
Research Article | DOI: https://doi.org/10.31579/2692-9406/117
1 Senior Consultant, Assistant Professor of Orthopaedics, 1st Department of Orthopaedics, Athens General HospitalG. Gennimatas, Athens, Greece.
2 Professor of Orthopaedic Surgery,Faculty of Medicine, University of Thessalia, Larissa, Greece.
*Corresponding Author: Konstantinos C Xarchas, Senior Consultant, Assistant Professor of Orthopaedics, 1st Department of Orthopaedics, Athens General Hospital G. Gennimatas, Athens, Greece.
Citation: Konstantinos C Xarchas, Zoe Dailiana (2022) A new combination of surgical techniques for the treatment of 1st carpometacarpal joint arthritis, J. Biomedical Research and Clinical Reviews. 7(1) DOI: 10.31579/2692-9406/117.
Copyright: © 2022 Konstantinos C Xarchas. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 25 March 2022 | Accepted: 25 April 2022 | Published: 18 May 2022
Keywords: surgical techniques; carpometacarpal; arthritis
Up till now, many different techniques have been used for the treatmentof 1st carpometacarpal (cmc) joint arthritis. Here we present a new combination of well- known techniques and surgical approaches that gave excellent results in a five year follow up.
Surgical techniques used for the treatment of 1st cmc joint arthritis include 1st cmc joint arthrodesis [1],1st metacarpal osteotomy [2],excisionof the trapezium with tendon interposition (known as the anchovy procedure) [3], excisionof the trapezium with ligamentreconstruction, tendon interposition (LRTI) [4], hematoma distraction arthroplasty (HDA) [5] and implant replacement [6].
We present a combination of hematoma distraction technique with interposition of a spacer from the distal part of the flexor carpi radial is tendon. Furthermore, the surgical approach used is a combination of Wagner approach for treatment of fractures of the base of the first metacarpal (Bennet etc.) [7] with the Trance FCR approach to the distal radius [8]. The former gives an excellent and more or less safe view for excision of the trapezium while the latter is equally efficient for lifting a small part of the distal flexor carpi radialis tendon. As an alternative, the longitudinal part of the incision can be replaced by a smaller one, positioned more centrally on the palmar surface of the wrist so that a Palmaris longustendon graft can be taken and used as a spacer instead of the FCR tendon. Both incisions can be used for simultaneous carpal tunnel decompression if needed.
During a time period of 12 years 20 patients suffering of 1st cmc joint arthritis have been treated with the technique we present. The mean follow-up time was 5 years (3-6).There were 13 women and 5 men (2 bilateral operations) all of them above their 40th year of age (40-82) All of them had an excellent pain relief and an improvement of their grasping ability of about 40%. This was below the healthy hand, but all patients were satisfied. Traumatic neuroma of a small branch of the radial nerve in one patient, was the only complication met and was treated by surgical exploration and cauterization. The stumps were then embedded in the radius.
Surgical Technique and Follow Up
Under general anesthesia and an arm tourniquet the upper limb is prepped and draped. A curved skin incision around the base of the first metacarpal is extended proximally on the line of the tendon of the flexorcarpi radials (Figure1).

Attention is then given to preserve the sensory radial nerve and it branches that may need to be carefully dissected. The longitudinal part of the incision is deepened through the fcr and the radial artery is usually not met (figure 2).

The trapezium is then excised-most of the times in one piece (Figure 3)
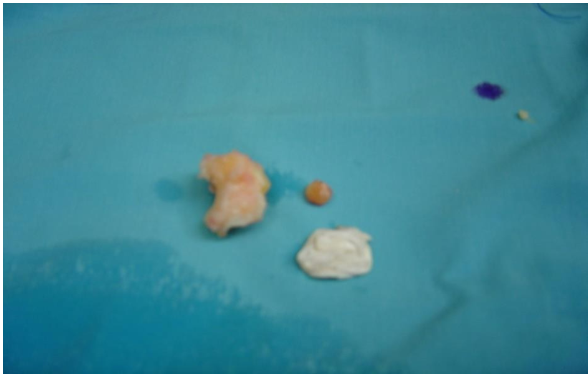
Taking care that the distal part of the fcr remains intact. The 1st metacarpal is then distracted and stabilized to the second one with a k-wire. Appropriate metacarpal distraction is verified with the c-arm (Figure 4).

and attention is then turned back to the fcr tendon. A longitudinal stripe of about 1/3 of the tendon’s width and 1/3 of its length is removed under direct vision, turned into a small ball with the use of an absorbable suture and put into the gap produced by the trapezium excision (Figure 5).

Finally, skin is closed and the hand put in a thumb spicapopsplint. Sutures are removed two, whereas the pin and spica six weeks postoperatively. A careful physiotherapy program is then commenced and the hand left
The method that we present offers an effective and safe approach for treatment of the first carpometacarpal jointarthritis of the hand.Low rate of complicationsand adequate pain relief,with improved graspingability of the hand, confirm its usefulness and we therefore propose it.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
