result with a likelihood ratio of 0.1 for an m-RAS of 3.
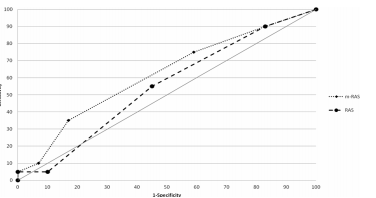
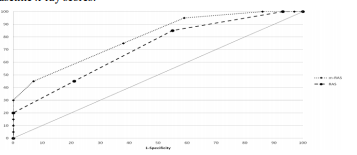
(Figure 2) shows the receiver operating characteristic (ROC) curves for using the two scores to predict whether the S/F ratio would be below 445 on day 3 using the baseline x-ray. The area under the curve for m-RAS is 0.62 and for RAS is 0.55. (Figure 3) shows the ROC curves for using RAS and m-RAS on day 1 to predict an S/F ratio <445 on day 3. The area under the curve for m-RAS is 0.79 and for RAS is 0.71.
When analyzing the oxygenation indices it was found that on day 3 41% of patients had an S/F ratio below 445, indicating either an ongoing requirement for supplemental oxygen therapy (n=10) or a measured SpO2 of ≤ 93% on room air (n=10). In the group still requiring supplemental oxygen, the average SpO2 was 94.3% (range 91-96%), while receiving an average FiO2 of 0.28 (giving an average S/F ratio of 330). Other data for the group not requiring oxygen but with SpO2 <94% is shown in (Table 1).
This study has evaluated a new system for assessing atelectasis on chest x-ray of patients following cardiac surgery. The overall incidence of atelectasis on return to ICU following cardiac surgery was found to be 86%. This is comparable with other studies in this population which have reported an incidence of 64% to 100% [13-15].
The m-RAS was developed to address perceived deficiencies when scoring atelectasis on CXRs of patients undergoing cardiac surgery. This study has demonstrated that day 1 m-RAS is more accurate than day 1 RAS in predicting poor oxygenation in postoperative cardiac surgical patients from their routine CXRs. We hypothesise that this improved predictive ability is due to the ability of m-RAS to better differentiate subtotal lobar atelectasis.
The selection of appropriate end-points for Phase II clinical trials is essential to robust study design but may prove problematic. Defining a clinically important end point in studies of critically ill patients is an important consideration in order to avoid poorly conceived clinical trials [16]. Whilst designing a study to investigate the effects of nasal high flow oxygen therapy on atelectasis in patients following cardiac surgery, [9] we were tasked with finding a suitable tool to measure, accurately, atelectasis on chest x-ray at various time points postoperatively. It was felt that published scoring systems may over-estimate the severity of subtotal bilateral basal atelectasis frequently seen following cardiac surgery, thus reducing the specificity of the scores ability to predict clinically important indices. Therefore, a system was designed to more accurately describe the degree of atelectasis formation recognizing changes throughout the whole lung and with the ability to differentiate between patients with bilateral changes affecting the lower lobes only and patients with more extensive changes. Other published trials have faced this problem too, describing inconsistencies in the way atelectasis is reported and the apparent lack of an adequately validated scoring system for assessment and reporting of atelectasis [12,14].
Previous studies differ in how atelectasis is perceived to affect oxygenation. One study found that hypoxaemia was not present in most patients who had demonstrated atelectasis, with only 4% being unable to maintain an arterial oxygen tension of 13.3kPa [14] while another reports that the presence of atelectasis coincided with a requirement for higher positive end expiratory pressure (PEEP) and FiO2 necessary to maintain oxygenation [17]. In this study it was found that the day 1 m-RAS was a good predictor of an S/F ratio of below 445 which would identify patients on supplemental oxygen therapy or those who had an SpO2<94% on day 3. This is a relevant and pragmatic clinical outcome for this group and reflects guidelines in the management of oxygen therapy in critically ill adults [18].
This study also demonstrated a difference in the temporal relationship between clinical signs (e.g. respiratory rate and oxygen saturations) and the changes seen on chest x-ray. This concept of a time-lag between clinical changes and CXR changes is well described. Clinical examination has been found to under-estimate the frequency of atelectasis and changes in temperature, heart rate and respirations are poorly correlated with atelectasis post cardiopulmonary bypass [14,19]. Changes in lung function have been described previously with evidence showing that pulmonary complications persist for around a week after cardiac surgery, with the most severe symptoms observed around the second post-operative day [20-22]. Increased elastance parameters following cardiac surgery with peak changes occurring around day two to three have also been demonstrated [22].
Limitations of this study
No assessment of atelectasis was performed on the preoperative chest x-ray, therefore the assumption is that there was no pre-operative atelectasis. Pre-operative CXR assessment has not been routinely performed in previously published studies either. One study took pre-operative x-rays and compared them to post-operative and found none at baseline but 8/35 had atelectasis post-operatively [22].
No other demographic or clinical data was collected. This study was performed purely to assess the degree of atelectasis on chest x-ray and to determine how this might predict oxygenation status post-operatively.
This study was designed as a retrospective study, thus potentially suffering from selection bias. However to minimize selection bias the protocol required the enrollment of 50 consecutive patients who met the inclusion and exclusion criteria chosen for this study who received routine postoperative oxygen therapy. They should therefore reflect the group that will be enrolled into the planned randomized controlled trial.
This new scoring method appears to be better suited as an outcome measure of atelectasis in studies of patients following cardiac surgery. It may also have some utility in discriminating patients who require ongoing supplemental oxygen on postoperative day 3, however further prospective studies are required to confirm this. We propose to use this modified scoring system as a secondary outcome in a randomised controlled trial investigating the use of prophylactic nasal high flow oxygen therapy after cardiac surgery [9].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
